

On March 26, BMS announced that the FDA had approved Zeposia (ozanimod) for marketing. It is administered orally once daily at a dose of 0.92 mg for the treatment of adult patients with relapsing forms of multiple sclerosis (RMS), including clinically isolated syndrome, relapsing-remitting multiple sclerosis (RRMS), and active secondary progressive multiple sclerosis (SPMS).
Zeposia is currently the only sphingosine-1-phosphate receptor (S1PR) modulator that does not require genetic testing prior to prescription or health monitoring according to the label after the initial dose. Before initiating treatment with Zeposia, all patients with multiple sclerosis (MS) must undergo a physical assessment, including lymphocyte count, electrocardiogram (ECG), liver function tests, and a review of medication history (including vaccination status). Patients with uveitis or macular edema also require an ophthalmologic evaluation. Upon initiation of Zeposia therapy, dose titration is required, gradually increasing to the maintenance dose of 0.92 mg/day; transient bradycardia and atrioventricular conduction delays may occur during this process. If a dose is missed during the first two weeks of initial treatment, the patient must restart the dose titration.
Chemical Structure of Ozanimod
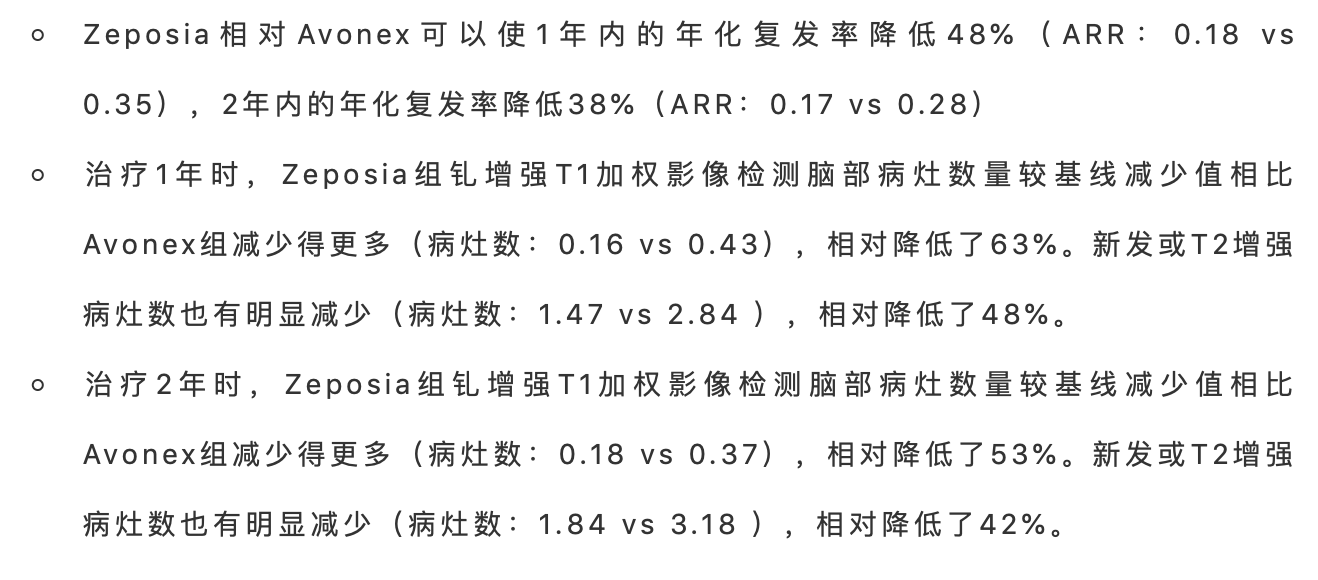
This FDA approval is primarily based on data from the largest head-to-head pivotal Phase III SUNBEAM study (n=1,346) conducted to date in patients with relapsing multiple sclerosis (MS), and Part B of the RADIANCE study (n=1,320), involving a total of more than 2,600 adult patients. Both studies demonstrated that once-daily oral Zeposia was superior to once-weekly injectable Avonex (interferon beta-1a) in terms of annualized relapse rate (ARR), as well as the number and volume of brain lesions. Specifically:
During the 2-year treatment period, there was no significant difference between the Zeposia group and the Avonex group in the proportion of patients who experienced disability due to disease progression at months 3 and 6. Zeposia demonstrated favorable safety and tolerability profiles in both studies. The prescribing information for Zeposia indicates that it may increase the risk of infections, bradyarrhythmias, atrioventricular conduction delays, hepatic injury, fetal health risks, hypertension, respiratory symptoms, macular edema, and posterior reversible encephalopathy syndrome. The most commonly reported adverse reactions (incidence ≥4%) include upper respiratory tract infection, elevated liver enzymes, orthostatic hypotension, urinary tract infection, back pain, and hypertension.
Multiple sclerosis (MS) is a chronic disease caused by an abnormal immune response in which the body’s immune system attacks the myelin sheaths of nerve cells in the brain, spinal cord, and optic nerves. It manifests as muscle weakness, fatigue, and visual disturbances, ultimately leading to disability. There are approximately 2.3 million people with MS worldwide; of these, 85% are classified as having relapsing-remitting multiple sclerosis (RRMS) at initial diagnosis, while 15% have primary progressive multiple sclerosis (PPMS). Patients with RRMS experience periodic relapses and remissions; as the disease progresses, it often evolves into secondary progressive multiple sclerosis (SPMS). In contrast, patients with PPMS exhibit continuous worsening of symptoms without distinct remission periods. Currently, there is no cure for MS.
Ozanimod is a sphingosine-1-phosphate receptor (S1PR) modulator with high affinity for S1PR1 and S1PR5 on the surface of lymphocytes. Upon binding to these receptors, ozanimod prevents lymphocytes from egressing lymph nodes and entering the central nervous system, thereby exerting anti-inflammatory effects. In addition, siponimod can penetrate the central nervous system and directly bind to S1PRs on oligodendrocytes and astrocytes, promoting remyelination and preventing inflammation.
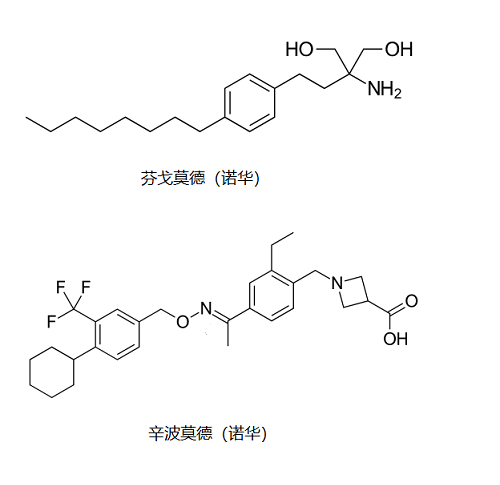
In September 2010, Novartis launched Gilenya (fingolimod), the world’s first sphingosine-1-phosphate receptor (S1PR) modulator for the treatment of multiple sclerosis (MS). It was also the first oral therapy capable of reducing the frequency of relapses in MS patients, and it quickly became a blockbuster drug after its market debut. In 2019, Gilenya generated $3.223 billion in sales revenue. As the patent cliff approached, Novartis introduced Mayzent (siponimod), a next-generation S1PR modulator, in March 2019, thereby maintaining its leading position in this therapeutic area. In 2019, Mayzent achieved $26 million in sales revenue.
Bristol-Myers Squibb’s Zeposia (ozanimod) is the third S1P receptor modulator approved globally, directly challenging Novartis’ market position. Originally developed by Receptos, ozanimod demonstrated potential to compete with the flagship product in the multiple sclerosis (MS) market during its clinical development phase, prompting Celgene to acquire Receptos for $7.2 billion in July 2015 and bring ozanimod into its portfolio. Ozanimod was also one of the key assets that motivated Bristol-Myers Squibb’s $74 billion acquisition of Celgene. In addition to multiple sclerosis, ozanimod’s indications for Crohn’s disease and ulcerative colitis have advanced to late-stage development, positioning it as a leader in the S1P receptor modulator class for these two indications and aligning with BMS’ strategic focus on autoimmune diseases.

The market approval process for Zeposia was also fraught with twists and turns. Celgene initially submitted the New Drug Application (NDA) for ozanimod in December 2017, but received a Refusal to File (RTF) letter from the U.S. Food and Drug Administration (FDA) on February 28, 2018. In the RTF letter, the FDA indicated that there were gaps in certain pharmacological data from the preclinical and clinical studies of ozanimod, rendering the application unacceptable for filing, and requested the submission of additional materials. This development raised concerns among investors regarding the market prospects of this product, which had been acquired at a significant cost. Celgene’s stock price plummeted by more than $6 billion overnight.
When Bristol-Myers Squibb (BMS) announced its major acquisition of Celgene in January last year, it faced shareholder opposition. The primary concerns for BMS shareholders were the patent challenge risks associated with lenalidomide and the regulatory approval risks for the key asset ozanimod. However, Celgene’s resubmission of the marketing application for ozanimod in March 2019 reassured BMS shareholders and bolstered support for the acquisition vote in April 2019. In June 2019, BMS announced that both the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) had accepted the marketing applications for ozanimod. With the drug’s approval today, BMS shareholders can finally breathe a sigh of relief.
Novartis’s Gilenya is priced at $6,000 per year, while Mayzent is priced at $8,800 per year. Although Zeposia has been approved, it still faces a challenging path to pricing and market launch. Given that the U.S. healthcare system is urgently responding to the COVID-19 pandemic, Bristol-Myers Squibb (BMS) has had to decide to postpone the commercial launch of Zeposia. The specific launch timing will be determined based on changes in the public health situation and following consultations with partner neurology societies. The marketing authorization application for Zeposia in Europe is currently under review, with results expected in the first half of 2020.