Two Decades of Challenges in Hyperphosphatemia Treatment: Libang Pharmaceuticals' Two Innovative Pipelines Are Rewriting the Answer
Opening the "Blue Paper on the Current Status of Medical Diagnosis and Treatment for Hyperphosphatemia in China" (hereinafter referred to as the "Blue Paper"), a set of figures is shocking —

However, everything is changing quietly.
In 2024, the National Health Commission (NHC) listed improving the blood phosphorus control rate of dialysis patients as a key quality control improvement goal for the nephrology specialty for the first time.In 2025, the National Nephrology Quality Control Center reaffirmed: to continuously promote key medical quality improvements, placing the control rate of blood phosphorus management alongside the control rate of renal anemia as the core focus for the year. At the National Nephrology Quality Control Center conference, Academician Xiangmei Chen further emphasized the need to systematically advance from four aspects: medical institution diagnosis and treatment management, data monitoring, quality improvement, and central supervision.
The baton of quality control has been raised, and clinical practice must respond. However, in actual daily management, clinicians often feel that the existing tools are not yet adequate.
In the qualitative interviews of the "Blue Book," a nephrologist described his daily routine this way: "Monitoring blood phosphorus levels always takes a backseat to urgent issues like hyperkalemia and anemia. It's not that we don't care; it's just that we can't keep up." A patient who had been on regular dialysis for three years was taking more than ten sevelamer tablets every day, enduring persistent nausea and bloating, yet his blood phosphorus levels remained consistently above 1.8 mmol/L (approximately 5.58 mg/dL). The doctor said that if this continued, vascular calcification would only be a matter of time. What he didn’t realize was that this wasn’t an isolated case but rather one among over a million dialysis patients in China.76% of patients with uncontrolled blood phosphorus levelsThe collective epitome.
AP301 and AP306 from Libang Pharmaceuticals are specifically designed to address this clinical gap. These two drugs respectively focus on "optimizing existing treatments" and "covering treatment blind spots," precisely targeting the weak points in the current therapeutic landscape. The former redefines the standard for first-line foundational treatment with its attributes of "no chewing required, lower daily dosage, and high target achievement rate," while the latter, with its breakthrough efficacy, has the potential to revolutionize the treatment paradigm for phosphorus management.
The "Triple Dilemma" of Phosphorus Control: Why 76% of Patients Are Stuck in a Deadlock
The management of hyperphosphatemia follows the classic "3D principle": Diet, Dialysis, and Drug. However, each principle faces significant challenges in clinical practice, jointly forming the complex puzzle of the current dilemma.
Dietary control is fundamental, but the difficulty of implementation is tantamount to an "impossible mission." According to the research in the *Blue Book*, 94% of doctors require patients to strictly limit phosphorus intake. However, traditional Chinese diets include high-protein foods rich in phosphorus, such as bean products, nuts, and animal organs. Moreover, inorganic phosphate additives (with an absorption rate as high as 90%-100%) commonly found in modern processed foods and condiments are "hidden phosphorus bombs." Patients often find themselves in a dilemma of "wanting to eat but not daring to, needing to eat but being unable to." The strict limitation of phosphorus simultaneously leads to insufficient protein intake, causing malnutrition, which itself is a risk factor for mortality. In other words, relying solely on patient self-discipline for dietary phosphorus control is extremely challenging, and the outcomes of serum phosphorus management remain far from satisfactory.
Dialysis is the core method for clearing blood phosphorus, but its efficiency in phosphorus removal is limited and only functions during dialysis sessions, after which blood phosphorus levels quickly rebound. More critically, the adequacy of dialysis in China still needs improvement. Data from DOPPS shows that over 20% of hemodialysis patients in China still follow a twice-weekly regimen, and nearly 30% of patients do not meet the adequacy standard (spKt/V), further restricting the upper limit of phosphorus clearance through dialysis.
When non-pharmacological means fall short, pharmacological treatment should become the mainstay. However, the *Blue Book* reveals that the current state of drug treatment for hyperphosphatemia in China has fallen intoInadequate efficacy, poor compliance, safety concerns"The Triple Dilemma."
Dilemma 1: Severe delay in treatment initiation.According to the "Chinese Expert Consensus on Clinical Management of Hyperphosphatemia in Chronic Kidney Disease (2025 Edition)," the blood phosphorus intervention threshold should be >1.45 mmol/L (approximately 4.50 mg/dL). However, a survey of doctors shows that only 6% strictly adhere to this standard for initiating drug treatment, while up to 70% of doctors relax the threshold to between 1.45 mmol/L (approximately 4.50 mg/dL) and 1.78 mmol/L (approximately 5.52 mg/dL). Moreover, 24% of doctors wait until the patient’s blood phosphorus level exceeds >1.78 mmol/L (approximately 5.52 mg/dL) before starting intervention. The widespread delay in treatment timing leaves patients chronically exposed to the risks of hyperphosphatemia, missing the critical window for early intervention to improve prognosis.
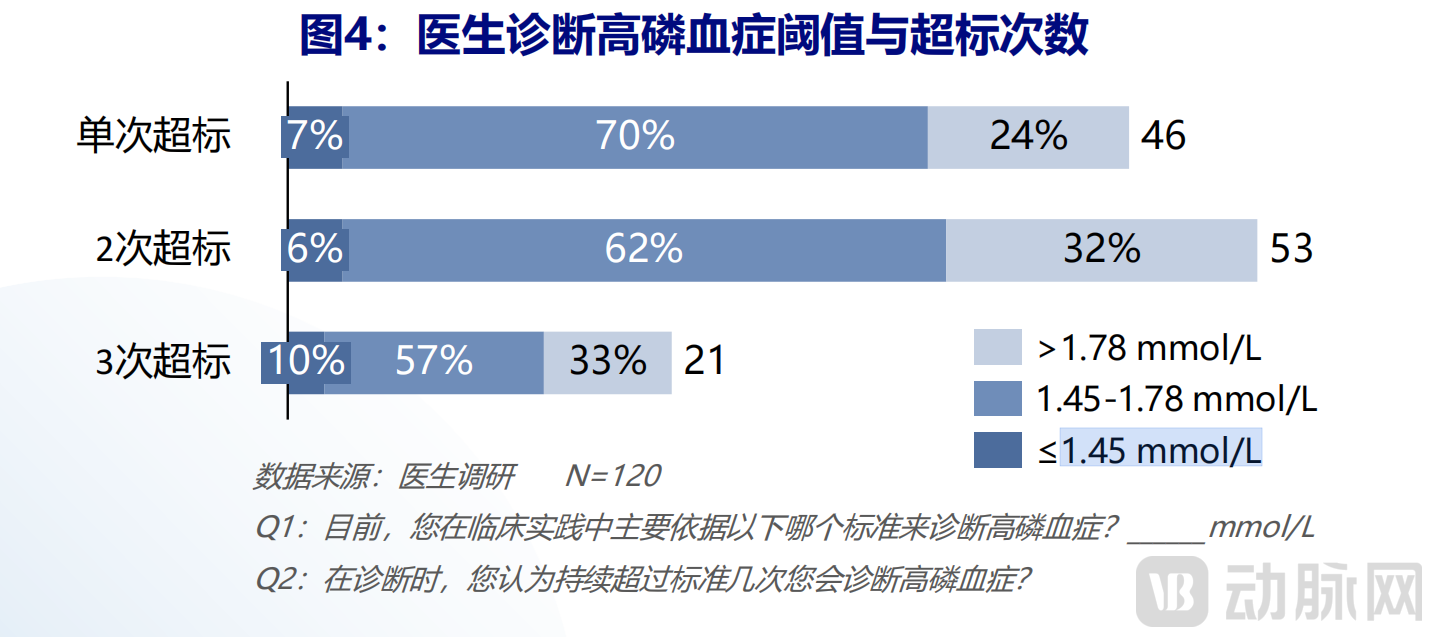 Source: "Blue Paper on the Current Status of Diagnosis and Treatment of Hyperphosphatemia in China"
Source: "Blue Paper on the Current Status of Diagnosis and Treatment of Hyperphosphatemia in China"
Dilemma 2: Pill Burden and Side Effects Are the "Compliance Killers" for Patients Sticking to Treatment.The currently leading non-calcium phosphate binders in clinical practice, such as sevelamer carbonate and lanthanum carbonate, while reducing the risk of vascular calcification associated with calcium-containing phosphate binders, have notable shortcomings in terms of convenience and tolerability.
Sevelamer requires patients to take 6-12 large tablets daily, accounting for "half of the daily medication" for dialysis patients. Its gastrointestinal side effects are prominent; a systematic review showed that among sevelamer-related gastrointestinal injuries, 44.2% were bleeding, 37.7% were abdominal pain, and there was even a certain mortality rate. Patients described its texture as hard, "like swallowing stones." On the other hand, lanthanum carbonate needs to be chewed before swallowing, with the most common complaints being "chewing chalk" and "medicine residue stuck in teeth." Additionally, the deposition rate of lanthanum in the stomach is as high as 60%-85%, raising concerns about its long-term safety.
The heavy pill burden and significant side effects lead to an extremely high rate of patients discontinuing medication on their own. According to the research from "The Blue Book",73% of patients cannot adhere to long-term medication due to gastrointestinal side effects, and 58% of patients find it difficult to tolerate the high daily dosage.
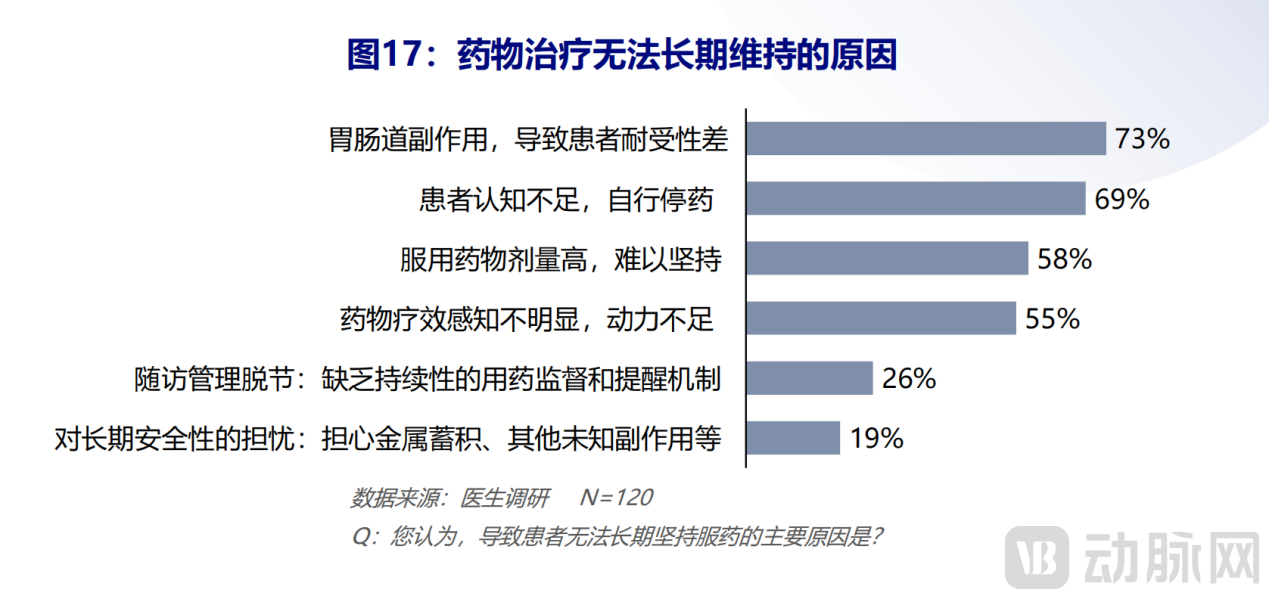 Source: "Blue Paper on the Current Status of Diagnosis and Treatment of Hyperphosphatemia in China"
Source: "Blue Paper on the Current Status of Diagnosis and Treatment of Hyperphosphatemia in China"
Dilemma Three: Existing solutions have reached a ceiling in efficacy.Even if patients overcome difficulties and adhere to medication, the phosphorus-lowering efficacy of existing drugs is still facing a bottleneck. Doctors' overall satisfaction rating with current solutions is less than ideal, particularly scoring low on long-term safety and patient tolerance. For patients who have adopted high-dose phosphorus-lowering drugs but still fail to achieve standard serum phosphorus levels, there is a lack of more effective options in clinical practice.
The "Blue Book" provides cold, hard data to substantiate this dilemma through quantitative research: among CKD dialysis patients diagnosed with hyperphosphatemia, only 71% received medication, and overall control outcomes were poor; regardless of whether they were medicated, a large number of patients remained continuously exposed to the risk of hyperphosphatemia.
At this point, a clear picture emerges — a critical indicator affecting millions of lives has been neglected due to insufficient monitoring, missed opportunities due to delayed treatment, and deterred both doctors and patients because of the drug’s inherent flaws, ultimately resulting in the severe situation of "high prevalence, low control rates." Clinical experts and patients are urgently calling for a new treatment paradigm capable of simultaneously addressing the three major challenges of "potency, safety, and convenience."
Industry Consensus: The Clinical Profile of the Next Generation of "Ideal Drugs"
Facing the dilemma of hyperphosphatemia management, clinicians share clear and urgent common expectations. The *Blue Book*, through large-scale physician surveys, vividly outlines the profile of the next-generation ideal phosphate-lowering drug.
First, it offers a more potent phosphorus-lowering capability, which is the core of breaking the deadlock.Doctors urgently need solutions that can break through the current efficacy ceiling, especially for situations where control remains poor even after treatment, fundamentally improving the rate of phosphate target achievement.
The second is better long-term safety.That is, it must completely avoid the risk of vascular calcification, eliminate concerns about metal accumulation, and significantly improve gastrointestinal tolerance to ensure that patients can use it safely and over the long term.
And more convenient medication regimens,This is reflected in the need to significantly reduce the daily pill burden and the difficulty of swallowing/chewing. "Turning a handful of pills into just a few" is the key to improving long-term compliance.
In addition, there is a more stable supply guarantee.Medicines need to be accessible, ensuring that patients can continuously receive treatment through reasonable payment policies and a stable supply chain.
These four major expectations go straight to the core of current clinical pain points. Industry consensus has already formed: the future game-changer must not only provide solid clinical data to prove its efficacy but also achieve a systematic breakthrough in safety, convenience, and accessibility. Whoever can deliver such results will take the initiative in defining the future treatment landscape.
Game Changer "Double-Edged Sword in Hand," Libang Brings Combined Solutions
On the competitive field of innovative drug development for kidney diseases, a Chinese biopharmaceutical company named Alebund Pharmaceuticals is attempting to provide a precise combination solution to the complex challenge of hyperphosphatemia through its unique and comprehensive pipeline layout. Alebund's two core investigational products for hyperphosphatemia, AP301 and AP306, represent "two sharp weapons" to break the deadlock, addressing the issue from the dimensions of "optimizing foundational treatment" and "disrupting treatment mechanisms," respectively.
1AP301: Reshaping "Cornerstone Therapy," Providing a New Solution for Long-term Safe and Effective Phosphorus Control
AP301 is an oral iron-based phosphate binder specifically designed to address the pain points of traditional non-calcium binders.
In terms of "high potency",AP301 has extremely high phosphate binding capacity. Results from its pivotal Phase III clinical trial (RESPONDER-1) showed that by Week 12 of treatment, AP301 was effective in reducing serum phosphorus levels.Not inferior to sevelamer carbonate(The reductions were 0.72 mmol/L (approximately 2.23 mg/dL) vs. 0.70 mmol/L (approximately 2.17 mg/dL), respectively.) More importantly, over the 52-week treatment period, AP301 demonstrated robust and sustained phosphorus-lowering effects, which remained stable at the end of treatment (Week 52).The serum phosphorus target achievement rate in the AP301 group was 67%, higher than 59% in the sevelamer carbonate group.The average total daily dose was lower in the AP301 group (7.45 g/day) vs. the sevelamer carbonate group (10.70 g/day, calculated by total drug weight).
In terms of "safety and convenience",AP301, due to the adoption of iron-polysaccharide fiber binding technology, has iron firmly bound to the polysaccharide fiber, fundamentally avoiding the potential overload risk associated with systemic iron absorption, which was confirmed in Phase III studies. In terms of gastrointestinal tolerance, the most common adverse events are stool discoloration and diarrhea, with diarrhea mostly occurring in the early stages of treatment, being mild in severity, alleviating long-term constipation in dialysis patients, and rarely leading to treatment discontinuation. In terms of formulation, AP301Capsule form, no chewing required,It avoids the trouble of chewing or swallowing difficulties, and has a small swelling volume in gastric juice, further improving safety and tolerance.
Currently, AP301 has a clear clinical positioning with its potent, safe, and convenient characteristics,It is expected to replace or upgrade existing non-calcium phosphate binders, becoming the "new cornerstone" for first-line treatment of hyperphosphatemia in dialysis patients.The goal is to enable a broader patient population to achieve better efficacy and experience at the starting point of treatment.
2AP306: Global First-in-Class Mechanism "Dimensionality Reduction Attack", Breaking Through the Ceiling of Blood Phosphorus Control
If AP301 aims to "raise the baseline and benefit widely," then AP306 is targeted at "focused breakthroughs and entirely new advancements." AP306 isThe world's first oral pan-phosphate transporter inhibitor.Its mechanism of action is fundamentally different from that of traditional phosphorus binders (which passively "bind" with phosphorus in the intestines): it actively shuts down key pathways for intestinal phosphorus absorption by inhibiting sodium-dependent phosphate transporter IIb (NaPi-IIb), phosphate transporter-1 (PiT-1), and phosphate transporter-2 (PiT-2).
This novel mechanism has also brought remarkable clinical feedback.
The goal of AP306 is to fully address the unmet needs of the majority of patients with hyperphosphatemia, especially those who respond poorly to or are intolerant of existing phosphate binders. It represents a therapeutic strategy innovation shifting from "passive binding" to "active inhibition."
The AP301 and AP306 from Libang Pharmaceuticals form a highly synergistic solution tailored for clinical applications.AP301 serves as a foundational, broad-spectrum first-line option, aiming to optimize the treatment experience and target achievement rate for the majority of patients; AP306, on the other hand, acts as a "blockbuster product," offering a disruptive, highly efficient, and low-burden solution with a completely new mechanism.In today's context, where the *Blue Book* repeatedly emphasizes the importance of "individualized management" and "stratified treatment," the choice of this strategic approach is itself a result of a deep understanding of clinical needs.
Let "76%" Become History: A Predictable Clinical Revolution
The publication of the "Blue Book" completed a thorough review of hyperphosphatemia in China. Its value lies in piecing together all fragmented challenges into a complete map, guiding future problem-solvers on where to go. Currently, AP301 and AP306 are advancing along this map. The former has completed Phase III clinical trials and entered the countdown to NDA submission (expected in the first half of 2026); the latter has received Breakthrough Therapy designation and is about to initiate subsequent registrational clinical studies. As innovative therapies represented by AP301 and AP306 from Libang Pharmaceuticals gradually move toward market launch, the treatment landscape for hyperphosphatemia in China is also expected to undergo significant transformation.
First is the adjustment of the treatment decision logic. When drugs like AP301 enter the first-line treatment, doctors will no longer need to make a difficult trade-off between "phosphate-lowering efficacy" and "patient tolerance" when facing newly diagnosed hyperphosphatemia patients. The glaring "29% of patients not receiving medication after diagnosis" figure in the Blue Book may finally be shaken.
Next is the shift in the target range for blood phosphorus control. Currently, in clinical practice, the blood phosphorus levels of most patients consistently hover near the upper limit of the control range (5.5 mg/dL), largely due to the ceiling effect of existing medications—patients are already using the maximum dose and enduring side effects, yet their blood phosphorus remains uncontrolled. The emergence of AP306 has significantly pushed back this boundary. Additionally, with the smooth inclusion of such drugs with an extremely low pill burden into medical insurance, the economic and psychological barriers to long-term treatment will be greatly reduced, fundamentally improving patient compliance.
Finally, there is a structural increase in the compliance rate. The compliance rate for blood phosphorus levels among dialysis patients in China has long fluctuated between 24% and 39%. Behind this figure lie both systemic issues such as late initiation of treatment and low monitoring frequency, as well as biological limitations imposed by the capped efficacy of existing drugs. AP301 and AP306 cannot address the former—this requires long-term collaboration across payment systems, tiered medical care, and patient education. However, they are capable of resolving the latter: when foundational medications become easier to adhere to, and clinical experts are equipped with a powerful tool, the compliance rate will experience a definitive upward shift. From 24% to what number remains to be answered by real-world data. But the direction is already clear.
Written at Last
The Blue Book concludes: "It is expected that the release of the Blue Paper on the Current Status of Diagnosis and Treatment for Chinese Hyperphosphatemia Patients and Physicians will provide scientific decision-making references and practical guidance to enhance the standardized management of hyperphosphatemia in China." This also sends a message to the industry: the field has been stuck too long in a low-level equilibrium, with patients enduring too many avoidable risks and suffering. China has 156 million CKD patients, of whom more than 24 million suffer from hyperphosphatemia. The persistently high phosphorus levels on lab reports are waiting for change.
The game changers are on the way, calling for more "hardcore innovations" like AP301 and AP306, which are based on cutting-edge science and patient needs, and dare to seek comprehensive breakthroughs in efficacy, safety, and convenience. At the same time, as mentioned in the *Blue Paper*, doctors strongly desire "stronger phosphorus-lowering efficacy" and "lower pill burden," but they also pragmatically care about "supply stability" and "economic accessibility." For a good drug to truly change clinical outcomes, it must successfully transform from scientific value to market value.
The Blue Book lays out the issues in front of everyone. Now, it's time to submit the answers.