GSK's First-in-Class Attachment Inhibitor Fostemsavir Shows Strong Efficacy in Multidrug-Resistant HIV-1 Infection
Mar 30, 2020 02:47
CST Updated
02:47

ViiV Healthcare
AIDS Drug Developer

GSK
Pharmaceutical R&D Manufacturer
March 29, 2020 /BioValleyBIOON/ --ViiV Healthcare is aGlaxoSmithKline(GSK) Holding,Pfizeran HIV/AIDS drug development company held by Pfizer and Shionogi. Recently, data from the pivotal Phase III BRIGHT clinical trial (NCT02362503) of the company’s investigational drug fostemsavir for the treatment of patients with multidrug-resistant HIV infection were published in the New England Journal of Medicine (NEJM), a top-tier international medical journal.
Fostemsavir is a first-in-class HIV-1 attachment inhibitor and an investigational prodrug of temsavir. It functions by directly binding to the glycoprotein 120 (gp120) subunit on the viral surface. By binding to this site on the virus, fostemsavir prevents HIV from attaching to CD4+ T cells and other immune cells of the host immune system, thereby inhibiting viral infection and replication in these cells. Due to its unique mechanism of action, fostemsavir can benefit individuals living with HIV who have developed resistance to most other antiretroviral agents.
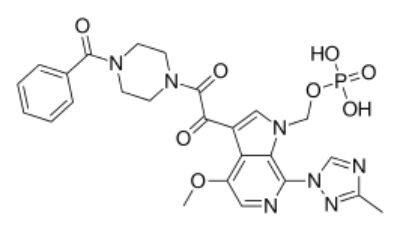
Chemical Structure of Fostemsavir (Image Source: Wikipedia)
Currently, fostemsavir is under review by the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA): in combination with other antiretroviral agents, for the treatment of heavily treatment-experienced adults with multidrug-resistant HIV-1 infection who are unable to achieve viral suppression due to resistance, intolerance, or safety considerations, and who have previously received multiple regimens. Previously,FDAFostemsavir has been granted Fast Track designation and Breakthrough Therapy designation. The EMA has granted fostemsavir accelerated assessment. If approved for marketing, fostemsavir will provide an important treatment option for people living with HIV who are unable to suppress the virus with other medications due to various reasons.
Over the past 30 years, incredible progress has been made in HIV treatment. Antiretroviral drugs can effectively suppress HIV, helping to reduce disease progression, HIV transmission, and AIDS-related deaths. However, due to HIV’s ability to continuously mutate, some patients may develop resistance to antiretroviral drugs, leading to treatment failure. Challenges related to tolerability, safety, and drug interactions may further limit the number of acceptable antiretroviral therapies available for designing effective treatment regimens. There remains a significant unmet medical need among multidrug-resistant patients who have previously received multiple regimens and failed to achieve successful HIV suppression. Efficacy and safety results from the fostemsavir clinical development program indicate that this drug holds unique potential for individuals with multidrug-resistant HIV who require new treatment options. If approved for marketing, fostemsavir would provide a novel approach to help these patients achieve viral suppression.
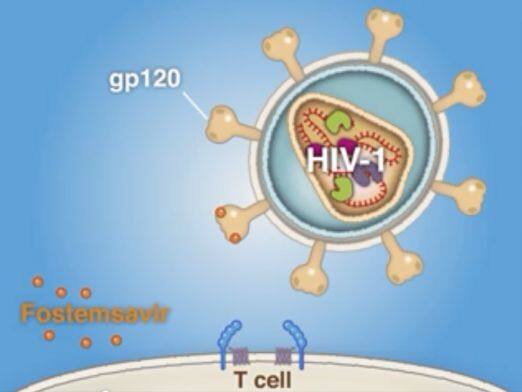
Mechanism of Action of Fostemsavir (Image source: Article published in NEJM)
In the United States and the European Union, the submission of the New Drug Application (NDA) for fostemsavir and the Marketing Authorization Application (MAA) were both based on data from the pivotal Phase III clinical study, BRIGHT. This was a two-cohort (randomized and non-randomized) study evaluating the safety and efficacy of fostemsavir, an HIV-1 attachment inhibitor, in heavily treatment-experienced adults with HIV-1 infection. A total of 371 patients were enrolled in the study, all of whom had documented resistance, intolerance, and/or contraindications to four of the six currently available classes of antiretroviral (ARV) drugs.
In the randomized cohort, patients were required to have full activity against no more than two but at least one class of antiretroviral (ARV) drugs at baseline and be unable to form a viable ARV regimen from their remaining active agents. These patients were randomized in a 3:1 ratio to receive blinded fostemsavir or placebo added to their current failing regimen (n=272), resulting in functional monotherapy for 8 days. Patients with no remaining fully active approved ARVs (n=99) were assigned to the non-randomized cohort and received open-label fostemsavir plus optimized background therapy on Day 1. The primary endpoint was the mean change in log10 HIV-1 RNA from Day 1 to Day 8 in the randomized cohort. After the 8-day double-blind period, all patients in the randomized cohort received open-label fostemsavir plus optimized background therapy. Key secondary endpoints included the durability of response at Weeks 24, 48, and 96, as well as changes in CD4+ cell counts from baseline and the emergence of viral resistance.
The results showed that, based on the adjusted mean decline in HIV-1 RNA from Day 1 to Day 8 in the randomized cohort, the primary endpoint analysis demonstrated that fostemsavir was superior to placebo (declines of 0.79 and 0.17 log10 copies/mL, respectively; p < 0.0001 in the intent-to-treat-exposed [ITT-E] population).
In the randomized cohort, rates of virologic suppression and immune response continued to increase from Week 24 to Week 96 in this difficult-to-treat population of patients with multidrug-resistant HIV-1. Specifically, among patients in the randomized cohort (n=163/272) who received fostemsavir plus optimized background therapy (OBT), the proportions achieving virologic suppression (HIV-1 RNA <40 copies/mL [c/mL]) at Weeks 24, 48, and 96 were 53%, 54%, and 60%, respectively. Over time, patients demonstrated sustained immune improvement, with mean increases in CD4+ cell counts continuing to rise (increases of 90, 139, and 205 cells/μL at Weeks 24, 48, and 96, respectively).
In the study, the most commonAdverse Reactions(≥5%, all grades) were nausea and diarrhea. By Week 96, 7% of patients discontinued fostemsavir treatment due to adverse events (randomized: 5%; non-randomized: 2%). (Bioon.com)
Original Source:Fostemsavir in Adults with Multidrug-Resistant HIV-1 Infection