Predictive Biomarkers Identified for T+A Regimen in Advanced Hepatocellular Carcinoma, According to Nature Medicine Study

Genentech
Pharmaceutical R&D Manufacturer
In November 2007, the U.S. Food and Drug Administration (FDA) approved sorafenib for the treatment of unresectable hepatocellular carcinoma, completely breaking the situation where no drugs were available for advanced liver cancer.
The emergence of the "T+A regimen," which combines the PD-L1 inhibitor atezolizumab with the VEGF inhibitor bevacizumab, has shaken the position of sorafenib.
According to the Guidelines for the Diagnosis and Treatment of Primary Liver Cancer in China (2022 Edition) [1], both the T+A regimen and sorafenib are listed as first-line treatment options for advanced liver cancer. In the NCCN Guidelines for Hepatobiliary Cancers (2021 Edition) [2] in the United States, not only are the T+A regimen and sorafenib listed as first-line treatment options for advanced liver cancer, but the T+A regimen has also become the only preferred first-line treatment option.
Combination therapies such as the "T+A regimen," which represent targeted therapy plus immunotherapy, have greatly enriched our "armamentarium" against liver cancer. However, the population benefiting from these combination therapies is still limited, making the search for efficacy-related biomarkers extremely urgent.
Recently, a research team led by Yulei Wang from Genentech published a latest study in the prestigious journal *Nature Medicine* [3], providing new answers to this question.
Researchers found that, compared with sorafenib monotherapy, hepatocellular carcinoma (HCC) patients with pre-existing high immune components in tumors (CD274 molecule, T-cell effector-related markers, and CD8+ T-cell density) tend to benefit more from the T+A regimen. In contrast, HCC patients with a high regulatory T cell (Treg)/effector T cell (Teff) ratio and high expression of oncofetal genes (GPC3 and AFP) often show poor efficacy with the T+A regimen.
Moreover, compared with atezolizumab monotherapy, patients with high expression of VEGFR2, Tregs, and myeloid inflammation-related markers in tumors benefit more from the T+A regimen.
Screenshot of the first page of the paper
Before the story begins, it is necessary to review some prior context.
In June 2020, *The Lancet Oncology* reported the latest data on the treatment of patients with unresectable hepatocellular carcinoma (HCC) in cohorts A and F of the clinical study code-named GO30140 [4]. GO30140 is an international, multicenter, open-label Phase Ib clinical trial that observed the safety and clinical efficacy of the T+A regimen in various solid tumors.
The A cohort released this time enrolled 104 patients, all treated with the T+A regimen. Data shows that the objective response rate (ORR) of the T+A regimen in first-line treatment for advanced hepatocellular carcinoma is 36%. The F cohort enrolled a total of 119 patients, with 60 receiving the T+A regimen and 59 treated with atezolizumab monotherapy. Data indicates that the median progression-free survival (mPFS) for patients with advanced hepatocellular carcinoma was 5.6 months for the T+A regimen and 3.4 months for atezolizumab monotherapy (HR=0.55, 80% CI 0.40-0.74, P=0.011). In terms of safety, no new safety issues related to combination therapy were identified beyond safety events associated with atezolizumab and bevacizumab monotherapy.
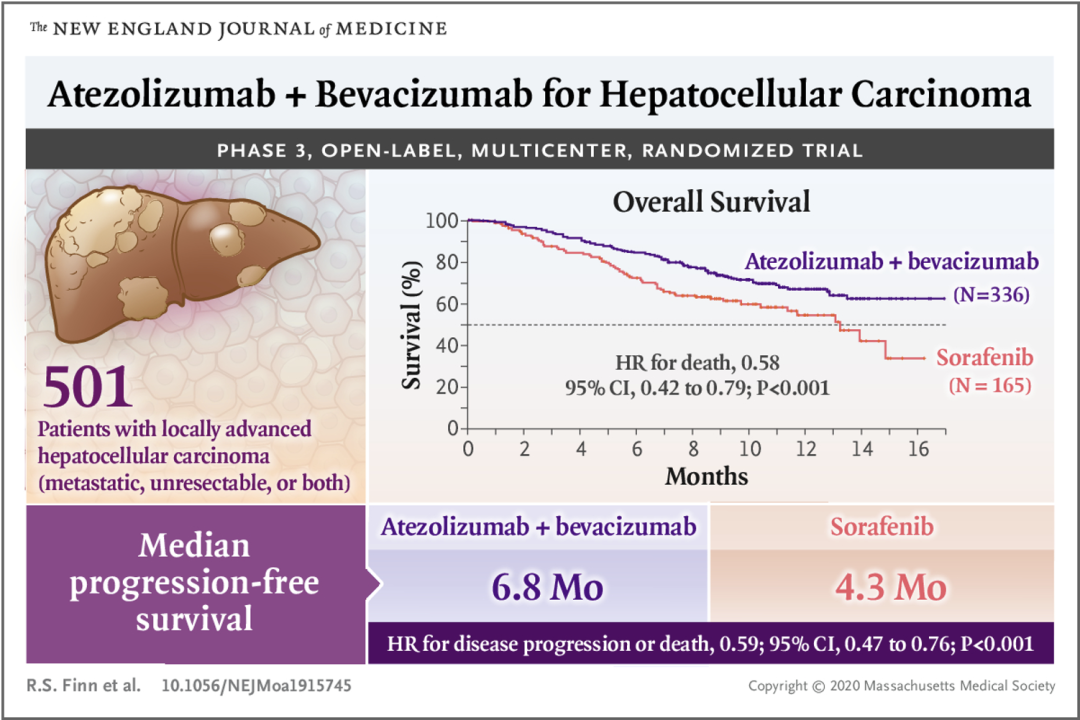
In the same year, the New England Journal of Medicine reported the results of the IMbrave150 study, which propelled the T+A regimen to become a new first-line treatment option for advanced hepatocellular carcinoma (HCC) [5]. The IMbrave150 study is an open-label, randomized, parallel-controlled international multicenter Phase III clinical trial that enrolled 501 patients with unresectable HCC who had not previously received systemic treatment. Patients were randomly assigned in a 2:1 ratio to receive either the T+A regimen or sorafenib monotherapy.
The co-primary endpoints of the study were overall survival (OS) and progression-free survival (PFS) assessed by an independent review committee according to RECIST 1.1. Data showed that the median overall survival (mOS) for the T+A regimen had not been reached, while the mOS for the sorafenib group was 13.2 months; the T+A regimen reduced the risk of OS by 42% (HR=0.58, 95% CI 0.42-0.79, P<0.001). The median PFS (mPFS) for the T+A regimen was 6.8 months, superior to 4.3 months in the sorafenib group, reducing the risk of disease progression by 41% (HR=0.59, 95% CI 0.47-0.76, P<0.001).
The important research results of IMbrave150 were reported in The New England Journal of Medicine and widely spread that year.
The latest disclosed data show that the mOS of the T+A regimen is 19.2 months, while the mOS of the sorafenib group is 13.4 months. The T+A regimen reduces the OS risk by 34% (HR=0.66, 95% CI 0.52-0.85, P<0.001). The mPFS of the T+A regimen is 6.9 months, which is superior to 4.3 months in the sorafenib group, reducing the risk of disease progression by 35% (HR=0.65, 95% CI 0.53-0.81, P<0.001) [6].
As key participants in GO30140 and IMbrave150, Yulei Wang et al. conducted pathological analyses on patients from these two studies to address the following two questions.
The first question is to find relevant markers for response or resistance to the T+A regimen.
The researchers used Cohort A of the GO30140 project (case number n=90, hereinafter the same) as the initial discovery cohort and further confirmed and explored through the IMbrave150 project cohort (n=177). If you pay attention, these patients are not all patients from the two clinical trials (ITT), but rather a subset of them, namely, the biomarker-evaluable patients (BEP) mentioned in the text. It should be noted that the baseline characteristics of BEP and ITT patients are consistent.
Researchers first conducted whole-genome differential expression gene analysis (DEG) and gene set enrichment analysis (GSEA) on cohort A patients from the GO30140 project. They found that patients responding to the T+A regimen showed significant enrichment in molecular pathways related to anti-tumor immune responses, including the IFNα/γ pathway, etc. In contrast, patients resistant to treatment exhibited significant enrichment in angiogenesis, cholesterol homeostasis, bile acid metabolism, and Notch signaling pathway genes.
Next, the researchers used xCell for immune infiltration analysis and found that CD8+ and CD4+ T cells, Tregs, B cells, and DCs were all associated with treatment response. In the IMbrave150 project cohort, the researchers also obtained similar results as before.
Thus, the researchers constructed a T+A regimen response-related gene signature (referred to as ABRS) using the 10 most significantly different genes obtained from the DEG analysis. Both ABRS and CD274, as well as the Teff gene signature (CXCL9, PRF1, and GZMB), were highly expressed in treatment-responsive patients.
In the IMbrave150 cohort, patients with high expression of these three biomarkers showed significantly improved PFS and OS with the T+A regimen compared to sorafenib monotherapy. However, for patients with low expression, there was no significant difference in PFS and OS between the two treatment regimens.
The previous analyses were all at the transcriptome level, and the researchers further validated them in situ in the tissue.
They designed two sets of multiplex immunohistochemistry to explore the relationship between the characteristics of the tumor microenvironment and clinical efficacy. The first set was used to detect the tumor-immune-stromal environment features: HepPar 1/Arginase 1, FAP, CD31, CD8, MHC-I. The second set was used to characterize the functional status of T cells: HepPar 1/Arginase 1, CD3, PD-1, PD-L1, GZMB.
Researchers performed multiplex immunohistochemical analysis on tumor samples (n=61) from cohort A of the GO30140 study. Consistent with genomic findings, patients responding to the T+A regimen tended to have higher infiltration of CD8+ T cells, CD3+ T cells, GZMB+CD3+ T cells, and MHC-I+ tumor cells.
At the same time, they also analyzed tumor samples (n=177) from the IMbrave150 project and found that patients with high CD8+ T cell density showed significantly improved PFS and OS when using the T+A regimen compared to sorafenib monotherapy. However, for patients with low CD8+ T cell density, there was no significant difference in PFS and OS between the two treatment regimens.
Thus, we have identified the characteristics of patients who benefit more from the T+A regimen compared to sorafenib monotherapy: high expression of CD274 molecules and T-cell effector-related markers, as well as high infiltration of CD8+ T cells.
Let's continue to examine the characteristics of patients resistant to the T+A regimen. Researchers analyzed the transcriptome data of tumor samples (n=177) from the IMbrave150 project using GSEA and xCell, finding that patients with a low ratio of Treg/Teff gene signatures showed significantly improved PFS and OS when treated with the T+A regimen compared to sorafenib monotherapy.
In addition, the researchers also analyzed the relationship between HCC-specific tumor markers AFP and GPC3 and the efficacy of the T+A regimen. For patients with high expression of AFP or GPC3, there was no significant difference in PFS between the two treatment regimens, but the OS of the T+A regimen still showed a trend of improvement. However, for patients with low expression of AFP or GPC3, the T+A regimen significantly improved both PFS and OS compared to sorafenib monotherapy.
Therefore, in summary, the patient characteristics for which the T+A regimen does not outperform sorafenib monotherapy are: high Treg/Teff ratio, and high expression of GPC3 and AFP.
The second question explores why the T+A regimen is more effective than atezolizumab monotherapy. From another perspective, this aims to illustrate how bevacizumab enhances the anti-tumor effects of atezolizumab.
Researchers analyzed the transcriptome data of cohort F patients from the GO30140 project (including 44 cases treated with the T+A regimen and 47 cases treated with atezolizumab monotherapy). Neither DEG nor GSEA analysis identified efficacy-related genes or pathways, but xCell analysis revealed that immune cell populations such as CD8+ T cells, Treg cells, and macrophages were associated with clinical benefits of the T+A regimen. They further found that patients with high expression of gene signatures related to Teff, Treg, and myeloid inflammation showed significantly improved PFS when treated with the T+A regimen compared to atezolizumab monotherapy.
Since bevacizumab targets the VEGF-VEGFR2 (KDR) signaling axis, researchers analyzed the relationship between these two molecules and clinical prognosis. They found that patients with high KDR expression benefited more from the T+A regimen, suggesting that anti-VEGF may enhance the efficacy of anti-PD-L1 by inhibiting tumor angiogenesis.
The researchers also analyzed the vascular density of patients in group F through CD31 staining. They found that patients with high vascular density showed significantly improved PFS when treated with the T+A regimen compared to atezolizumab monotherapy. This is consistent with the mechanism by which anti-VEGF can promote vascular normalization and inhibit tumor angiogenesis.
To validate this mechanism hypothesis, the researchers analyzed the expression levels of KDR and Treg gene signatures in 14 hepatocellular carcinoma patients before and after treatment.
They found that KDR expression decreased after treatment in both responders and non-responders to the T+A regimen. Regarding the Treg gene signature, it decreased post-treatment in 4 out of 5 responders to the T+A regimen, compared to only 2 out of 6 non-responders. The myeloid inflammation-related gene signature did not show a consistent trend before and after treatment.
To further understand the mechanism by which bevacizumab enhances the anti-tumor effects of atezolizumab, researchers utilized an anti-PD-1 treatment-resistant mouse HCC model (MYC overexpression, β-catenin activation). Similarly, they found that the T+A regimen significantly improved survival in mice compared to atezolizumab monotherapy.
Researchers further analyzed the immune composition of mice after treatment and found that compared with atezolizumab monotherapy, the T+A regimen showed a trend toward reducing the total number and proliferating Tregs infiltrating the tumor, as well as a decrease in the proportion of proliferating Tregs among total Tregs. Additionally, researchers observed a trend toward a reduction in monocyte-derived macrophages in the combination therapy group.
Combining clinical samples and mouse models, we can see the possible reasons for bevacizumab enhancing the anti-tumor effect of atezolizumab: inhibiting VEGF-mediated tumor angiogenesis, improving myeloid immunity, and suppressing Treg cell proliferation.
Overall, this study starts high——based on patient samples from two large clinical trials. The methods are diverse——including genomic and transcriptomic analysis, in-situ protein level detection, and exploration using mouse models. The significance is profound——compared to sorafenib monotherapy, hepatocellular carcinoma (HCC) patients with high levels of CD274 molecules, T-cell effector-related molecules, and CD8+ T-cell density tend to benefit more from the T+A regimen, while HCC patients with a high Treg/Teff ratio and high expression of oncofetal genes (GPC3 and AFP) often show poorer efficacy with the T+A regimen. Compared to atezolizumab monotherapy, patients with high expression of VEGFR2, Tregs, and myeloid inflammation-related markers in tumors benefit more from the T+A regimen.
Tumor treatment has entered the immunotherapy+ era. With the rise of various treatment combinations such as dual and triple therapies, clinical practice has moved ahead of basic research. The analysis and summary of clinical samples and case data will help us identify more specific and practical efficacy-related molecular markers, which in turn will drive basic research to better serve clinical needs.
References:
[1]. Guidelines for the Diagnosis and Treatment of Primary Liver Cancer (2022 Edition) [J]. Electronic Journal of Comprehensive Cancer Treatment, 2022, 8(02): 16-53.
[2].Benson AB, D'Angelica MI, Abbott DE, Anaya DA, Anders R, Are C, Bachini M, Borad M, Brown D, Burgoyne A, Chahal P, Chang DT, Cloyd J, Covey AM, Glazer ES, Goyal L, Hawkins WG, Iyer R, Jacob R, Kelley RK, Kim R, Levine M, Palta M, Park JO, Raman S, Reddy S, Sahai V, Schefter T, Singh G, Stein S, Vauthey JN, Venook AP, Yopp A, McMillian NR, Hochstetler C, Darlow SD. Hepatobiliary Cancers, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2021 May 1;19(5):541-565. doi: 10.6004/jnccn.2021.0022. PMID: 34030131.
[3].Zhu AX, Abbas AR, de Galarreta MR, Guan Y, Lu S, Koeppen H, Zhang W, Hsu CH, He AR, Ryoo BY, Yau T, Kaseb AO, Burgoyne AM, Dayyani F, Spahn J, Verret W, Finn RS, Toh HC, Lujambio A, Wang Y. Molecular correlates of clinical response and resistance to atezolizumab in combination with bevacizumab in advanced hepatocellular carcinoma. Nat Med. 2022 Jun 23. doi: 10.1038/s41591-022-01868-2. Epub ahead of print. PMID: 35739268.
[4].Lee MS, Ryoo BY, Hsu CH, Numata K, Stein S, Verret W, Hack SP, Spahn J, Liu B, Abdullah H, Wang Y, He AR, Lee KH; GO30140 investigators. Atezolizumab with or without bevacizumab in unresectable hepatocellular carcinoma (GO30140): an open-label, multicentre, phase 1b study. Lancet Oncol. 2020 Jun;21(6):808-820. doi: 10.1016/S1470-2045(20)30156-X. Erratum in: Lancet Oncol. 2020 Jul;21(7):e341. PMID: 32502443.
[5].Finn RS, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY, Kudo M, Breder V, Merle P, Kaseb AO, Li D, Verret W, Xu DZ, Hernandez S, Liu J, Huang C, Mulla S, Wang Y, Lim HY, Zhu AX, Cheng AL; IMbrave150 Investigators. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med. 2020 May 14;382(20):1894-1905. doi: 10.1056/NEJMoa1915745. PMID: 32402160.
[6].Cheng AL, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY, Lim HY, Kudo M, Breder V, Merle P, Kaseb AO, Li D, Verret W, Ma N, Nicholas A, Wang Y, Li L, Zhu AX, Finn RS. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022 Apr;76(4):862-873. doi: 10.1016/j.jhep.2021.11.030. Epub 2021 Dec 11. PMID: 34902530.