An EEG Headband with FDA Breakthrough Designation Rewrites the Landscape of In-Hospital Stroke Diagnosis and Treatment

Ceribell
Medical Diagnostic System Developer
In January 2026, Ceribell (Nasdaq: CBLL) announced that its detection and monitoring solution for acute large vessel occlusion (LVO) strokes, both intracranial and extracranial, received the "Breakthrough Device Designation" from the U.S. FDA. This solution is developed based on Ceribell’s existing hardware platform and uses artificial intelligence algorithms to analyze electroencephalogram (EEG) signals, aiming to enable early detection of LVO strokes, bringing critical innovation to the field of stroke diagnosis and treatment.

Image source: Ceribell.com
According to the "Interpretation of Data from the 2025 Global Stroke Report" released by the Army Medical University team, stroke remained the second leading cause of death globally in 2021. China bears the heaviest stroke burden worldwide, characterized by the "four highs": high incidence, high prevalence, moderately high mortality, and moderately high DALYs, placing a dual burden on both society and patients' families in China.
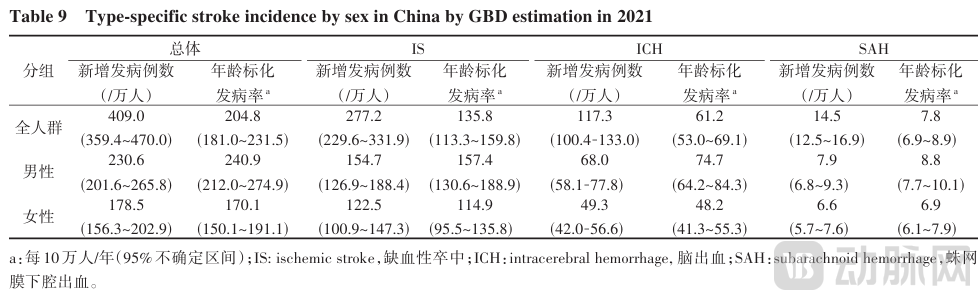
Incidence Rates of Different Types of Stroke by Gender in China, 2021
According to data from the Ceribell official website, in the main type of stroke—ischemic stroke, acute large vessel occlusion (LVO) in the cranium and extracranial areas is a medical emergency. Compared with non-LVO ischemic stroke, LVO has higher morbidity and mortality rates, accounting for approximately 96% of post-stroke mortality. In the United States, among approximately 800,000 stroke patients annually, in-hospital strokes account for up to 17%. These types of strokes often occur in non-neurology departments, and the related bedside medical teams may lack sufficient training or tools to accurately identify subtle neurological changes caused by strokes. Additionally, many patients are in postoperative recovery, intubated, or on ventilator support, or are under the influence of medications, making assessments more complex and early signs of stroke difficult to detect.
Therefore, unlike community-based strokes that occur outside the hospital and typically trigger an immediate emergency response, in-hospital strokes often experience significant delays in detection and treatment. This results in a mortality rate approximately three times higher than that of out-of-hospital stroke patients, even after adjusting for clinical characteristics and comorbidities, with the likelihood of being discharged home being only half as much.
Time is Brain——A tool that can continuously monitor brain function and alert the medical team immediately when abnormalities occur will help enable early intervention, thereby improving prognosis for in-hospital stroke patients.
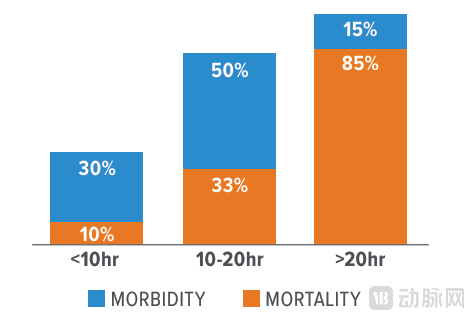
The longer the duration of non-convulsive status epilepticus (NCSE), the higher the morbidity and mortality, Source: Ceribell.com
Traditional stroke diagnosis heavily relies on imaging methods such as CT and MRI. The complete process involves patient transfer, equipment scanning, and image interpretation, often taking several hours. Such delays may cause patients to miss the optimal intervention window, thereby exacerbating neural damage and increasing the risk of sequelae.
At the same time, the practical application of conventional EEG technology faces multiple constraints: first, its setup relies on professional technicians, but there is a shortage of technicians and their working hours are limited, which can easily lead to delays; second, the recorded content must be interpreted by neurology specialists before it can be used for diagnosis and treatment, yet such expert resources are scarce, further slowing down the diagnosis; third, the occurrence of in-hospital strokes is random and requires continuous monitoring, but hospitals lack the manpower to conduct long-term uninterrupted EEG observation.
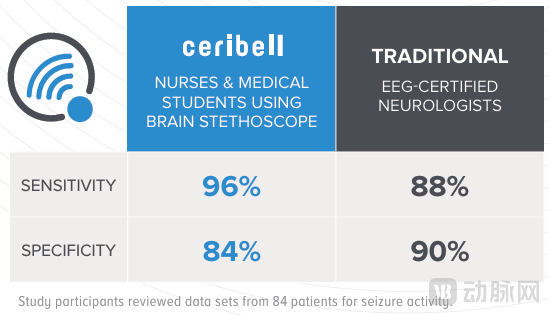
Comparison of Detection Capabilities Between Ceribell and Traditional EEG Devices, Image Source: Ceribell.com
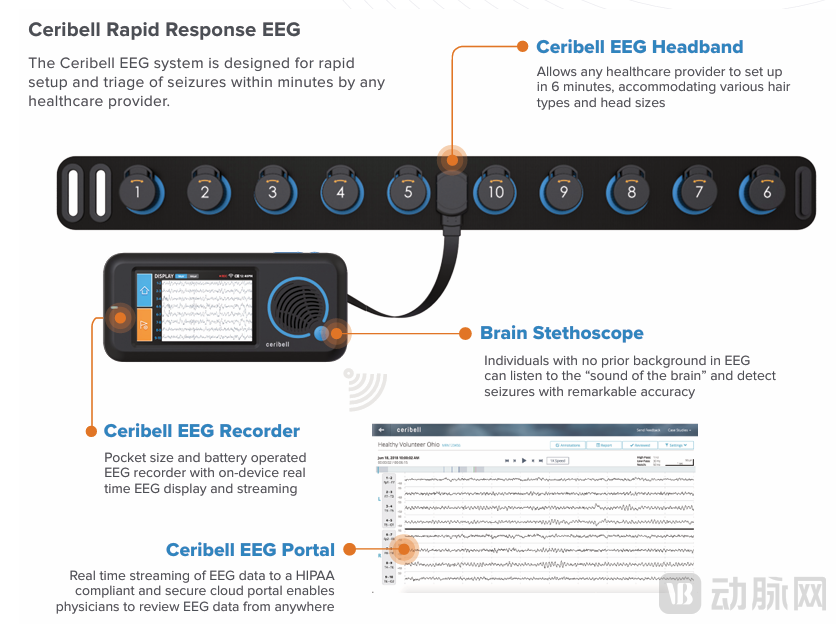
Facing these challenges, the bedside EEG model adopted by Ceribell, which features a "flexible headband + pocket-sized recorder," enables timely and reliable EEG assessment and continuous monitoring. It can be rapidly deployed in emergency rooms, ICUs, and at the bedside. Moreover, non-specialized medical staff, after about an hour of simple training, can help patients complete device installation within 5 minutes, significantly improving the efficiency of early stroke detection.
Source: Ceribell.com
Specifically, the product consists of four parts:
1. Disposable Flexible EEG Headband: The disposable flexible EEG headband requires no traditional electrodes or conductive gel, offering comfortable fit and quick preparation;
2. EEG Recorder: A pocket-sized, battery-powered wireless transmission recorder ensures patient mobility, enhances comfort, and facilitates medical operations. In high-pressure scenarios such as emergency rooms and ICUs, the device can be rapidly deployed to save critical time for treatment.
3. Clarity AI Algorithm: The team has developed a deep learning algorithm based on tens of millions of EEG data points to extract valuable insights. This AI algorithm can accurately differentiate between LVO stroke-related abnormal signals and background noise. It supports rapid single-test detection for urgent diagnosis while enabling continuous monitoring and dynamic tracking of the patient’s condition, providing end-to-end information such as early warning of stroke onset and treatment efficacy evaluation. It addresses the efficiency and accuracy limitations of traditional EEG manual interpretation, upgrading the process from data collection to clinical decision support.
4. EEG Management System: The Ceribell EEG System enables real-time transmission of EEG data through a cloud-based portal, allowing doctors to access the data anytime, anywhere. Its signal quality is comparable to traditional EEG devices and includes a full recording annotation feature that significantly enhances interpretation efficiency. The system can also generate seizure burden trend graphs, providing critical insights for effective seizure management and real-time evaluation of drug efficacy.
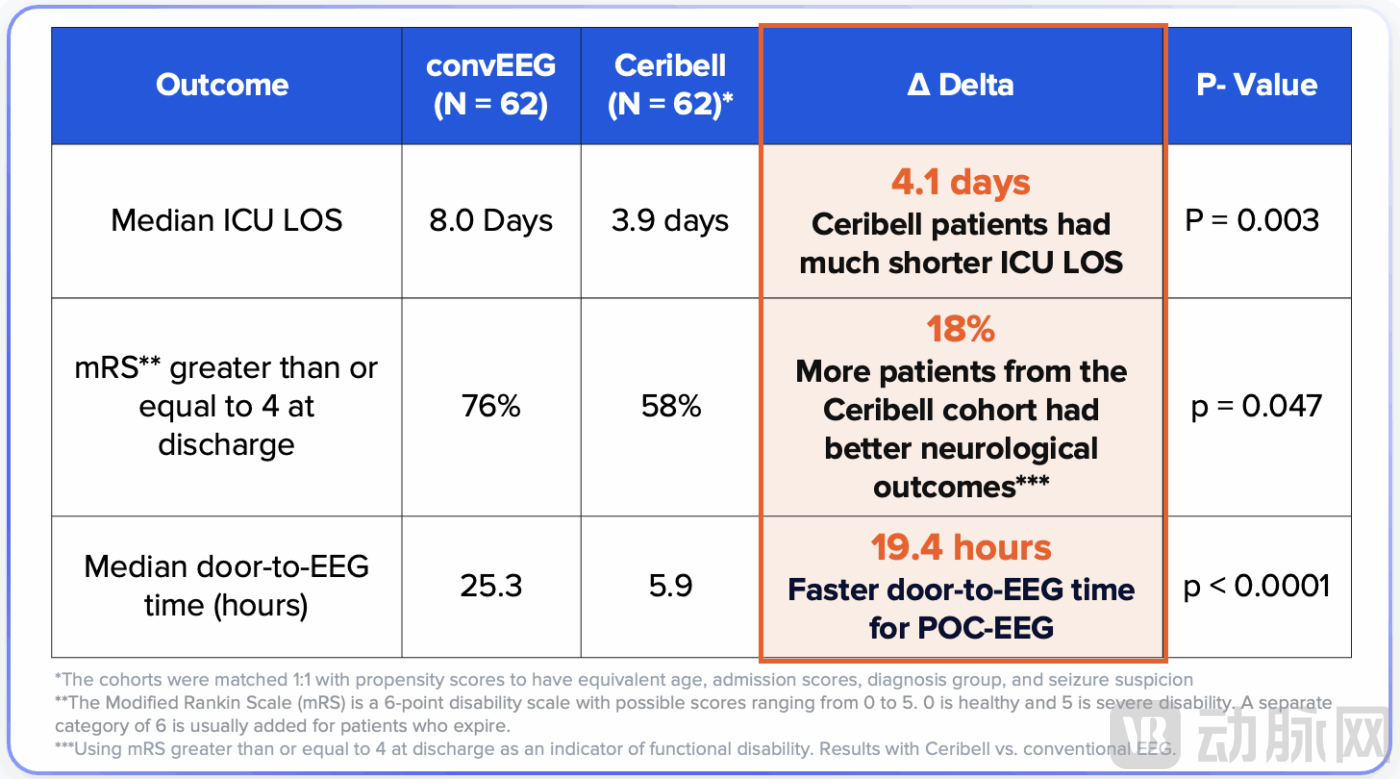
Ceribell has published nearly 50 papers and 100 abstracts, and released the largest SAFER study in 2025. This study found that even in top medical institutions, traditional EEG devices took an average of 19 hours to reach the patient's bedside. In contrast, patients using the Ceribell device had their ICU stay shortened by 4.1 days with better clinical outcomes. Specific data shows that the proportion of patients with severe disabilities at discharge was 76% in the traditional EEG group, while it dropped to 58% in the Ceribell group, a decrease of 18 percentage points. This means that approximately one-fifth of patients were able to recover at home instead of being transferred to care facilities, which significantly impacts the patients and their families.
Source: Ceribell.com
Ceribell's business model mainly relies on two recurring revenue streams: 25% of the revenue comes from subscription fees, which are monthly payments made by hospitals for using recorders, the Clarity algorithm, and related portal services; 75% of the revenue is derived from the sales of single-patient-use flexible EEG headbands.
Under the DRG/DIP medical insurance payment system, cases with MCC coding have significantly higher payment weights compared to basic cases. Increased use of EEG makes it easier to detect occult neurological abnormalities, aiding in the accurate coding of major complications and comorbidities (MCC). Each time a complication or severe complication (CC/MCC) is identified and recorded through an EEG examination, the hospital can secure an additional $5,000 to $24,000 in medical insurance reimbursement for that case.

Image source: Ceribell.com
As of now, its target markets are primarily concentrated in the intensive care unit (ICU) and emergency department (ED). In the United States alone, the potential size of this niche market exceeds $2 billion. By 2025, the company expects to achieve revenue between $87 million and $89 million, representing a year-over-year growth of approximately 34%, with a gross margin reaching 88%.
Ceribell is a medical technology company focused on transforming the diagnosis and management of patients with severe neurological conditions. Ceribell has developed the Ceribell System, an innovative bedside EEG platform specifically designed to address unmet patient needs in acute care settings. Xingjuan Chao, President, CEO, Co-founder, and Director of Ceribell, holds a Bachelor’s degree in Chemistry from Peking University and a Ph.D. in Biophysics from Cornell University. Prior to joining Ceribell, Dr. Chao worked at Genentech, Novartis, McKinsey, and Magnus Medical.