Tecartus® CAR T-cell Therapy Demonstrates Strong Overall Survival Rates and Continued Durable Responses in Long-Term Follow-Up of Two Pivotal Studies Including Longest Ever Follow-Up of a CAR T-cell Therapy in Mantle Cell Lymphoma

Gilead Sciences
Antiviral Drug Developer

Kite Pharma
CAR-T Cell Immunotherapy R&D Provider
News on June 10, 2022 /BioValleyBIOON/ -- Gilead Sciences' T-cell therapy company, Kite Pharma, recently presented at the 2022 American Society of Clinical Oncology (ASCO) Annual Meeting Announced CD19CAR-TLong-term Follow-up Results of Two Pivotal Clinical Trials (ZUMA-2, ZUMA-3) for Cell Therapy Tecartus (brexucabtagene autoleucel). ZUMA-2 is a global, multicenter Phase 2 study evaluating Tecartus for the treatment of relapsed/refractory mantle cell lymphoma.Lymphoma(R/R MCL) patients; ZUMA-3 is a global, multi-center, single-arm, open-label Phase 1/2 study evaluating Tecartus for the treatment of R/R B-cell acute lymphoblastic leukemia.Leukemia(B-ALL) adult patients.
The 3-year follow-up results of the ZUMA-2 study and the 2-year follow-up results of the ZUMA-3 study were announced at the meeting. Among them,The 3-year follow-up of the ZUMA-2 study represents the longest follow-up for CAR-T cell therapy in the treatment of MCL.. In the long-term follow-up of these two key studies,Tecartus treatment demonstrates strong overall survival and sustained durable remission.
In the ZUMA-2 study,After nearly 3 years of follow-up (median follow-up time 35.6 months), the overall response rate (ORR) was 91%, and the complete response rate (CR) was 68%.(95% CI: 55.2-78.5). The median duration of response (DOR) was 28.2 months, and at the data cutoff, 37% of patients were still in response. The median overall survival (OS) among treated patients was 46.6 months. In patients achieving CR, the median OS has not yet been reached (The 30-month OS rate was 60.3%.). Late recurrence (more than 24 months after infusion) is uncommon (n=3).
In the ZUMA-3 study, longer-term follow-up results of a larger pooled analysis were reported for Phase 1 and Phase 2 patients who received the pivotal dose of Tecartus. The analysis includedMost patients are heavily pre-treated (referring to having received numerous prior treatment regimens)., with a median of 2 prior treatments, and 47% of patients having received ≥3 prior treatments. Analysis was performed on pooled data from Phase 1 and Phase 2 patients.At a median follow-up of 29.7 months, 73.1% of patients achieved complete remission (CR) or CR with incomplete hematologic recovery (CRi).The median OS for Phase 2 treated patients and the pooled Phase 1 and Phase 2 treated patients was 25.4 months. At the data cutoff, the median OS for Phase 2 patients who achieved CR had not been reached. The results of the combined analysis of Phase 2 treated patients (n=55) and Phase 1 and Phase 2 patients (n=78) were similar.
In these two studies, no new safety signals were observed during the extended follow-up period. In the ZUMA-2 study, since the initial report, 3% of treatment-emergent adverse events (AEs) have occurred. The most frequent Grade ≥3 AEs were neutropenia (1 case [1%] Grade 3; 7 cases [10%] Grade 4). Two patients experienced treatment-related Grade 3 serious adverse events.InfectionPneumonia and upper respiratory tract infections (n=1) and influenza (n=1). No new cytokine release syndrome (CRS) adverse events (AEs) occurred. In the ZUMA-3 study, since the initial analysis of Phase 2, no new occurrences of CRS, neurological events, infections, or hypogammaglobulinemia of any grade have been reported. Since the initial analysis, one new Grade 5 adverse event (graft-versus-host disease; considered unrelated to treatment) has occurred.
Michael Wang, Chief Investigator of ZUMA-2 and Professor in the Department of Lymphoma and Myeloma at the University of Texas MD Anderson Cancer Center, stated: "There remains a significant need for treatments that can offer long-term efficacy for MCL patients, as many have high-risk disease and are more prone to relapse or progression after receiving multiple therapies."The 3-year data from the ZUMA-2 study represents the longest follow-up time for CAR-T cell therapy in MCL patients to date, confirming that Tecartus treatment can induce durable long-term remission.”
ZUMA-3 investigator Dr. Bijal Shah, an oncologist at Moffitt Cancer Center in Tampa, Florida, stated: "After two years of follow-up and the expansion of the heavily pre-treated patient dataset in the ZUMA-3 study, we observed a high rate of durable responses, with most responses associated with undetectable minimal residual disease following Tecartus treatment. This represents a significant improvement over historical standards of care for adult patients with B-ALL, making these treatment outcomes particularly important."

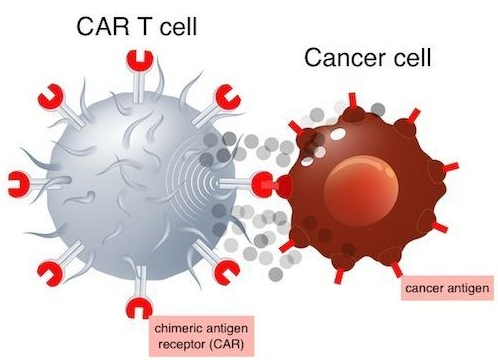
T-cell therapy is a highly promising treatment method. Tecartus is a CD19-directed autologous CAR-T cell therapy. Its principle involves genetically modifying the patient’s own T cells to express chimeric antigen receptors (CAR) that target the CD19 antigen. CD19 is an antigen protein expressed on the surface of various hematologic tumor cells, including B-cell lymphoma and leukemia cells. The modified T cells are reinfused into the patient's body, thereby recognizing and attacking tumor cells and other B cells expressing CD19.
Tecartus adopts the XLP manufacturing process, including T-cell screening and lymphocyte enrichment. For certain B-cell malignancies with evidence of circulating lymphoblasts, lymphocyte enrichment is a necessary step.Currently, Tecartus is being developed for the treatment of mantle cell lymphoma (MCL), acute lymphoblastic leukemia (ALL), chronic lymphocytic leukemia (CLL), and others.
To date, Tecartus has been approved for 2 indications: (1) for the treatment of adult patients with relapsed or refractory mantle cell lymphoma (R/R MCL) who have previously received 2 or more systemic therapies (including a BTK inhibitor); (2) for the treatment of adult patients with relapsed or refractory precursor B-cell acute lymphoblastic leukemia (B-ALL) (18 years and older). Notably,Tecartus is the first CAR-T cell therapy approved for the treatment of R/R MCL, and also the first CAR-T cell therapy approved for the treatment of adult ALL patients (≥18 years old).
Mantle Cell Lymphoma (MCL) is a rare type of non-Hodgkin lymphoma (NHL), originating from the "mantle zone" cells of the lymph nodes, primarily affecting men over the age of 60. Approximately 33,000 people worldwide are diagnosed with it each year.DiagnosisFor MCL. MCL is highly aggressive after recurrence, and many patients experience disease progression following treatment.
Acute Lymphoblastic Leukemia (ALL) is an aggressive blood cancer that can also affect the lymph nodes, spleen, liver, central nervous system, and other organs. Approximately 64,200 people worldwide are diagnosed with ALL each year, with 60% of cases occurring in individuals under the age of 20. The survival rate for adult patients with relapsed or refractory ALL remains low, with a median overall survival of less than 8 months when treated with the most commonly used therapies.Precursor B-cell ALL is the most common type, accounting for approximately 75% of ALL cases.Compared with other types of ALL, the treatment outcome of this type of ALL is usually poorer. (Bioon.com)
Source of the original text:Tecartus® Car T-cell Therapy Demonstrates Strong Overall Survival Rates and Continued Durable Responses in Long-Term Follow-Up of Two Pivotal Studies Including Longest Ever Follow-Up of a CAR T-cell Therapy in Mantle Cell Lymphoma