Bristol Myers Squibb's Opdivo Combined with Chemotherapy Achieves 49% Pathological Complete Response Rate in Neoadjuvant Treatment of Muscle-Invasive Bladder Cancer
Feb 18, 2020 14:54
CST Updated
14:54

Bristol-Myers Squibb
Biopharmaceutical and Nutritional Product R&D and Sales

February 18, 2020 News /BioonBIOON/ -- Recently, at the 2020 American ClinicalTumorA bladder cancer study presented at the Genitourinary Cancers Symposium (ASCO-GU 2020)Clinical TrialResults from BLASST-1 showed that Bristol-Myers Squibb’s anti-PD-1 therapy Opdivo (brand name: Opdivo; generic name: nivolumab) in combination with gemcitabine and cisplatinNeoadjuvant Therapy for Muscle-Invasive Bladder Cancer (MIBC)Patients Achieved Robust Efficacy:The pathological non-muscle invasive rate (PaR) was 66%, and the pathological complete response rate (pCR) was 49%.In the study, this combination therapy was safe, with no increased toxicity or mortality, and did not lead to delayed cystectomy or unexpected surgical complications. These results are highly encouraging, and long-term follow-up will further confirm its safety.
Shilpa Gupta, a study investigator and Associate Professor of Genitourinary Oncology at the Cleveland Clinic, stated, “Cisplatin-based neoadjuvant chemotherapy is associated with a pCR rate of approximately 30%. The survival benefit of neoadjuvant chemotherapy primarily occurs in patients who achieveTumorAmong patients with downstaged pathological grading. However, a considerable number of patients still experience recurrence, leading to early mortality. Therefore, there is a significant unmet medical need in this field to improve pathological response rates through novel combination therapies and biomarker-driven approaches for better patient selection.
Shilpa Gupta stated that prior studies of single-agent neoadjuvant immunotherapy for muscle-invasive bladder cancer have demonstrated benefits, as seen in the PURE-01 and ABACUS trials. The neoadjuvant immunochemotherapy regimen of Merck’s anti-PD-1 therapy Keytruda (pembrolizumab) combined with gemcitabine/cisplatin also showed activity in a Phase I/IIb trial. Opdivo has been approved for the treatment of patients with metastatic urothelial carcinoma who have experienced disease progression following platinum-based chemotherapy.
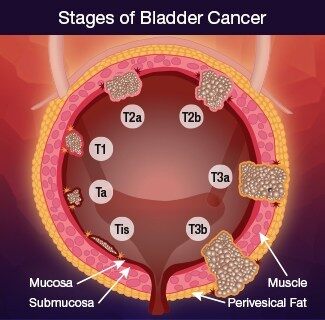
Patients in the BLASST-1 study had cT2–T4a N≤1 M0 disease, predominantly urothelial carcinoma, and were considered candidates for radical cystectomy. All patients were deemed eligible for cisplatin-based therapy, with a creatinine clearance threshold of ≥50 mL/min.
DiagnosisFollowing diagnosis of muscle-invasive disease, patients received four cycles of gemcitabine/cisplatin therapy. Cisplatin was administered at a dose of 70 mg/m² on Day 1 of each cycle (21 days per cycle). The decision to split the cisplatin dose was left to the investigator’s discretion. Gemcitabine was administered at a dose of 1000 mg/m² on Day 1 and Day 8 of each cycle (21 days per cycle) for a total of four cycles. Opdivo was administered at a fixed dose of 360 mg every three weeks on Day 8 of each cycle. Patients underwent cystectomy 6–8 weeks after completion of systemic therapy. Prior to study treatment, CT and fluorodeoxyglucose (FDG)-PET scans were performed, and tissue and blood samples were collected for relevant analyses. At the end of treatment, CT/FDG-PET scans were repeated, and tissue samples were collected. The primary endpoint was pathological response, defined as the rate of non-muscle-invasive pathology at the time of surgery.
This study enrolled 41 patients (63% male, 37% female) across three clinical centers, with a median age of 66 years (range: 45–82 years). Clinical staging was T2N0 in 90%, T3N0 in 7%, and T2–4N1 in 3%. Two patients (4.8%) had previously received bacillus Calmette-Guérin (BCG) therapy. Thirty-eight patients completed all four treatment cycles, two completed two cycles, and one completed only one cycle. All patients who received at least one cycle were considered evaluable. Forty patients underwent cystectomy; one patient withdrew consent after one cycle and was lost to follow-up but was included in the intention-to-treat analysis. All patients underwent cystectomy within 8 weeks after completing treatment.
Among the 27 patients whose tumors were downstaged to non-muscle-invasive status, 14 (51.8%) were downstaged to pT0, 2 (7.4%) to pT1, 5 (18.5%) to pTa, and 6 (22.2%) to pTis. The pathological complete response (pCR) rate was 49% (20 out of 41 patients), defined asTumorDownstaged to pT0 or pTis.
Of the 39 tumors, 15 (39%) tested positive for PD-L1. There was no correlation between PD-L1 positivity and response. Tumor shrinkage occurred in 10 of the 15 patients (67%) with PD-L1-positive tumors, compared with 17 of the 24 patients (71%) with PD-L1-negative tumors.TumorShrinkage.
Relief analysis by molecular subtype showed one case of claudin-lowTumor(characterized by high immune infiltration and basal marker expression) achieved a complete pathological response to treatment (pT0N0); another patient with the luminal infiltrative subtype (characterized by high stromal infiltration and moderate luminal marker expression) was a non-responder (pT3N2).
Gene signature scoring for 50 cancer hallmarks. In this case of claudin-lowTumorAmong the patients, those exhibiting “high immune marker activity” showed high expression of Immune 190, interferon-gamma (IFN-γ), interferon-alpha (IFN-α), and inflammatory markers. In contrast, this case of luminal invasive subtype disease demonstrated strong angiogenic activity and low proliferation.
In the study, most treatment-related adverse events (AEs) were attributed to chemotherapy. Most hematologic toxicities were consistent with those observed with gemcitabine and cisplatin. The majority of these were Grade 1/2.Anemia, neutropenia, and thrombocytopenia. A total of 10 patients (24%) experienced anemia, 20 (48%) had neutropenia, and 13 (31%) had thrombocytopenia.Grade 1/2 fatigue occurred in 60% of patients, and grade 1/2 nausea in 70%. Elevated levels of alanine aminotransferase (ALT) and aspartate aminotransferase (AST) were observed in 24% of patients. Acute kidney injury was reported in 6 cases (14%), all of which were grade 1/2 except for one case.One case of immune-related adverse event was rash, one case was hypothyroidism, two cases were lymphadenitis (both in patients with complete response, biopsy confirmed benign), and one case was Guillain-Barré syndrome.
Shilpa Gupta stated, “Ongoing biomarker analyses will help identify predictors of response and resistance to chemoimmunotherapy in muscle-invasive bladder cancer. The Phase III ENERGIZE trial is ongoing.”(NCT03661320), these results will be confirmed.”(BioValley Bioon.com)
Original Source: ASCO-GU 2020: Abstract 439