Naturally Selected CD7 CAR-T Therapy without Genetic Manipulations Demonstrates Safety and Efficacy in Relapsed/Refractory T-ALL/LBL: First-in-Human Phase I Trial Published in Blood

Senlang
Developer of Novel Anti-Tumor Bio-Immunotherapy Drugs

Peking University People's Hospital
Modern Comprehensive Tertiary Grade A Hospital
Beijing, May 8, 2022 /PRNewswire/ -- On May 2, 2022, the team of Professor Lu Peihua (first author and co-corresponding author) from Lu Daopei Hospital, the team of Professor Li Jianqiang (co-corresponding author) from Hebei Senlang Biotechnology Co., Ltd. ("Senlangbio") (Liu Ying, co-first author), and Professor Huang Xiaojun (co-corresponding author) from Peking University People's Hospital collaborated in...International authoritative journal in hematologyBlood(IF=23.63) published a paper titledNaturally Selected CD7 CAR-T Therapy without Genetic Manipulations for T-ALL/LBL: First-in-human Phase I Clinical Trial Research Paper.
Acute T-cell lymphoblastic leukemia (T-ALL) and T-cell lymphoblastic lymphoma (T-LBL) are highly aggressive T-lineage malignancies. Due to the shared antigenicity between normal T cells and malignant T cells, there is still a lack of approved CAR-T therapies specifically targeting T-cell malignancies.
CD7 is highly expressed on the surface of T-ALL/LBL T cells and is a potential CAR-T therapeutic target.Targeted CD7 immunotherapy may be affected by the T-cell fratricide mechanism. Therefore, in previous studies, CRISPR/Cas9 gene editing technology and protein silencing expression techniques have been used to produce CD7-targeting CAR-T cells. However, gene editing technology increases the production cost of CD7 CAR-T cells. Additionally, manufacturing CD7 CAR-T cells using autologous T cells from patients remains challenging. Although donor-derived or universal CD7 CAR-T cells are an option, issues such as finding suitable donors, the expansion capacity of allogeneic CAR-T cells in vivo, and their persistence still need to be addressed.
In response to the above challenges,This study explores the use of patient- or donor-derived products developed by Senlangbio, without the need for additional...A New Product of "Naturally Selected" CD7 CAR-T Cells (NS7CAR) with CD7 Gene Editing or Protein Expression Blocking, and for the first time explored the safety and efficacy of NS7CAR therapy in humans in a phase 1 clinical trial targeting patients with T-ALL/LBL.
Preclinical Research
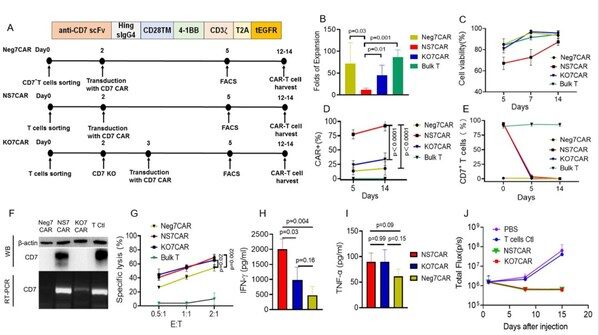
Researchers used three different methods to generate CD7-targeted CAR-T cells and compared their functions: 1) NS7CAR: Obtained by transducing total T cells with 7CAR followed by a "natural selection" cell culture process; 2) Neg7CAR: Produced by purifying and transducing naturally occurring CD7-negative T cells (which account for 3%-10% of CD3+ T cells) with 7CAR; 3) KO7CAR: Generated by transducing 7CAR into total T cells where the CD7 gene was knocked out using CRISPR/Cas9 RNP.
During the 2-week culture period, the cell expansion fold of NS7CAR was significantly lower than that of Neg7CAR and KO7CAR. However, 87.3% of NS7CAR cells were viable, making further research possible. At harvest, an average of 92.4% of T cells in the NS7CAR group expressed the 7CAR molecule, significantly higher than in Neg7CAR or KO7CAR (p<0.0001). Three days after 7CAR lentiviral transduction, the T cells in the NS7CAR group underwent a rapid and significant phenotypic shift from CD7+CAR- to CD7-CAR+.
An interesting finding is that, despite the absence of CD7 surface expression detected by flow cytometry in NS7CAR T cells after in vitro culture, significant CD7 mRNA and protein expression were detected using RT-PCR and Western Blot. Meanwhile, no CD7 mRNA or protein expression was observed in Neg7CAR or KO7CAR cells. These results indicate that although NS7CAR expresses CD7 mRNA and protein, they are immunologically CD7-negative and escape fratricidal cell killing mechanisms due to antigen masking/intracellular sequestration by CD7CAR. This was further confirmed in subsequent clinical studies by the persistent detection of CD7 mRNA expression in NS7CAR within patients on day 28 post CAR-T infusion. Additionally, compared to Neg7CAR and KO7CAR, NS7CAR contained a higher proportion of the CD8+ subset and central memory phenotype subset.
In vitro anti-leukemia experiments showed that both NS7CAR and KO7CAR exhibited significant cytotoxicity against CCRF-CEM cells, releasing high levels of IFN-γ and TNF-α, while the corresponding values for Neg7CAR cells were relatively low. In animal experiments, both NS7CAR and KO7CAR significantly reduced leukemia burden in mouse models within the first two weeks after CAR-T injection. These data demonstrate the feasibility of generating effective CD7CAR-T cells directly from total T cells transduced with 7CAR without additional gene editing. Therefore, the Lu Daopei medical team utilized NS7CAR-T cells in a Phase 1 clinical trial to further explore their efficacy and safety.
Clinical Research
‖Study Design
This is an open-label, single-arm phase 1 clinical study aimed at evaluating the safety and efficacy of NS7CAR in patients with CD7+ R/R T-ALL or T-LBL. Enrollment criteria include patients aged between 2 and 65 years who have failed at least two prior lines of therapy and have CD7 expression ≥80%. After day 28 post-NS7CAR infusion, consolidative allogeneic hematopoietic stem cell transplantation is permitted based on the physician’s consideration and the patient’s willingness.
‖Baseline Data of Patients
In this clinical trial, a total of 20 patients with relapsed or refractory (R/R) T-ALL/T-LBL were enrolled and received reinfusion, including 14 R/R T-ALL patients and 6 R/R T-LBL patients. Three patients had high-risk subtypes such as Ph-positive or ETP-ALL; 11 patients exhibited high-risk mutations or gene fusions. Five patients had undergone transplantation prior to enrollment. The patients received a median of 4.5 lines of treatment. At the time of enrollment, the median percentage of bone marrow tumor cells in 17 patients was 21.49%; no tumor cells were detected in the bone marrow of three T-LBL patients. Five T-LBL patients and four T-ALL patients had extramedullary lesions, with three having central nervous system involvement.
‖Clinical Product Preparation and Infusion
The study applied the NS7CAR product derived from patients or their transplant donors. For patients who had not undergone allogeneic transplantation, autologous CAR-T cells were used; for patients in a post-transplant relapse state at enrollment, the use of either patient-derived autologous or donor-derived CAR-T cells was determined after a comprehensive evaluation of the patient. The NS7CAR products for all patients were successfully manufactured (autologous source, n=18; donor source, n=2), with a median transfection efficiency of 95.10%. The NS7CAR product contained a higher CD8+ subpopulation, with a median CD4/CD8 ratio of 0.42. On Day 0, 3, 16, and 1 patients received low doses (0.5×106/kg), medium dose (1-1.5×106/kg) or high dose (2×106/kg) of a single NS7CAR infusion.
‖Efficacy and Safety
NS7CAR Demonstrates Good Safety and Tolerability. One patient did not experience CRS; 18 patients had CRS ≤ grade 2, with only one patient experiencing grade 3 CRS. Two patients developed grade 1 ICANS.
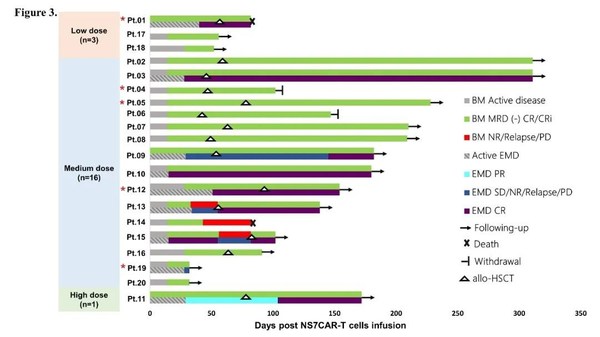
Meanwhile, NS7CAR has demonstrated exciting efficacy in clinical trials. By Day 28, 16 out of 17 (94.12%) patients with bone marrow involvement achieved MRD-negative complete remission (CR); the three patients with only extramedullary lesions of T-LBL remained in a state of intramedullary CRi. Among the nine patients with extramedullary lesions, five reached extramedullary CR at a median time of 29 days. Two patients with large mediastinal masses (>7cm) achieved partial response (PR) and stable disease (SD), respectively, on Day 29; the PR patient's extramedullary lesion further reduced by Day 104. Two patients with central nervous system infiltration also achieved CR on Days 15 and 28, respectively.
As of the study cutoff date (October 25, 2021), the median follow-up time for patients was 142.5 days, with the longest being 311 days. Six out of 20 patients did not receive additional anti-leukemia treatment or transplantation after CAR-T cell infusion, and four of them remained progression-free at a median time of 54 days. At a median time of 57.5 days post-infusion, 10 patients in complete remission (CR) underwent consolidative bridge transplantation; the median follow-up time after transplantation was 210 days, with 7/10 CR patients remaining minimal residual disease (MRD)-negative and continuing to survive. Two patients withdrew from the study for personal reasons while both were in CR. One patient underwent a second transplant, developed grade 3 acute graft-versus-host disease (aGvHD), and subsequently passed away. Four patients who did not achieve CR or relapsed after CR received salvage transplantation and all achieved CR.
‖Cell Kinetics of NS7CAR
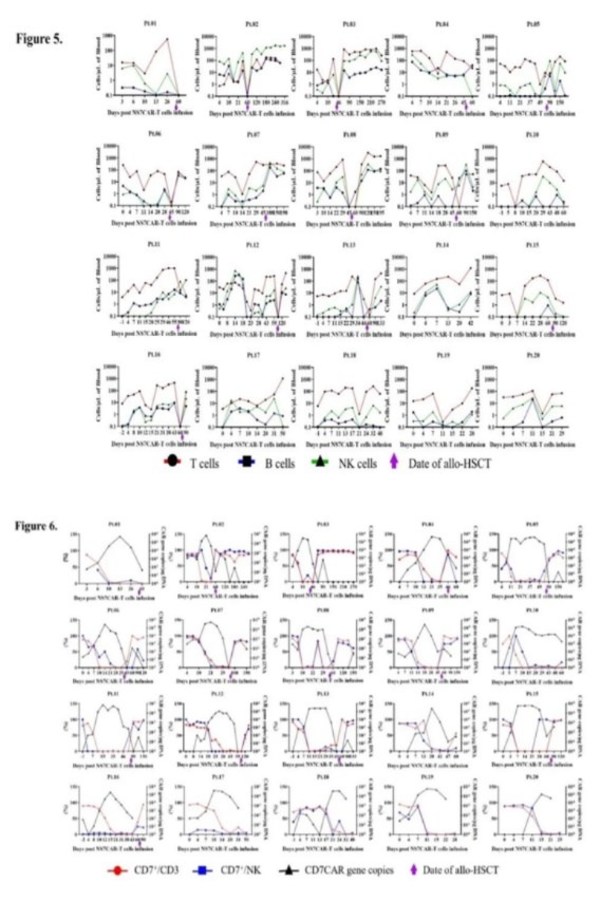
NS7CAR amplification started at a median of 4.5 days after infusion. The median peak copy number of CAR was 1.37×10.5copies/μg DNA, with a median time to peak of 19 days. At the last follow-up, the median duration of NS7CAR+DNA was 90 days; at a median time of 39.5 days post-transplant, 12 out of 14 patients still had detectable low levels of NS7CAR+DNA via qPCR. For the six patients who did not undergo bridging transplantation, CAR-T cells were still detectable at the last follow-up, with a median duration of 48.5 days. The median peak percentage of NS7CAR detected by flow cytometry was 67.76%, with the highest proportion reaching 84.71%; the median peak time was 17 days.
The most significant reduction in malignant and normal CD7+ cells in the peripheral blood of patients after NS7CAR infusion occurred at a median time of 7 days post-infusion. At the peak of CAR-T expansion, the absolute numbers of T/B/NK cells (excluding CAR+ and leukemic T cells) in each patient showed varying degrees of transient decline. NS7CAR rapidly eliminated CD7+ cells while predominantly preserving the CD7-negative cell subsets. T/B/NK cells subsequently recovered to baseline levels but, as expected, exhibited a decrease shortly after transplantation. Normal CD7+ T cells and NK cells were adequately restored post-transplantation.
‖Summary
The study reveals a method for producing targeted CD7 CAR-T cells through a "natural selection" mechanism (NS7CAR). Researchers found that although the CD7 molecule on the surface of NS7CAR-T cells could not be detected by flow cytometry, the levels of CD7 mRNA and protein continued to be expressed in NS7CAR-T cells, albeit slightly lower, but comparable to those in normal control T cells. The study suggests that the CD7 molecules of NS7CAR-T cells are likely masked by CD7CAR antigens or sequestered intracellularly, significantly reducing surface CD7 antigen on NS7CAR-T cells and avoiding extensive fratricide among CAR-T cells. It cannot be ruled out that a small number of NS7CAR-T cells might emerge from fratricide during the in vitro "natural selection" process. This contrasts NS7CAR-T with truly CD7-negative Neg7CAR-T or KO7CAR-T cells. The researchers proposed that many NS7CAR-T cells themselves are not CD7-negative but functionally CD7-negative.
Therefore, the researchers hypothesized: Since CAR signaling may require the formation of a protein complex, CAR-T cells are activated through the interaction between free CD7CAR on the surface of NS7CAR-T cells and CD7 expressed on target T cells, while the intracellular CD7-CD7CAR complex cannot activate T cells. Compared with Neg7CAR and KO7CAR cells, it remains to be determined whether the intracellular CD7CAR-CD7 interaction leads to reduced CAR signaling and decreased in vitro expansion of NS7CAR cells. Secondly, whether fratricide plays a role in the reduced expansion of NS7CAR cells needs further investigation.
In NS7CAR, there are significantly more CD8+ central memory CAR-T cells, and this CD8 bias may provide more durable disease control. Since the production of NS7CAR does not involve additional gene editing, it avoids the potential risk of off-target effects. Therefore, the biological characteristics of NS7CAR and the convenience of its production are highly advantageous for clinical application.
To date, there are only limited clinical trials and case reports on CD7-targeted CAR-T therapy for T-cell malignancies. NS7CAR can be prepared from the peripheral blood of patients or donors, with a median transfection rate greater than 95% and a cell viability rate of approximately 90%. The primary safety concern with autologous CAR-T cells prepared from patients with T-cell malignancies is malignant cell contamination in the final cell product. Based on the phenotype of circulating tumor cells in each patient, the use of CD3 or CD4/CD8 selection combined with the in vitro "natural selection" of NS7CAR and its robust anti-leukemia activity can successfully eliminate malignant cells during NS7CAR production.
In this clinical trial, nearly all patients achieved MRD-negative CR by Day 28. Most patients with extramedullary lesions, including those with central nervous system leukemia or diffuse extramedullary involvement, also reached extramedullary CR. Two patients with large mediastinal masses achieved PR and SD, respectively. For patients with large masses, a longer treatment duration and combination therapy may be required to achieve CR, as further clinical improvement was observed on Day 104 in the patient assessed as PR based on PET-CT evaluation.
Patients enrolled in this clinical trial had received extensive prior treatments. Given the high relapse rate of B-ALL patients treated with CD19 CAR-T and the fact that T-ALL/LBL is more aggressive than typical B-ALL, the study allowed for consolidative allogeneic hematopoietic stem cell transplantation (allo-HSCT) after achieving remission. A total of 10 patients who achieved complete remission (CR) in both bone marrow and extramedullary sites underwent consolidative allo-HSCT, which may limit the assessment of the durability of NS7CAR-T monotherapy. Nevertheless, with a median follow-up time exceeding 4.5 months (up to 10 months), no relapses were observed in the group that received NS7CAR reinfusion followed by allo-HSCT. Among the six CR patients who did not undergo transplantation, four remained in CR at their last follow-up (median duration 1.5 months, up to 6 months). However, loss of the CD7 target was observed in some patients who did not achieve CR or who relapsed.
The STIL-TAL1 fusion gene is associated with a higher relapse rate and poorer prognosis, occurring in up to approximately 25% of T-ALL patients. In this study, all three patients with the STIL-TAL1 fusion gene had poor prognoses, with one showing no response (NR) and two experiencing early relapse, indicating that CAR-T therapy alone may not reverse their clinical outcomes. Once these patients achieve complete remission (CR) from CAR-T therapy, transplantation should be considered early in the treatment process.
The expansion of NS7CAR-T cells peaked at a median of day 19 and persisted for up to 195 days as of the last follow-up. NS7CAR-T cells were still detectable at low levels by qPCR in 12/14 patients at a median follow-up of 1.2 months (maximum 4.9 months) post-transplant.
NS7CAR demonstrated excellent safety, with only mild CRS in most patients and no severe neurotoxicity. In this clinical study protocol, the early application of tocilizumab for intervention and management may reduce the occurrence of severe CRS. This early intervention and management may have played a role in decreasing CRS.
Two patients with a history of allogeneic hematopoietic stem cell transplantation received CAR-T cells derived from the transplant donor during infusion, one of whom developed a mild skin graft-versus-host reaction. Therefore, special attention should be paid to such patients. Among 14 patients, 7 underwent subsequent allogeneic hematopoietic stem cell transplantation, including 2 patients who received a second transplantation and developed GvHD. Although very low levels of CAR-T cells were still detectable in the 7 patients who developed GvHD after infusion, it is unlikely to be the cause of GvHD.
Summary
In this study, NS7CAR demonstrated potent antitumor effects both in vitro and in vivo. The first-in-human clinical trial of NS7CAR indicated that prevention of CD7 expression and successful production of NS7CAR-T cells could be achieved without additional gene editing. Overall, NS7CAR is safe and highly effective for treating R/R T-ALL/LBL.