Temporal Interference Stimulation: A Breakthrough in Non-Invasive, Precise Deep Brain Neuromodulation for Humans

Neurodome
Neurodome, Inc.
Recent, École Polytechnique Fédérale de LausanneFriedhelm C. HummelWaitScholarIn《Nature Biomedical Engineering》(Impact Factor26.7)Published inTitled“Temporal interference stimulation for deep brain neuromodulation in humans” of important reviews. This article systematically elaboratesTemporal Interference Stimulation(temporal interferenceTI)ResearchofProgress, Mechanism、Challengeand Optimization Directions, providing for basic research and clinical applicationsserved as an important reference. WorthyFollowingYes,Multiple studies cited in the text (e.g., references103、118etc.)All usedNeurodome's independently developedtTISDevice。The full text is translated as follows:
Abstract
Summary
Deep brain stimulation requires highly precise focusing on deep brain targets, so clinical applications mostly rely on invasive surgical methods.Transcranial Temporal Interference Stimulation(Transcranial temporal interference stimulation ,tTIS)It is a non-invasive, localized electrical stimulation technique that can act on deep brain structures.This technology was initially developed and validated for efficacy using computational simulation models and rodent experiments. It has since been progressively applied in human studies, enabling precise targeting of deep brain nuclei such as the hippocampus and striatum. This article reviews the current evidence on tTIS-related neuromodulation research and elucidates itsPotential Mechanisms of Action,and explore the future development directions of this technology. At the same time, focus on analyzing its role in basic neuroscience research and the development of intervention strategies for neuropsychiatric disorders.Application Opportunities and Existing Challenges.We believe that, at this stage, it is necessary to conductMultidisciplinary Collaborative Research,Further validate the application value of tTIS in various research scenarios, clarify its underlying mechanisms, and optimize the technical framework to support large-scale basic research and clinical translation.

Introduction
Over the past few decades, non-invasive brain stimulation (NIBS) techniques have garnered interest in the field of neuroscience because they can modulate neural activity in specific brain regions. Techniques such as transcranial magnetic stimulation (TMS) and transcranial electrical stimulation (tES) have been proven to be effective tools for both basic research and clinical applications.
In basic neuroscience, these techniques can modulate neurophysiological activity in specific regions and infer their causal roles by investigating subsequent behavioral changes. Both TMS and tES are applied to cortical areas to study their involvement in a wide range of functions. Over the past two decades, non-invasive brain stimulation (NIBS) technologies have demonstrated significant translational potential, capable of enhancing activity in underactive brain regions, suppressing activity in overactive ones, or restoring synchrony when connectivity between brain regions is altered. This evidence has led to the approval of clinical applications for some of these approaches by regulatory agencies such as the U.S. Food and Drug Administration (FDA). For example, TMS is now an effective treatment option for refractory depression, addiction, and obsessive–compulsive disorder (OCD).
However, to date,Constrained by the inherent trade-off between depth and focality in these technologies, stimulation targets remain largely confined to the cerebral cortex.Stimulating deep brain regions requires higher intensities, which ultimately causes unintended off-target modulation of the overlying superficial (cortical) areas. Therefore, conventional non-invasive brain stimulation (NIBS) methods do not allow for selective modulation of key subcortical regions, such as the hippocampus, basal ganglia, thalamus, or cerebellum, which are involved in many cognitive functions and exhibit alterations in various neurological and psychiatric disorders, including Alzheimer’s disease, Parkinson’s disease, and stroke. Some traditional NIBS approaches, such as transcranial magnetic stimulation (TMS), can indirectly modulate deep brain regions via neural connections, but their focality is arguably limited. Due to this limitation, the function of subcortical regions has primarily been studied through animal recordings, lesion studies (e.g., post-stroke), or invasive techniques in patients with implants, thereby hindering detailed exploration and understanding of their healthy functioning. The high prevalence of disorders involving subcortical regions (e.g., Parkinson’s disease, Alzheimer’s disease, and obsessive-compulsive disorder) underscoresDevelopment of Alternative Non-Invasive Deep Brain StimulationThe Necessity of Deep Brain Stimulation (DBS) Technology.
tTIS was introduced for peripheral stimulation more than 30 years ago, but it has only recently been proposed for brain stimulation and validated through physical and animal experiments.tTIS has the potential to overcome the depth–focality trade-off associated with traditional non-invasive brain stimulation (NIBS), enabling focused modulation of deep brain structures.tTIS employs a combination of two electrode pairs to deliver high-frequency currents with a small frequency difference (Δf) (Fig. 1a), thereby enabling access to deep brain regions without affecting the overlying areas.The interference between two currents generates an envelope oscillating at a low frequency Δf. Since the high-frequency currents exceed the natural frequency range of neuronal activity, they are considered to have no effect on neural activity, whereas the low-frequency envelope can induce neural effects in regions where its amplitude is sufficiently large.(Fig. 1a). The electric field distribution can be optimized to localize the maximum amplitude modulation to deep regions while minimizing its amplitude in overlying tissues. Consequently, the overlying tissues are primarily exposed to unmodulated high-frequency stimulation, which is generally considered to have minimal neuromodulatory effects (see “Limitations and Current Challenges of tTIS” for further discussion).Optimization of the electric field distribution can be achieved through electrode placement and by adjusting the current intensity ratio between the two channels; the latter feature enables spatial manipulation of the maximum amplitude without the need to move the electrodes.
In mice, a 10-Hz envelope elicited neuronal firing at the same frequency, whereas neurons remained silent under high-frequency stimulation. The expression of c-fos (a marker of neuronal activation) increased in the stimulated target region, the hippocampus, but not in the overlying cortex beneath the electrodes (Fig. 1b), suggesting selective activation of the target region. Another mouse study demonstrated that tTIS targeting the superior colliculus (a deep brain structure critical for eye movement control) could induce eye movements and alter neural activity in the target region. These early rodent studies provide preliminary evidence thattTIS can modulate deep brain regions and induce behavioral changes in a region-specific manner.However, due to the larger head size, translating tTIS from rodents to human brains is not straightforward. The first step toward applying it to larger brains was testing this stimulation method in non-human primates, which demonstrated that tTIS can induce subthreshold modulation of neural activity in deep brain regions when using parameters compatible with human application.
These early animal study findings were corroborated by computational models (Fig. 1b). The simulation results support the following view:tTIS can evoke neural firing in the deep brain regions of rodents, and the stimulation site can be controlled by adjusting the current ratio between electrodes.Data from realistic human head models confirm that electric field strength decreases when stimulation is applied to larger heads. This precludes direct suprathreshold activation at intensities tolerable to the human body, while remaining compatible with subthreshold modulation. Individualized human brain information extracted from structural MRI also enables researchers to better examine inter-individual and inter-group variability, as well as the influence of neuronal orientation on electric field distribution, highlightingDetermining Optimal Electrode Placement and Current Intensity Based on Individual Anatomical Structuresits potential value.
Preliminary studies combining tTIS with human functional neuroimaging have provided evidence that tTIS can modulate the activity of deep brain structures such as the striatum and hippocampus (Figure 1b). These preliminary findings highlight several potential applications, including: the use of plasticity-inducing tTIS protocols to enhance deep brain activity and improve learning; the potential of this technology to intervene in specific deep brain rhythms to investigate their causal roles in behavior and brain function [58]; and the possibility of directing temporal interference fields to specific deep regions without moving electrodes.The application of tTIS is safe, well-tolerated, and facilitates effective blinding.Multiple other studies have also investigated the effects of tTIS on human cortical regions, confirming the feasibility and safety of this technique and demonstrating the potential to modulate different cortical areas, similar to traditional transcranial alternating current stimulation (tACS). Overall, these studies indicate that tTIS is a safe technology that offers the opportunity to selectively and non-invasively modulate deep brain activity and induce associated behavioral changes.
We believe that,tTIS provides an opportunity to gain a deeper understanding of the causal role of deep brain regions in specific human cognitive functions, as well as to investigate the pathophysiological mechanisms of neuropsychiatric disorders.Furthermore,tTIS may provide an alternative therapeutic strategy for the modulation of deep brain structures,These structures are involved in the pathophysiological processes, adaptive changes, or rehabilitation associated with neurological and psychiatric disorders. Another emerging technology—transcranial focused ultrasound stimulation (tFUS)—offers the possibility of non-invasive deep brain stimulation (DBS). tFUS employs low-intensity ultrasound for focused neuromodulation, a concept that has been extensively detailed in numerous topical reviews and thus falls beyond the scope of this perspective. We note that although the spatial resolution of temporal interference stimulation (tTIS) is at the centimeter scale (i.e., lower than the millimeter-scale resolution of tFUS along the transducer axis), its advantage lies in its ability to modulate well-characterized physiological electrical neuronal mechanisms. With clearly defined safety parameters, tolerability, and blinding efficacy characteristics, as well as established modeling workflows, tTIS is well-suited for large-scale, rapid clinical deployment.
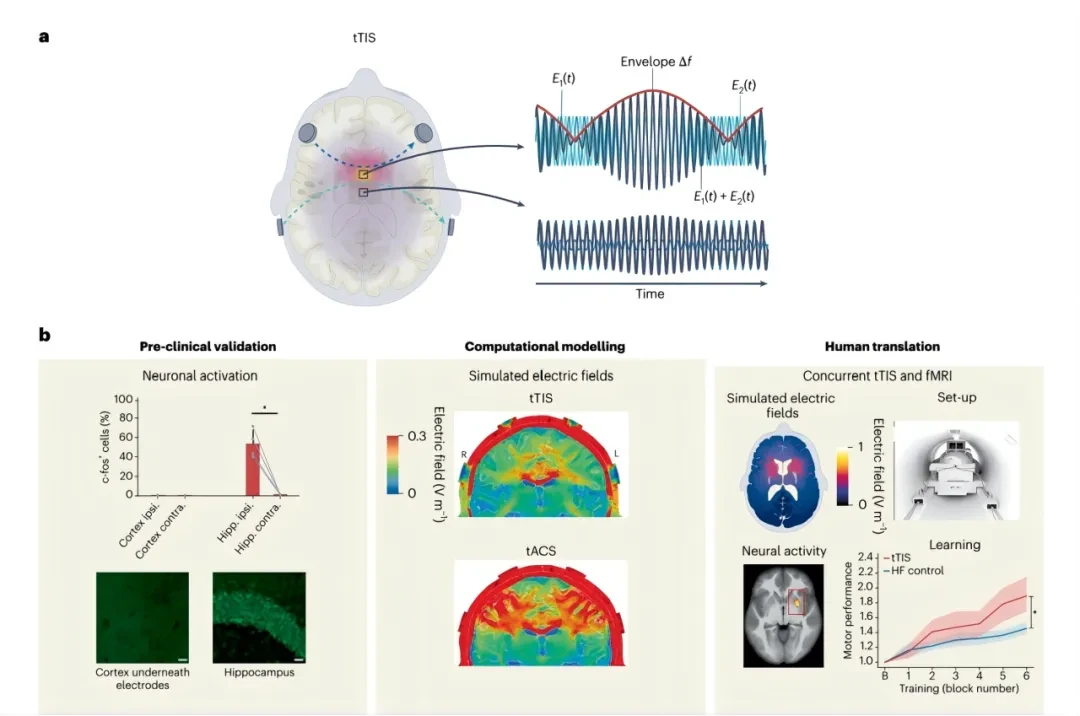
Figure 1. Concept and translational pathway of tTIS. a, Concept of tTIS. Left panel: A head model showing two pairs of electrodes with an applied current frequency difference of Δf. Right panel: Illustration of electric field interference at two different locations within the brain: one with higher envelope modulation (top) and one with lower envelope modulation (bottom). E1(t) and E2(t) represent the temporal modulation of field strength magnitude. b, Translational pathway of tTIS. Left panel: Following hippocampal tTIS, focal neuronal activation was observed in the stimulated (ipsilateral, ipsi.) hippocampus (Hipp.), whereas no activation was seen in the contralateral (contra.) hippocampus or the cortex beneath the electrodes. The lower images show the stimulated cortex (left) and hippocampus (right), respectively. Significance was analyzed using one-way ANOVA with Bonferroni post-hoc tests; asterisks indicate P < 0.00001. Data are presented as mean ± standard deviation. Middle panel: Computational modeling study based on a human head model, comparing tTIS electric fields with high-frequency carrier electric fields. Note that the upper part shows temporal interference exposure (amplitude modulation), while the lower part shows high-frequency alternating current exposure. Right panel: Based on a recent human validation study applying tTIS to the striatum during fMRI scanning with synchronized behavioral testing, improvements in motor learning and focal modulation of striatal activity were observed. B, baseline; HF, high frequency; L, left; R, right.
Next, we focus on tTIS, highlighting its prospects and potential challenges in both basic applications and clinical translation. First, we examine the applications of this technology, covering aspects ranging from basic neuroscience to clinical translation. Second, we outline some of the challenges facing this field, particularly concerningHypothetical Off-Target Effects, Stimulation Intensity, and Barriers to Clinical Deployment.Finally, in Part III, we discussPotential Neural Mechanisms of tTIS,and propose technical optimization solutions to enhance its effectiveness.
Neuroscience frequently employs lesion studies to investigate the causal role of specific brain regions in behavior. In humans, the study of patient H.M., who suffered bilateral hippocampal damage, revealed the region’s role in declarative memory and contributed to the formation of many theoretical models of memory function. Over the years, careful neuropsychological assessment of patients with focal lesions has yielded significant insights into inferring the causal roles of brain regions, greatly advancing our understanding of the neural correlates of various functions, including cognitive control, executive control, social behavior, language, motor control, learning, motivated behavior, and time perception. A parallel approach involves the systematic evaluation of brain regions through intracranial electrical stimulation. Modern neuroimaging strategies, such as lesion-symptom mapping and lesion-network mapping, have enabled the generalization of these findings by leveraging the diversity of lesion locations in large patient populations or by observing the effects of deep brain stimulation (DBS) targeted at specific implanted brain regions (e.g., in depression or movement disorders). However, the conclusions drawn from these studies may be confounded by neural alterations or compensatory mechanisms associated with the underlying pathology. Studying patients before and after predictable lesions—such as those resulting from resection surgery or expected neurodegenerative processes caused by genetic diseases—may provide valuable research models for inferring healthy brain function. Nevertheless, it remains challenging to completely exclude the influence of the underlying pathology on the observed effects. Overall, these research paradigms are limited by the fact that certain lesion locations are more prevalent than others (e.g., due to the vascular distribution of the nervous system in vascular lesions) and that DBS is implanted only in specific brain regions where therapeutic benefit has been established.
Non-invasive brain stimulation (NIBS) can be used to infer the causal role of specific brain regions in healthy behaviors. Through transcranial magnetic stimulation (TMS), researchers can apply focal, reversible perturbations to a specific brain region and investigate their effects on neural activity and behavior. Targeted brain stimulation satisfies most of the Bradford Hill criteria for causality, including temporality, specificity, experimental manipulation, counterfactual considerations, dose-response relationship, and reversibility. Such perturbations have yielded fruitful results in studying the causal contributions of brain regions to various functions, including motor control, motivational behavior, and visual perception. Although this approach can determine whether a specific region makes a causal contribution to a particular behavior, it does not provide information about the subsequent chain of neural events, such as the potential mediating roles of other regions within the network. Combining neuromodulation with simultaneous neuroimaging techniques (such as electroencephalography or functional magnetic resonance imaging) allows for the investigation of network effects induced by these perturbations. Beyond its value in basic research, this line of inquiry has advanced the development of repetitive transcranial magnetic stimulation (rTMS) therapy, which has been approved by the U.S. Food and Drug Administration for treatment-resistant depression, addiction, and obsessive-compulsive disorder. However, TMS primarily targets superficial (cortical) brain regions, as stimulation intensity attenuates with increasing depth of the target area. Consequently, even if certain TMS protocols can reach deeper structures, they invariably cause strong co-activation of the cortex, which may lead to unintended effects or complicate the interpretation of results.tTIS enables non-invasive, focal targeting of deep brain regions to investigate their causal roles in healthy cognition and behavior, without the robust cortical co-activation associated with traditional NIBS.In the following, we will highlight some core features of tTIS, including the potential for spatial steering and temporal selectivity, and explore how these aspects enable spatiotemporal targeting of deep brain regions.
The characteristics of tTIS include adjusting the intensity ratio between two pairs of electrodes (for example, each pair of electrodes has a peak-to-baseline value of 2mA, or one pair is 3mA and the other is 1mA), inControlling the Position of Maximum Electric Field Envelope Modulation Without Moving the Electrodescapability. Leveraging this concept, previous studies have demonstrated that distinct motor representations within the motor cortex can be activated without relocating electrodes. Similarly, a human neuroimaging study indicated that different regions of the hippocampus can be stimulated by altering the current ratio between two pairs of electrodes. This feature of temporal interference stimulation (tIS) holds several practical applications. First, it enables the comparison of experimental conditions targeting different deep brain (sub)regions without changing electrode positions, thereby allowing for cross-over designs across different brain regions while maintaining blinding integrity. This is not feasible with conventional transcranial electrical stimulation (tES) or transcranial magnetic stimulation (TMS) methods, as stimulating control regions requires separate repositioning of electrodes or coils, although multi-channel tES and TMS approaches utilizing electrode arrays and coil arrays, respectively, have recently emerged. Second,The guidance function can also adjust stimulus localization based on real-time activity during specific training phases (Fig. 2b), potentially in a closed-loop manner.Many behavioral functions involve time-varying processes, such as learning or fatigue, in which neural activity is not static but dynamically evolves across repeated trials. For instance, previous studies have shown that motor learning induces a shift in activity from the associative striatum to the sensorimotor striatum, presumably facilitating the automation of acquired motor skills. By directing temporal interference stimulation (tTIS) to specific regions of the striatum, one can investigate the causal roles of distinct striatal subregions at different stages of training. More broadly, this approach enables stage-specific modulation of deep brain regions based on their level of involvement in particular processes.
tTIS can rapidly trigger stimulation without causing the intense cutaneous sensations typically produced by conventional tES techniques when the current ramp-up time is less than 5–10 seconds.This is because the high-frequency carrier waves can ramp up with Δf = 0 at the onset of the task, after which a Δf is rapidly introduced by adjusting one of the high-frequency currents, thereby generating interference. This characteristic of tTIS makes it highly suitable for stimulating rapid, time-locked processes, such as reward processing, or for integration into closed-loop systems that require real-time triggering of stimulation based on specific neural signals. Furthermore, Δf can be set to specific frequencies, enabling the modulation of specific oscillatory activity patterns with distinct temporal dynamics (Fig. 2c). Consistent with the effects of tACS, applications of tTIS in non-human primates have demonstrated that it does not affect firing rates but rather modulates the spike timing of individual neurons. Under tTIS, some neurons become rhythmically synchronized, whereas the majority exhibit desynchronization at the envelope frequency. The propensity to induce synchronization or desynchronization may depend on various factors, including neuron type, initial synchronization level, envelope frequency, and stimulation intensity. Therefore, tTIS can be used to investigate the causal role of brain rhythms generated in deep brain structures by modulating the coordination of neural spiking associated with specific target frequencies. In humans, applying an 80 Hz envelope frequency to the striatum (a frequency associated with reinforcement learning in the rodent striatum) disrupted reinforced motor learning compared to a 20 Hz control condition, an effect accompanied by the suppression of striatal neural activity. Consistently, 20 minutes of tTIS targeting parieto-occipital alpha oscillations enhanced event-related alpha desynchronization in subjects performing mental rotation tasks post-stimulation. Thus, frequency-specific tTIS appears to be a promising tool for causally investigating the role of specific deep brain rhythms in human behavior. Another approach in basic neuroscience involves utilizing classic timing-specific, plasticity-inducing (or blocking) patterning protocols to modulate synaptic plasticity mechanisms in target regions, which has been studied in the rat motor cortex. Consistent with this, striatal tTIS delivered using an intermittent theta-burst stimulation pattern (a classic protocol known to induce long-term potentiation [LTP] in rodents) enhanced striatal activity and improved motor learning abilities in healthy adults. tTIS modulated task-evoked changes in striatal blood-oxygen-level-dependent (BOLD) signals but did not directly activate the region at rest. This method enables the manipulation of timing-specific plasticity mechanisms in deep brain areas to explore their causal roles, such as in various learning processes. Overall,tTIS can rapidly induce stimulation, making it suitable for targeting brief, time-specific processes; it can also target temporally specific deep oscillatory or plasticity mechanisms, thereby elucidating their causal roles in both health and disease.
Taken together, the spatial orientation and temporal selectivity of tTIS enable it to target deep neural mechanisms with specific (and potentially dynamically evolving) spatiotemporal characteristics, thereby facilitating the investigation of their functional roles in behavior. This stimulation modality can be combined with associative neuroimaging techniques to monitor intervention-related neural changes. For instance, applying tTIS to deep brain regions while concurrently performing fMRI can reveal neural alterations in the target area as well as connectivity modulation with connected brain regions. Furthermore, cortical tTIS has been employed to assess the lasting effects of stimulation on electrophysiological, electroencephalographic (EEG), or magnetoencephalographic (MEG) activity before and after intervention. Researchers are also striving to measure electrophysiological activity during tTIS by utilizing specific filters to remove stimulation artifacts. Theoretically, combining tTIS with other neuroimaging modalities, such as magnetic resonance spectroscopy or positron emission tomography, may further enhance our understanding of its neural effects. We believe that integrating tTIS with sophisticated behavioral paradigms and multimodal imaging technologies will be a crucial step toward better comprehending stimulation effects and ultimately establishing this technique within human neuroscience.
Overall, tTIS offers a non-invasive approach to locally stimulate deep brain regions to determine their causal roles in healthy individuals, thereby overcoming some limitations of invasive DBS or cortical NIBS. Spatially targeted and temporally selective tTIS stimulation of deep brain regions may yield new insights into the causal spatiotemporal mechanisms underlying various behaviors, including learning, motivation, memory formation, and executive control.
tTIS technology holds promise for advancing translational clinical research across multiple application areas, ranging from elucidating the pathophysiological mechanisms of neuropsychiatric disorders to developing innovative therapeutic strategies.
The safety and tolerability of tTIS have been explored at multiple levels.From cellular markers and computational models to the assessment of adverse events and pathological biomarkers. At the cellular level, evidence indicates that tTIS does not induce apoptotic activity, DNA damage, or immune responses when applied in mice. In humans, no adverse events have been reported, and tTIS has demonstrated good tolerability for targeting deep brain regions (such as the striatum and hippocampus) across more than 250 treatment sessions; reported sensations were limited to mild tingling, consistent with those observed in conventional tES. Furthermore, following cortical tTIS, neither evidence of epileptiform EEG activity nor elevation of neuron-specific enolase (a biomarker of neuronal injury) was observed. Previous tACS studies also support the safety of high-frequency electrical stimulation (up to at least 10 kHz) in humans. Finally, guidelines for the safe application of tTIS have been published based on extensive evaluations of electric field simulations and related parameters (i.e., current density and thermal effects). According to these metrics, peak-to-baseline current intensities are recommended not to exceed 3–5 mA and 15–30 mA within envelope frequencies typical of tES and DBS ranges, respectively, within which tTIS is considered safe. Therefore, these studies indicate that tTIS is safe and well-tolerated, supporting its use in larger-scale clinical trials. However, many unknowns remain in other aspects, such as the onset time, duration, and potential reversibility of effects. Combining tTIS with neural recording techniques such as EEG or MEG can deepen our understanding of these issues. Nevertheless, as most current evidence derives from a limited number of treatment sessions, further work is required to determine the safety of tTIS under longer exposure durations spanning several weeks.
To ensure clinical translation, tTIS must demonstrate robust blinding efficacy. Implementing appropriate control conditions—typically sham stimulation (usually involving rapid ramp-up and ramp-down of high-frequency currents) or high-frequency controls—is critical for clinical research and represents the gold standard for evaluating the efficacy of novel therapeutic strategies. In a dataset comprising over 100 participants and more than 250 trials, tTIS targeting deep brain regions (striatum or hippocampus) demonstrated comparable effects under both sham and active (high-frequency) control stimulation.Robust Blinding Efficiency,For example, high-frequency stimulation without frequency offset between stimulation channels. This lays an important foundation for the future clinical translation of tTIS.
Preliminary clinical data on tTIS indicate that in a study employing a double-blind design with a 130 Hz tACS control condition, 130 Hz tTIS stimulation of the substantia nigra in two patients with Parkinson’s disease and one patient with essential tremor reduced clinical tremor scores (assessed using Part III). Compared with invasive deep brain stimulation (DBS), this approach targeted an unconventional site. Subsequently, research shifted toward more classical DBS targets. In a randomized, double-blind, sham-controlled study involving patients with Parkinson’s disease (n = 12), 20 minutes of 130 Hz tTIS stimulation of the right globus pallidus internus was found to alleviate motor symptoms, particularly bradykinesia and tremor, resulting in a 6.64-point (14.7%) improvement in Part III scores. Another separately published, uncontrolled, unblinded case series (n = 8 patients with Parkinson’s disease) similarly reported positive effects of 130 Hz tTIS stimulation of the subthalamic nucleus (STN) on motor function, quantified using the same scale. Furthermore, recordings from the STN in eight patients with Parkinson’s disease demonstrated that tTIS targeting the STN could reduce pathological beta activity, with effects comparable to those of invasive DBS. Although these proof-of-concept studies of tTIS in patients with movement disorders are significant, many questions remain unresolved. A pilot cohort study involving 15 patients with traumatic brain injury has demonstrated the feasibility and blinding efficacy of tTIS targeting deep brain regions. Currently, multiple tTIS studies in clinical populations are underway. As of March 4, 2025, a search for “temporal interference stimulation” in the ClinicalTrials.gov database identified 19 studies covering various clinical conditions, including bipolar disorder, major depressive disorder, addiction, mild cognitive impairment, Alzheimer’s disease, and gambling disorder. These early data suggest that the application of tTIS in clinical populations is feasible. Current efforts are focused on better defining its potential efficacy for various neuropsychiatric disorders.
Based on the existing stimulation protocols,tTIS can be used to modulate neuroplasticity, synchronize oscillatory activity, or disrupt persistent pathological oscillations.(Fig. 2c). Therefore, tTIS not only helps to further elucidate the pathophysiological processes of neuropsychiatric disorders characterized by abnormal oscillatory activity (sometimes referred to as "oscillopathies"), but also serves as a therapeutic intervention to alleviate neurological symptoms by modulating abnormal brain activity. tTIS is complementary to other non-invasive brain stimulation (NIBS) methods, which will continue to play significant roles due to their distinct advantages; for instance, transcranial direct current stimulation (tDCS) is easy to operate and has established protocols for supervised home use, while transcranial magnetic stimulation (TMS)-based approaches enable supra-threshold stimulation.
Pathological brain states can manifest as dysfunction in neuronal plasticity across whole-brain networks. This characteristic is observed in various well-studied model diseases, including stroke, dystonia, depression, schizophrenia, addiction, post-traumatic stress disorder, and autism spectrum disorder. Recently developed patterned transcranial temporal interference stimulation (tTIS) protocols simulate plasticity-induction paradigms established in hippocampal slice preparations, such as intermittent or continuous theta-burst stimulation (TBS). Specific stimulation patterns can bidirectionally modulate synaptic plasticity according to their precise temporal structure, potentially through cellular mechanisms such as long-term potentiation (LTP) and long-term depression (LTD). Furthermore, this approach may also remodel abnormal brain network interactions.
First, the TBS-based tTIS approach helps elucidate the pathophysiological role of specific plasticity states (e.g., by investigating the functional role of activity in key deep brain regions during motor recovery after stroke). Multimodal methods combining functional neuroimaging and non-invasive brain stimulation (NIBS) have played a pivotal role in proposing hypotheses on cortical network plasticity and developing novel stimulation strategies. tTIS extends these investigations to critical deep brain hubs, such as the striatum or thalamus, and may further advance existing cortex-centric pathophysiological models.
Secondly, the TBS-mode tTIS can enhance training efficacy during motor rehabilitation. Compared with conventional techniques such as tDCS, tTIS can selectively target key regions of the deep-brain motor learning network, such as the striatum. This is crucial because the striatum plays a pivotal role in regulating transitions between different stages of motor learning. Here, the steering capability of tTIS holds promise for delivering precise, stage-specific stimulation (Fig. 2b), such as shifting the stimulation focus from the associative subregion to the sensorimotor subregion of the striatum during learning and recovery processes. This strategy is customizable and may help stabilize the therapeutic effects of neuromodulation-assisted motor training across different patients.
Pathological brain states may also be accompanied by attenuated oscillatory activity. A potential example is the reduction of gamma-band activity in Alzheimer’s disease. It remains unclear whether these changes in gamma activity play a causal role or are merely epiphenomena. However, in mouse models of Alzheimer’s disease, optogenetic gamma stimulation (40 Hz) has been shown to reduce the accumulation of beta-amyloid, a key pathological hallmark of Alzheimer’s disease. This finding was corroborated by a clinical study demonstrating that chronic 40 Hz audiovisual stimulation reduces brain atrophy, improves functional connectivity patterns, and enhances performance on memory recall tests in patients with mild Alzheimer’s disease. Furthermore, studies have indicated that 40 Hz transcranial alternating current stimulation (tACS) applied to the parietal cortex in Alzheimer’s patients with mild cognitive impairment can improve memory performance and cholinergic neurotransmission. In rodent models of Alzheimer’s disease, attenuated gamma rhythms in deep brain regions such as the hippocampus have also been observed. Therefore,γ-band tTIS stimulation of the hippocampus or other deep brain regions involved in the pathophysiology of Alzheimer’s disease (such as the amygdala) appears to be a promising research avenue.This synchronization strategy can also be employed to enhance beneficial oscillatory patterns in specific task-related states (for instance, by investigating the functional role of enhanced theta oscillations in episodic memory encoding and retrieval, and their subsequent reinforcement in therapeutic contexts). Compared with deep brain stimulation (DBS), the non-invasive nature of temporal interference stimulation (tTIS) facilitates the implementation of cross-species translational research designs that include both healthy subjects and patients with neurodegenerative diseases, thereby potentially paving a rapid pathway from laboratory to clinic.
Pathological brain states may also be induced by excessively strong oscillatory activity. An example of such a condition is the enhancement of beta activity in Parkinson’s disease. Oscillatory beta activity recorded from the subthalamic nucleus (STN) in patients with Parkinson’s disease correlates with the severity of akinesia-rigidity symptoms and can be attenuated by levodopa or invasive STN deep brain stimulation (DBS) therapy. A recent small-sample study (n=8) combining temporal interference stimulation (tTIS) with STN recordings demonstrated that tTIS targeted at the STN can reduce pathological beta activity, with effects similar to those of established therapies for Parkinson’s disease. Pathological beta activity in Parkinson’s disease does not appear to be unique to the STN; rather, it is thought to propagate throughout the cortico-basal ganglia network. Causal brain-behavior relationships have been preliminarily confirmed by applying beta-frequency stimulation to different brain targets using both non-invasive (e.g., transcranial alternating current stimulation, tACS) and invasive (e.g., DBS) methods. tTIS extends previous methodological approaches by enabling the non-invasive, simultaneous investigation of both cortical and deep nodes within the studied network. This approach allows for the perturbation and study of oscillations associated with deep brain regions in patients who do not have implanted DBS systems—including those in the early stages of the disease or those unsuitable for invasive DBS—as well as in healthy controls. As previously mentioned, tTIS can precisely target time-specific processes, such as delivering stimulation at a specific phase of the target oscillation, particularly within brain state-dependent interference paradigms. This can be achieved by rapidly adjusting Δf to trigger tTIS, thereby eliminating the long ramp-up and ramp-down intervals required by other transcranial electrical stimulation (tES) methods, such as tACS or transcranial direct current stimulation (tDCS).Opens up new opportunities for closed-loop non-invasive DBS.
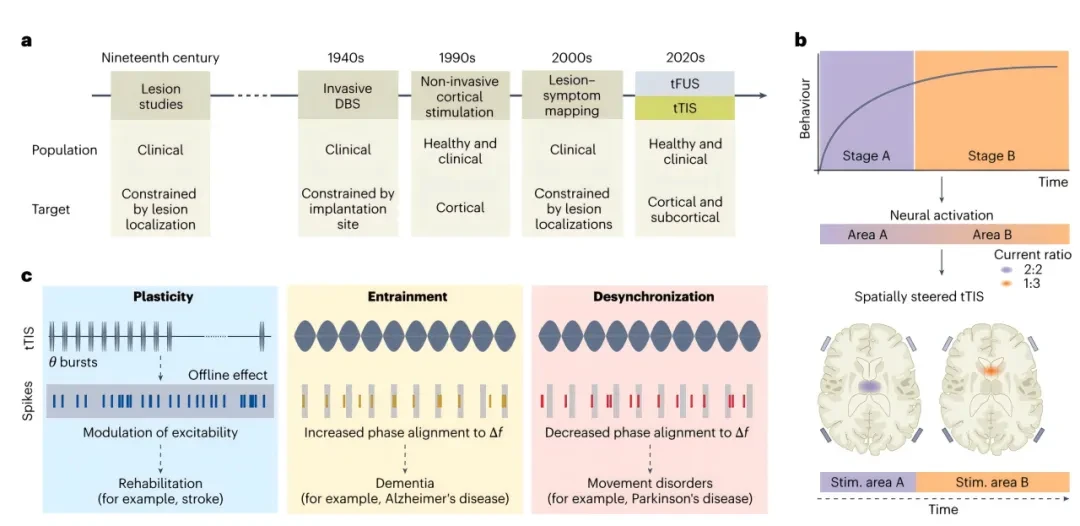
Figure 2. Basic and clinical application prospects. a, A brief history of causality in human neuroscience (non-exhaustive). The timeline lists experimental methods and techniques used since the 19th century to deepen the understanding of brain-behavior causal relationships. These methods vary in terms of the populations that can be studied (healthy subjects or patients) and the brain regions that can be examined (cortical or subcortical). tTIS involves focal, non-invasive electrical stimulation of cortical and deep brain regions in both healthy subjects and patients. tFUS also employs non-invasive deep brain stimulation but relies on ultrasonic neuromodulation with distinctly different mechanisms, and thus is not discussed in this perspective. Dates correspond to the approximate time when each technique was introduced in humans. b, The concept of stage-dependent spatial targeting. Consider a dynamic behavioral process; neural activity during tasks such as learning new skills is not static but changes with practice. tTIS can target different brain regions according to activity patterns associated with specific behavioral stages (e.g., early learning or performance plateaus) without moving electrodes. This facilitates the exploration of the causal dynamic roles of specific deep brain regions in certain behaviors. It should be noted that different envelope frequencies can target deep brain regions at their preferred operating frequencies in a stage-dependent manner. c, Targeting mechanisms of tTIS neuromodulation and potential clinical applications. Three distinct mechanisms of action for tTIS are proposed. Specific theta-burst stimulation patterns can induce plasticity in the target region, thereby modulating its excitability (left). Stimulation at specific envelope frequencies can induce rhythmic synchronization (center) or desynchronization (right), depending on factors such as the target region, neuron type, or the initial pattern of endogenous activity at that frequency. We emphasize that these three distinct concepts can be applied separately to different clinical areas, such as rehabilitation, dementia, or movement disorders.
Despite the high enthusiasm surrounding the development of tTIS since its initial proof-of-concept, and although numerous basic and clinical application prospects have been discussed above, tTIS technology still faces certain challenges (Figure 3).
Like other tES methods such as tACS, tDCS, or transcranial random noise stimulation,The intensity used in human applications of tTIS can only induce subthreshold—rather than suprathreshold—neuromodulation.The safety and tolerability of tES have been confirmed at intensities up to several milliamperes (with a conventional peak-to-baseline intensity of 4 mA for traditional tES), which generate electric field strengths of less than 1 V/m, resulting only in subthreshold neuromodulation. Preliminary evidence suggests that kilohertz-frequency stimulation may be safe and painless at intensities up to 10 mA. However, even such intensities are unlikely to produce suprathreshold neuromodulation, as this requires electric field strengths in the range of 10–200 V/m. Therefore, compared with invasive or non-invasive alternatives, an inherent limitation of tTIS is its inability to induce suprathreshold stimulation in humans. Nevertheless, TMS also cannot selectively deliver suprathreshold stimulation to deep brain regions, and the feasibility of achieving suprathreshold stimulation with tFUS in humans has not yet been demonstrated.
A key concept underpinning tTIS is that amplitude-modulated electric fields can modulate brain activity while minimizing off-target effects.Off-target effects may arise from neuromodulation induced when the high-frequency carrier is strongest at the cortical level.(see also Figure 1b). Previous studies have shown that when tTIS is applied at suprathreshold intensity in rodents, it can selectively induce hippocampal discharge without affecting the overlying tissues. However, this conclusion is based on electrophysiological and c-fos-related neural activation detection, which may fail to capture subtle changes in superficial neural activity. Computational model studies targeting peripheral axons and cortical neurons suggest that when tTIS is applied at suprathreshold intensity, it could theoretically cause off-target effects through conduction block induced by high-frequency carrier waves. Nevertheless, applying tTIS at suprathreshold intensity is not feasible in humans, as it would require an electric field of several hundred milliamperes, raising concerns regarding tolerability and safety.
The next question is: When tTIS is applied at subthreshold intensities (the intensity generally recommended for human use, with the peak-to-baseline intensity of conventional tES typically suggested to be ≤4 mA), can high-frequency carrier waves modulate neural activity? Simulations based on realistic cortical neuron models indicate that conduction block is unlikely to occur at subthreshold intensities, as the electric field strength required for this is four to five orders of magnitude higher than the electric field strengths commonly used in humans. Some experimental findings suggest that magnetic fields in the low-kilohertz range can modulate neuronal activity. However, even if it is assumed that the neuromodulatory effects of magnetic stimulation also rely on induced electric fields, the effects may differ from those of tES due to differences in the characteristics of the electric fields generated by these different methods, such as focality, directionality, intensity, and waveform. Regarding tES, one study tested the effects of low-kilohertz frequencies on cortical excitability in 11 healthy subjects and found that 1, 2, and 5 kHz tACS applied to the M1 region enhanced corticospinal excitability. We note that this contradicts the results of a combined human tTIS–fMRI study, which found no enhancement of BOLD signals in the cortical regions beneath the electrodes when using either striatal or hippocampal electrode configurations. More data are needed to resolve this discrepancy and to gain a clearer understanding of the potential effects of high-frequency electrical stimulation.
Meanwhile, appropriate control conditions need to be established to accurately interpret the effects of tTIS. Where feasible, we advocate adoptingActive control conditions, such as pure high-frequency controls, to isolate the specific effects of temporal interference components.When testing more than two conditions is feasible, a robust approach involves combining sham stimulation conditions (e.g., rapidly ramping high-frequency currents up and down to mimic tTIS-related sensations) with active controls (e.g., pure high-frequency stimulation; tTIS using a control ∆f frequency; or tTIS targeting a different anatomical region). This method helps rule out the potential influence of the high-frequency carrier signal on the observed effects and, depending on the experimental design, allows for conclusions regarding the frequency specificity and spatial selectivity of tTIS effects.
Compared with standard TMS, tACS, and tDCS, computational studies suggest that tTIS can achieve higher focality for deep brain targets. However, there is currently a lack of human experimental studies directly comparing the focality of tTIS with other techniques. Depending on the size of the target area, tTIS cannot achieve millimeter-level precision. Although focality can be optimized through technological advancements, other methods are already available to reach deep brain regions, such as deep TMS or tFUS. Deep TMS enhances penetration depth by improving the design of standard TMS coils, but this approach sacrifices focality for deeper penetration, limiting precise localization of structures such as the striatum or hippocampus while avoiding concomitant cortical activation. In contrast, tFUS utilizes ultrasound with high tissue penetrability to modulate deep brain regions with higher spatial resolution than existing tTIS protocols, achieving millimeter-level focality along the transducer axis. Although tFUS offers higher focality than tTIS, its effectiveness is highly dependent on individual head characteristics, such as skull thickness and composition. Therefore, tFUS is more sensitive to individual differences; even a 0.1 mm difference in scalp thickness can affect the final target. This sensitivity to minor variations in anatomy and transducer positioning may pose challenges to the large-scale clinical deployment of tFUS. The choice between tTIS and other non-invasive alternatives (such as tFUS or deep TMS) may depend on the specific application, requiring comprehensive consideration of multiple factors, including required focality and stimulation intensity, accessibility of imaging data and modeling platforms (to account for individual anatomical differences), and economic factors. Currently, efforts are being made to enhance focality through technical means, such as adopting multi-channel or synergistic activation strategies (Figure 3).
Identifying effective protocols is a key challenge in translating temporal interference stimulation (tTIS) into clinical trials and future applications. Invasive deep brain stimulation (DBS) employs pulsed, suprathreshold stimulation, whereas conventional non-invasive tTIS relies on subthreshold, sinusoidal stimulation, making direct one-to-one translation of established protocols difficult. For instance, in the aforementioned application case for Parkinson’s disease, employing desynchronization protocols to disrupt pathophysiologically relevant oscillatory features (such as excessive beta oscillations) may be more effective than attempting to mimic the 130 Hz frequency used in invasive DBS.
The process of bringing emerging neurotechnologies to market has historically been inefficient, likely due to numerous challenges and barriers in the translation process, including medical and R&D economics, unclear mechanisms of action, regulatory hurdles, and acceptance by clinicians and patients. tTIS technology is likely to encounter similar obstacles. It is estimated that the cost to bring a non-invasive general-purpose device to market is approximately $10 million over four years, whereas the cost for an invasive product is around $100 million over ten years. Many neurotechnology-based therapies suffer from low adoption rates; for example, in Parkinson’s disease, fewer than 15% of eligible patients receive deep brain stimulation (DBS) therapy. There is no single solution to address these challenges. Potential approaches include conducting comprehensive translational mechanism research, coordinating broad collaborative initiatives (possibly through open-source databases), or strengthening industry-academia-research collaboration.
To fully realize the potential of temporal interference stimulation (tTIS) in basic neuroscience and clinical neuropsychiatry, we need to better understand the neuronal mechanisms that can be targeted in pathology and optimize the technology. Since electrical brain stimulation induces cutaneous sensations, the intensity used in tTIS is limited to a few milliamperes, thereby producing only subthreshold neuromodulation. Accordingly, we will focus exclusively on the mechanisms of subthreshold tTIS applied in humans, without discussing other hypothetical mechanisms associated with suprathreshold stimulation, which only occur when tTIS is administered at higher intensities in animal experiments or computational studies.
Similar to other tES techniques,Neuromodulation by subthreshold tTIS may occur via neuronal membrane polarization.tDCS and tACS primarily modulate the likelihood and timing of endogenous action potentials, which may have profound effects on synaptic efficacy and network synchronization. Recent computational and primate studies suggest that subthreshold tTIS operates via similar mechanisms. It has been proposed thattTIS biases the timing of neuronal firing but does not modulate the average firing rate.More specifically, although some neurons are synchronized at the envelope frequency, most neurons exhibit desynchronization, and this effect depends on the baseline synchronization level of the neurons, which is similar to the case with tACS. Therefore,One possible mechanism of tTIS is to modulate synchronization or desynchronization at the envelope frequency based on the initial activity patterns of neurons.It may also depend on the relative phase difference between endogenous rhythms and the applied stimuli, as is the case with tACS. Other factors may also play a role, such as the type and morphology of target neurons, their orientation relative to the electric field, and the density of specific neuronal compartments (e.g., soma or axons) within the stimulated region. These factors suggest that, like other forms of tES,The sensitivity to tTIS may depend on the initial endogenous activity patterns of the target region, but also on its structural characteristics.The relationship between endogenous activity (potentially task-induced) and tTIS responsiveness remains to be investigated, possibly using electrophysiological methods such as calcium imaging or stereoelectroencephalography in preclinical models, and scalp electroencephalography or magnetoencephalography in humans. These data will clarify which brain states are more likely to respond to tTIS and pave the way for functionally targeted stimulation of regions exhibiting specific activity patterns during tasks, ultimately enhancing the spatial resolution of tTIS.
Modeling and experimental studies indicate that although temporal interference stimulation (tTIS) can elicit neuronal effects at clinically relevant electric field strengths (~0.4–1.0 V m⁻¹), these effects may be weaker at the cortical level compared to conventional transcranial alternating current stimulation (tACS), particularly as the carrier frequency increases. Furthermore, unlike conventional tACS, tTIS consists of pure high-frequency components amplitude-modulated at a low frequency Δf. Consequently, neurons must demodulate the signal to extract the envelope frequency—a process achievable through frequency mixing. However, recent evidence suggests that this demodulation comes at a cost; even when accounting for current shunting, tTIS-induced responses remain weaker than those elicited by tACS, likely because neurons cannot fully demodulate the amplitude-modulated waveform. The attenuated response to tTIS can be partially offset by its higher tolerability, which permits stimulation at higher intensities. Indeed, a recent study demonstrated that tolerability increases with carrier frequency, with the perceptual threshold for 2 kHz stimulation being tenfold higher than that for standard tACS. The pain threshold for kilohertz stimulation is also substantially higher, reaching a peak intensity of 3.8 mA at 2 kHz, compared to 0.5 mA for conventional 10 Hz tACS. Thus, it is possible to leverage the superior tolerability of tTIS to deliver stimulation at intensities unattainable with standard tACS, even with the use of topical anesthetics. These preliminary data suggest that the kilohertz components of tTIS require higher-intensity stimulation to achieve neuronal effects and efficacy comparable to tACS—a challenge that can be addressed by the greater tolerability of kilohertz electric fields.
Although other mechanisms for supra-threshold tTIS may exist in animals, a key mechanism for sub-threshold tTIS is the demodulation of amplitude-modulated high-frequency electric fields. Recent evidence suggests that this process can occur at the single-cell level through ion channel-mediated mechanisms. It is generally believed that responsiveness to tTIS requires an ion channel-mediated rectification process prior to low-pass filtering. This rectification may arise from a temporal kinetic mismatch between fast inward depolarizing sodium currents and slower outward repolarizing potassium currents. Within this framework, neurons respond to tTIS if the slope of the amplitude-modulated electric field is sufficient to generate this inward-outward current imbalance, thereby bringing the membrane potential closer to the depolarization threshold. Consistent with this, computational modeling indicates that responsiveness to tTIS decreases as the membrane polarization time constant increases, confirming that the key determinants of tTIS responsiveness are indeed the rapid membrane polarization dynamics in target neurons and neuron-specific gating properties, such as the time constant. The specific role of sodium channel dynamics in tTIS sensitivity is further corroborated by the fact that pharmacological blockade of voltage-gated sodium channels abolishes tTIS-mediated membrane potential modulation, whereas no such effect is observed when blocking synaptic NMDA, AMPA, and GABA-A receptors, suggesting a degree of selectivity in the cellular mechanisms underlying tTIS. Therefore, these early mechanistic findings suggest thatThe dynamics of specific ion channels on the neuronal membrane underpin tTIS electric field demodulation, ultimately achieving subthreshold membrane polarization.An important direction for future research is to identify neurons that demodulate more efficiently and are therefore more sensitive to tTIS electric fields. In vitro studies applying suprathreshold tTIS to cortical neurons suggest that different cell types exhibit varying responsiveness to tTIS (for example, excitatory pyramidal neurons respond more strongly than parvalbumin-expressing inhibitory neurons), but this responsiveness largely depends on network interactions between inhibitory and excitatory neurons. To gain a deeper understanding of the responsiveness of different cell types to tTIS under in vivo conditions (including at subthreshold intensities), optogenetics (possibly combined with fMRI) can be employed in rodents, or spectroscopic methods can be used in humans.
Overall, subthreshold-intensity transcranial temporal interference stimulation (tTIS) neuromodulation applied in humans is considered to rely on membrane polarization modulation that primarily affects the timing of neuronal firing. Compared with transcranial alternating current stimulation (tACS), responsiveness to tTIS requires a demodulation process dependent on the temporal dynamics of ion channels on the cell membrane, which may attenuate the neuromodulatory effects but can be compensated for by the potentially higher focality and higher intensities tolerable with tTIS. Understanding the factors influencing the responsiveness of specific brain regions and neuron types to specific tTIS electric fields is a key avenue for further optimizing this technology and enhancing its efficacy.
Computational studies have demonstrated that, in both animals and humans, temporal interference stimulation (tTIS) exhibits higher focality than standard transcranial alternating current stimulation (tACS), enabling access to deep brain targets. Nevertheless, there remains room for optimization, whereby focality can be further enhanced by reducing off-target electric fields. Studies using cortical models and primate brains have revealed that the effects of tTIS are weaker than those of conventional tACS, and the intensity required to modulate neural activity increases with higher carrier frequencies. Building on these findings, technical optimizations of tTIS can be achieved by enhancing stimulus focality and neuronal effects in the target region.
When considering the focality of tTIS and the responsiveness to tTIS,It is necessary to consider the influence of individual anatomical structures, morphology, and connectivity on the electric field distribution of tTIS.Most studies employ preset electrode montages optimized for template heads. Although effective envelope modulation can be achieved in the target region, these approaches fail to account for inter-individual differences in brain properties. More precise head modeling can be realized by adjusting electrode size and shape according to individual geometric structures and incorporating specific anatomical features. Group-level studies have shown that the focality of electric fields generated by the same electrode montage varies across subjects. Magnetic resonance imaging (MRI) provides critical information on brain properties, such as morphology, degree of atrophy, and fiber orientation, which influence electric field distribution and can be used to reduce inter-subject variability. Individual anatomical structures can also inform electrode design, which has been proven to affect stimulation outcomes in standard transcranial electrical stimulation (tES) techniques. Current density and field distribution are fundamentally determined by electrode size and placement. However, personalized modeling incurs high logistical and computational costs, requiring expensive MRI acquisitions and substantial computation time to simulate electric fields for various electrode montages to identify optimal configurations. Therefore, it is crucial to investigate the extent to which temporal interference stimulation (tTIS) applications benefit from personalization. Some studies have found that models based on individual MRI scans exhibit better target exposure than those generated from templates, and that the orientation relative to the target structure also influences tTIS effects. Other studies indicate that inter-subject variability in electric fields is lower than the variability in blood oxygen level-dependent (BOLD) signals associated with functional brain activity, suggesting that personalization may not be necessary. These studies have primarily focused on healthy brains. A key step in translating this technology to clinical applications involves not only exploring inter-individual differences in healthy populations but also investigating pathology-related brain changes, such as lesions or atrophy known to affect electric field distribution. Future research should clarify the differential impacts of personalized versus template-based models in both healthy and pathological brains, with particular emphasis on assessing behavioral outcomes (Figure 3).
Another approach to enhancing the focus of deep neural modulation is to applyMulti-channel tTIS(Figure 3), utilizing a greater number of electrode pairs. Preliminary studies using computational models have demonstrated that, compared to standard stimulation with two pairs of electrodes, stimulation using multiple electrode pairs can reduce off-target electric fields, with focusing precision improving as the number of electrode pairs increases. This has been confirmed in mice, where the application of six-channel transcranial Temporal Interference Stimulation (tTIS) to the primary motor cortex enhanced focality, reduced sensory sensations, and mitigated the impact of variability in electrode placement. Furthermore, a third electrode pair can be employed as a phase-canceling field to target specific off-target regions, thereby minimizing unintended modulation. Reported standard multi-channel tTIS variants include the use of electrode arrays or the replacement of discrete electrode pairs with patch electrodes to improve stimulation precision. However, adjusting parameters beyond merely changing the number of electrodes is more effective in reducing unintended envelope modulation outside the target region. Another proposed method is multi-modulation synthesis, wherein different channels deliver stimulation with varying timing, frequencies, and polarities. For all the aforementioned applications, particular attention must be paid to potential unnecessary stimulation caused by interference fields arising from additional electric fields introduced by the head, as well as shunting effects that may result from excessively close electrode spacing. Specific algorithms can help balance focality and computation time, determine the optimal number of electrodes, and simultaneously minimize off-target modulation and shunting effects while ensuring the feasibility of electrode mounting.
Subcutaneous electrode placement enables extracranial stimulation, enhancing electric field intensity in the target region while maintaining minimal invasiveness (Figure 3). This approach mitigates current attenuation caused by the skin and muscles, which are primary contributors to the shunting effect. This consideration is particularly critical for temporal interference stimulation (tTIS), as evidence indicates that such shunting effects intensify with increasing frequency. Subcutaneous placement also improves the consistency of electrode positioning, facilitating repeated and prolonged stimulation sessions. Animal studies have demonstrated that extracranial stimulation of cortical targets using pulsed currents is safe, achieving electric field intensities an order of magnitude higher than those produced by transcranial electrical stimulation (tES) with standard surface electrodes. Initial human applications have confirmed the safety and efficacy of this method in patients with epilepsy, with no long-term complications observed. Electrode depth and tissue contact are two key variables in reducing current shunting. To enhance intracerebral electric field intensity, the conductive portion of the electrode should be positioned at the level of the subcutaneous fat layer, avoiding contact with the epidermis.Extracranial tTIS represents a promising direction for this technology, offering both higher intensity and minimal invasiveness, making it highly suitable for clinical applications.
Stimulus focality can be enhanced and neuronal effects optimized through study design. Due to the subthreshold nature of human tTIS, modulation of brain region activity in the resting state may be difficult to achieve.Pre-activation of the target area can enhance the effect in that region,In contrast, the effects on surrounding regions exposed to similar tTIS electric fields are limited. Behavioral tasks can be employed for this purpose to induce task-related activity in the target area. Specific experimental paradigms can further enhance the focality of stimulation by selectively activating a subregion of the target area, thereby optimizing electrode placement without the need for additional re-optimization. A recent study provided an example: applying tTIS to the bilateral striatum enhanced the selectivity of BOLD activity in a subregion (the putamen) that already exhibited higher task-related activity under control conditions, with this enhancement effect being specifically contralateral to the executing hand. Furthermore, combining tTIS with other stimulation techniques, such as TMS or tFUS, can achieve similar effects by pre-activating deep structures. TMS has been used to indirectly target deep structures by stimulating connected cortical regions, demonstrating its influence on network activities involved in associative memory, attention, and motor control. Modulating cortical seed points via TMS can initiate activity in deep structures or induce plastic changes, subsequently causing alterations in connected regions within the same network. Conversely, direct pre-activation of deep brain regions can also be achieved through tFUS, another promising method for focal intervention in deep structures (Figure 3).
Various alternative stimulation protocols have been explored to implement tTIS more effectively (Figure 3). In current applications, two distinct approaches have primarily emerged:Frequency-Specific Stimulation and TBS-Patterned Stimulation.The former applies an envelope at a constant frequency, with mechanisms analogous to the rhythmic resonance or synchronization effects of transcranial alternating current stimulation (tACS). This approach yields varying neuromodulatory effects depending on current intensity, neuronal subtype responsiveness, and individual endogenous activity in the target region. Although the underlying mechanisms of temporal interference stimulation (TIS) may differ substantially due to the need to extract the envelope frequency, several parameters of the stimulation protocol can be adjusted according to the target region and functional objectives. Another challenge in studying TIS while accounting for endogenous activity is the lack of non-invasive methods for directly recording deep brain activity. The second approach employs theta-burst stimulation (TBS)-patterned TIS to replicate plasticity effects similar to long-term potentiation (LTP) and long-term depression (LTD). This protocol was initially tested in hippocampal slices and subsequently translated to humans using transcranial magnetic stimulation (TMS). Although such effects may exhibit lower dependence on specific frequencies, LTP- and LTD-like effects in humans are difficult to investigate and may vary across different brain structures.
Currently, several variants have been derived from these two initial protocols to optimize stimulation efficacy.Phase-Modulated tTISThis approach can serve as an improvement to enhance temporal control over the interfering electric field and generate a pulse-like envelope to replace the sinusoidal envelope. In this scheme, two pairs of electrodes output the same current frequency, with a phase transient of specific duration introduced in one pair. To better align with clinical protocols,Pulse Width Modulation tTISIt was also tested in animal models of epilepsy and demonstrated a reduction in epileptogenic biomarkers. In this application, biphasic square-wave pulses were used to replace sinusoidal waveforms, yielding neuromodulatory effects comparable to or stronger than those of standard tTIS, which may be attributed to the higher energy carried by the square waves. Meanwhile,Multi-point tTISProposed to increase the number of stimulation sites with the aim of achieving network modulation. This method assigns two different carrier frequencies to each pair of electrodes while maintaining a four-electrode configuration, and forms two interference sites through different current ratios within each carrier: one derived from the interference of the first carrier frequency, and the other from the interference of the second carrier frequency. This technique enables multi-point stimulation without the need for additional electrodes.The concept of temporal interference has also been extended to other non-invasive brain stimulation techniques, such as TMS.Computational studies and rodent experiments have both demonstrated promising results. However, further research is needed to gain a deeper understanding of the mechanisms, effects, and feasibility of temporally interfering TMS. Several key issues are shared between tTIS and temporally interfering TMS, such as focality, optimization of electrode/coil configurations, and high-frequency effects. Feasibility-related challenges must be addressed, including potential system overheating and coil-dependent attenuation of the electric field with depth. Given that TMS intensities are higher than those of tES, the potential for conduction block effects should also be carefully investigated.
Compared with traditional NIBS, tTIS not only provides greater focusing in deep brain regions, but also possessesSimultaneously record brain activitypotential. By leveraging EEG, MEG, DBS recordings, and in vitro neuronal recordings on chips respectively, the understanding of NIBS can be elucidated from the network level down to single-neuron resolution. The latter has recently been explored in combination with tTIS to better understand its effects on different types of neurons. In contrast, macroscopic recordings such as EEG, MEG, and DBS are known to be severely affected by artifacts when combined with conventional tACS, because the frequencies of interest during recording often coincide with the stimulation frequency. Consequently, the signals become dominated by the frequency of the injected current, thereby masking natural oscillatory patterns. Since the high carrier frequencies used in tTIS exceed the frequency range of endogenous brain activity, recording during tTIS can theoretically avoid stimulation artifacts. However, practical challenges remain, as system nonlinearities may introduce unwanted artifacts, particularly at the difference frequency of the two carriers. These artifacts can be mitigated and reduced below the noise floor through additional hardware (utilizing low-pass and high-pass filters), but the design of these components requires testing, and tailored protocols are needed to distinguish brain responses from stimulation artifacts.
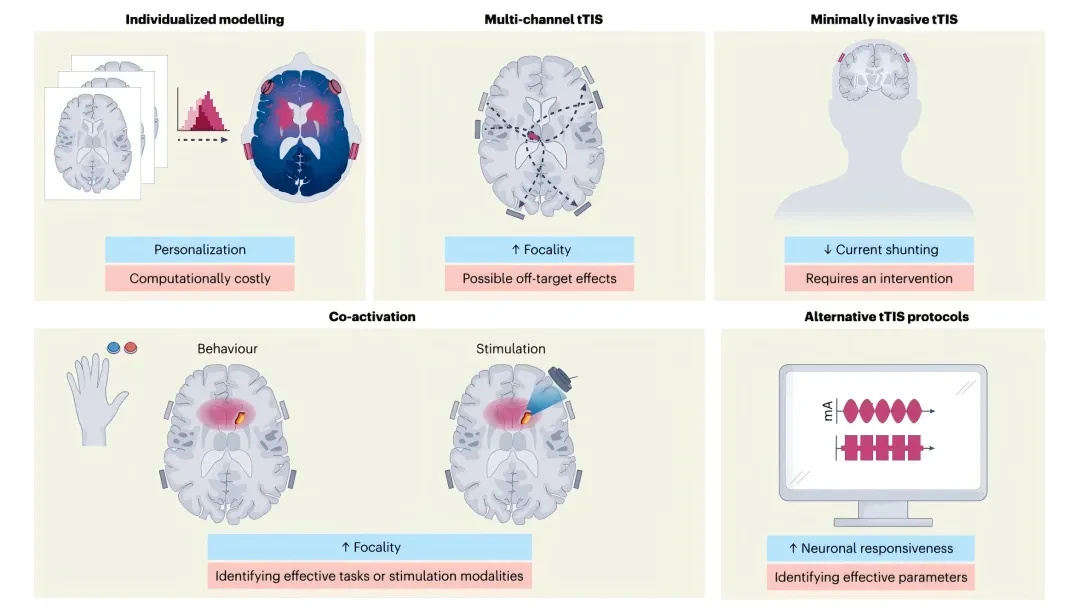
Figure 3. Schematic diagram of the proposed optimization strategy for tTIS technology. Technical improvements to the currently used tTIS protocol can enhance its focality. These optimizations include: (1) personalized modeling based on individual imaging data; (2) increasing the number of electrodes to enhance amplitude modulation within a smaller target region; (3) employing extracranial electrodes to reduce current shunting effects; (4) pre-activating the target region through behavioral tasks or via concurrent external brain stimulation techniques (such as transcranial focused ultrasound, tFUS, or transcranial magnetic stimulation, TMS); and (5) refining stimulation parameters, such as waveform shape or stimulation timing, according to different brain regions and task characteristics.
tTIS is a promising non-invasive method for electrical modulation of deep brain regions, offering excellent focality and opening new possibilities for fundamental systems neuroscience and clinical translational applications.We explored how to leverage some of the core features of tTIS—including spatially guided stimulation, rapid-triggered stimulation, and modulation of specific neural processes (such as neural oscillations or plasticity mechanisms) without the need to move electrodesthe potential to address key neuroscience questions and design alternative intervention strategies for neuropsychiatric disorders. We present the putative mechanisms of action, possible technological advancements, and unresolved issues in the field of tTIS neuromodulation, and argue thattTIS can establish itself as a non-invasive, precise deep brain stimulation technique.
References
Vassiliadis P, Beanato E, Wessel MJ, Hummel FC. Temporal interference stimulation for deep brain neuromodulation in humans. Nat Biomed Eng. 2026 May 19. doi: 10.1038/s41551-026-01665-z. Epub ahead of print. PMID: 42157014.



Contact & Consultation

WeChat Official Account
Neurodome
Pioneer in Non-Invasive Deep Brain Neuromodulation

Tel: 400-629-2019
Email info@neurodomers.com