2022 ESMO: The Ups and Downs of Novel Drug Clinical Development

GSK
Pharmaceutical R&D Manufacturer
Pioneers are not always successful. When we focus on drug molecules and start to follow, we are reluctant to accept the failure of the "leading brother," but fantasize that we are the FIC (first in class) / BIC (best in class). Regarding the data and trends reflected in clinical research, we should deeply consider the underlying biological mechanisms and transform them into new product strategies.
The 2022 ESMO Congress has come to an end, with its share of surprises, disappointments, and helplessness. Although there were not many drugs targeting new targets making their debut at this conference, there are still many drug targets that have garnered attention and are making progress. Here, we have selected8 targets10 DrugsThe dynamics of clinical research allow us to experience the ups and downs in the clinical development of new drugs.

Image source: ESMO official website
WEE1: Pioneers Fall, Successors Pursue

In May, AstraZeneca reported the second/third-line treatment of metastatic triple-negative breast cancer with olaparib in combination with the ATR inhibitor ceralasertib or the WEE1 inhibitor adavosertib.Breast CancerThe Phase II clinical study (VIOLETTE study) for mTNBC did not achieve satisfactory results, and the WEE1 pipeline was removed in the Q2 report. This move has led to the complete termination of adavosertib's clinical development. However, the safety advantages of ZN-c3, developed by Zentalis, still keep the industry hopeful about the performance of the WEE1 target.
1. IMP7068
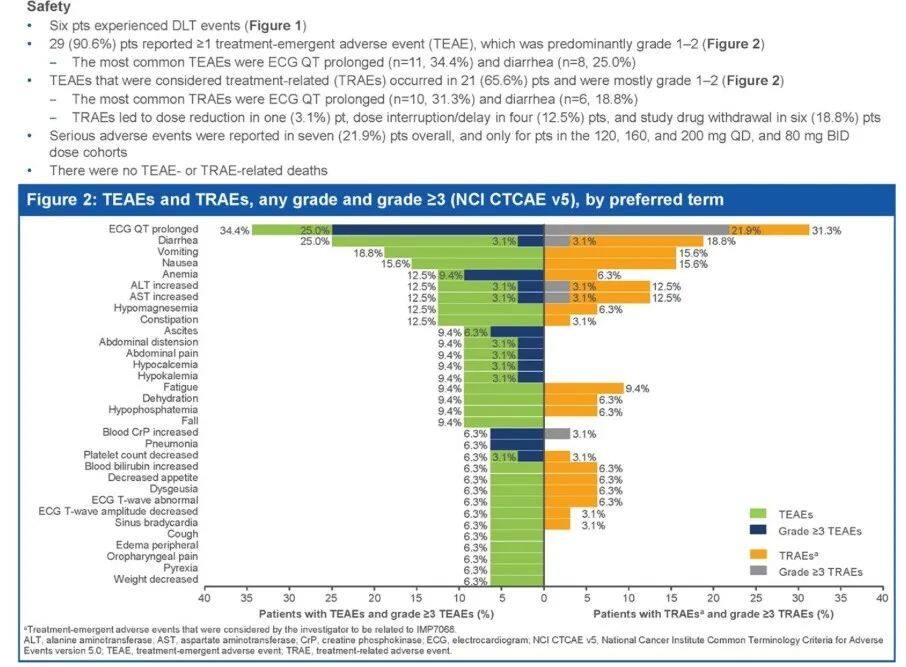
At the 2022 ESMO conference, InnoPharma announced the preliminary safety, PK, and clinical activity of the WEE1 inhibitor IMP7068. Previously,ASCOPreliminary data from a dose-escalation study involving nine patients were previously disclosed at a conference; this time, the number of patients has increased to 32. However, compared to the data available at that time, the safety data released at ESMO showed dose-limiting toxicity (DLT), and the incidence of grade 3 or higher adverse events also significantly increased.
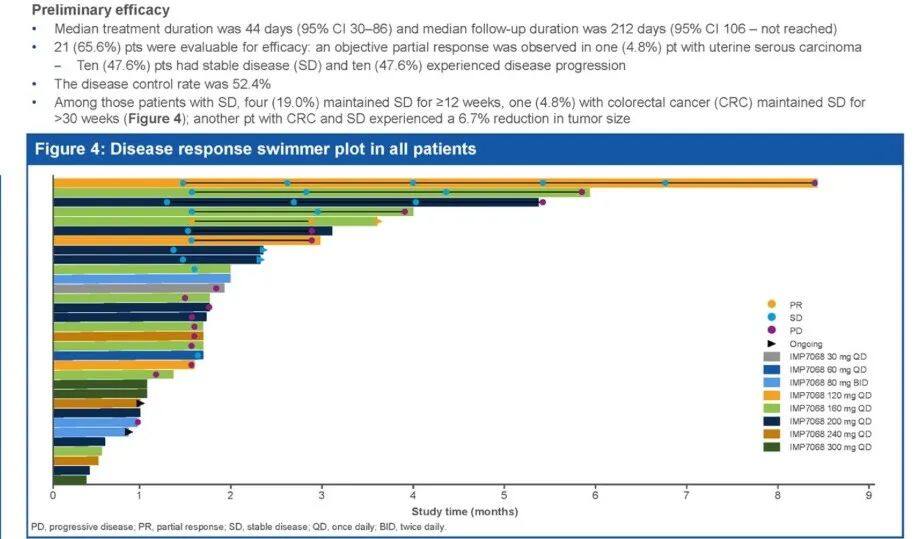
In terms of preliminary efficacy, 21 patients were included in the evaluation, with 1 showing PR (4.8%) and 10 showing SD (47.6%).
Currently, IMP7068 is still under further evaluation to determine the RP2D and optimize the dosing regimen to mitigate ECG QT prolongation adverse events.
PRMT5: The Leading Candidate Returned, Development Terminated

It seems that we have already seen the reason for the poor safety of the first generation of PRMT5 inhibitors (such as GSK3326595), which is believed to not bind to the PRMT5-MTA complex, failing to achieve selectivity for MTAP-deficient cancers. The complete inhibition of PRMT5 from start to finish leads to side effects. However, for intracellular proteins, which one exists in isolation? Protein-protein interactions cause conformational changes, rendering the experience in developing protease small molecules ineffective specifically for PRMT5.
2. PRMT5
GSK briefly mentioned the end of its collaboration with Epizyme in its 2021 annual report, returning the rights to the PRMT5 inhibitor GSK3326595 without elaborating much on the reasons for terminating the partnership. Following Epizyme's acquisition, GSK3326595 was not included in the valuation of the acquisition target.
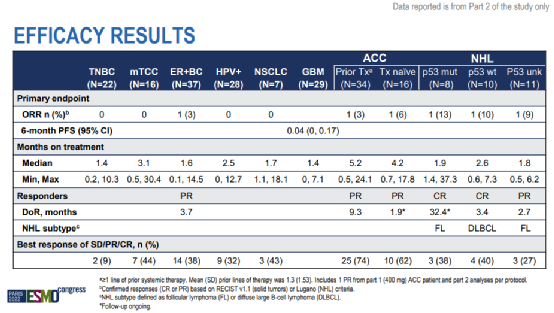
At the 2022 ESMO conference, the safety and efficacy data of GSK3326595 in advanced solid tumors were disclosed, which might have revealed the reasons for its discontinuation.
Results showed that the majority of patients had discontinued treatment at the time of data cutoff (211/218, 97%). Only three responses were observed in solid tumor patients and NHL patients respectively, with a median treatment duration of just 1.87 (0-34.8) months across cohorts. Treatment-related adverse events occurred in 95% of patients, with half of the patients (51%) experiencing grade 3/4 treatment-related adverse events. The majority of patients (70%) underwent dose interruptions, 56% required dose reductions, and 13% discontinued treatment due to adverse events.
As a small-molecule inhibitor, sufficient time must be allowed for it to take effect. However, with a median treatment duration of less than two months and nearly half of the patients experiencing grade 3/4 treatment-related adverse events, this drug was always destined to benefit only a few fortunate patients. In the real world, such luck is rare, and we can only continue to look forward to the performance of the next generation of PRMT5 inhibitors.
TIGIT: Roche Steps Back, Who Will Take the Lead?

Roche's TIGIT Antibody Tiragolumab Successively in Small CellLung Cancer/Missing the primary endpoint in two clinical trials for non-small cell lung cancer (SKYSCRAPER-02/SKYSCRAPER-01) directly hindered Roche's TIGIT therapy progress. Other TIGIT drugs still in clinical development have increased their chances of becoming the first to market.
3. ociperlimab
Currently, except for tiragolumab, domvanalimab, MK-7684A, vibostolimab, and ociperlimab have also entered Phase III clinical trials, with most of these drugs being presented at this year’s ESMO.
However, MK-7684A, tiragolumab, and domvanalimab have mostly disclosed clinical progress updates, while osericept has announced a...NSCLCDose expansion data in the field.
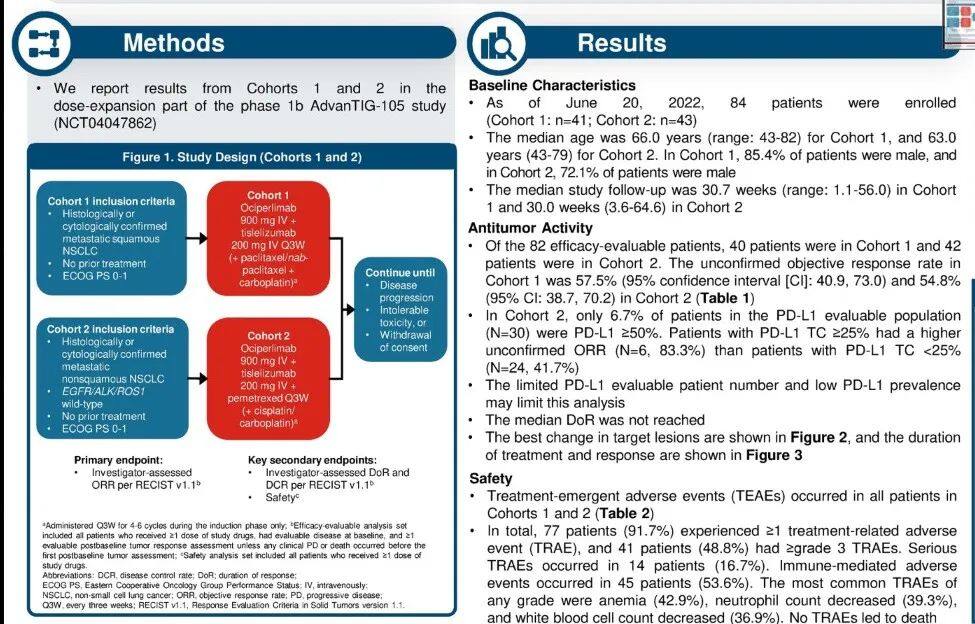
AdvanTIG-105 aims to explore the pharmacokinetic profile, safety, and anti-tumor efficacy of osiperlimab in combination with tislelizumab and chemotherapy in patients with advanced recurrent solid tumors. At the RP2D dose, 84 patients received treatment.
In terms of safety, 48.8% of patients experienced grade 3 or higher adverse events, with the incidence of serious adverse events being approximately 16.7%. In terms of efficacy, the ORR reached 57.5% in squamous NSCLC patients and 54.8% in non-squamous NSCLC patients, all of which were partial responses.
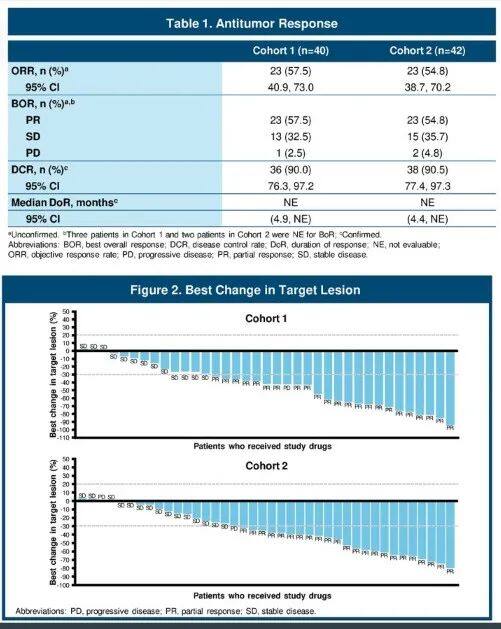
The AdvanTIG-105 study represents only the preliminary clinical data available at present. Two Phase III clinical trials (AdvanTIG-301/2) investigating ociperlimab in combination with tislelizumab and chemotherapy are currently underway, with the hope of ultimately demonstrating superior clinical outcomes compared to the combination of tislelizumab and chemotherapy (RATIONALE 304/307).
In addition to the TIGIT antibody, BeiGene also announced the results of the DisTinGuish study on the DKK1 inhibitor DKN-01 in combination with tislelizumab and chemotherapy as a first-line treatment for advanced gastric esophageal adenocarcinoma (GEA). DKN-01 is one of four clinical drugs targeting DKK1 and its development progress is relatively advanced. Preliminary results from the DisTinGuish study show that the level of DKK1 expression impacts patients' ORR performance but appears to have less effect on mPFS.
In patients with high DKK1 expression, the ORR of DKN-01 combined with tislelizumab and chemotherapy reached 90%, while in those with low expression, it was 56%. For patients with high DKK1 expression, the level of PD-L1 expression had little effect on ORR, and even better outcomes were observed in patients with low PD-L1 expression. Regarding mPFS, it was 11.3 months for patients with high DKK1 expression and 12 months for those with low expression. The mOS data are not yet mature, as only 44% of patients had died by the data cutoff date, with a median study duration of 15.7 months.
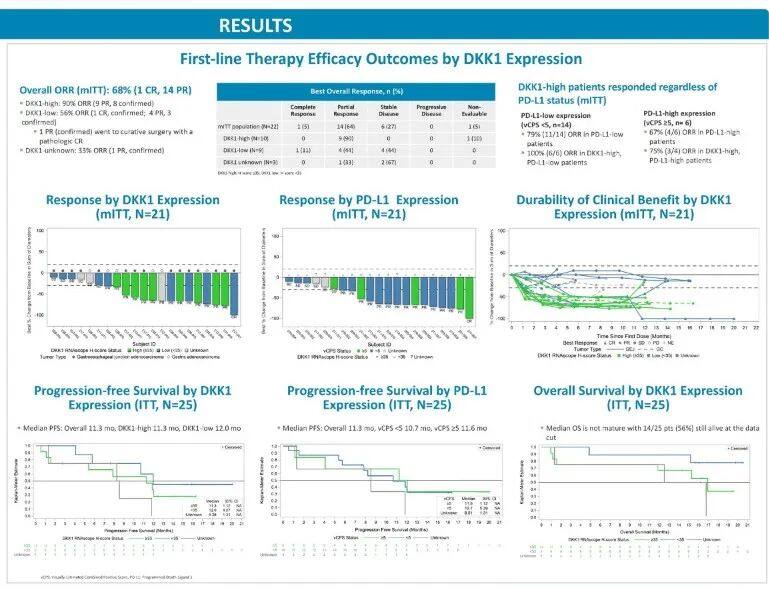
However, the number of patients included in this study was relatively small, and further evaluation of its efficacy and safety is still needed. Relevant Phase II clinical trials are currently underway. The impact of biomarkers on various efficacy endpoints clearly warrants further exploration.
CEACAM5: Sanofi's Hope in Oncology

Sanofi's exploration in the oncology field has not been smooth. The SERD oral drug amcenestrant suffered consecutive failures in Phase II and Phase III studies, leading to the termination of its development. In early June, Sanofi and Regeneron "parted ways," with the global development and commercialization rights of Libtayo returning to Regeneron. In the oncology field, the only late-stage clinical product left is the CEACAM5 antibody-drug conjugate tusamitamab ravtansine.
4. tusamitamab ravtansine
At the ESMO conference, tusamitamab ravtansine announced two clinical updates. Among them, CARMEN-GC01 is a Phase II, open-label, single-arm study evaluating tusamitamab ravtansine in combination with ramucirumab for the treatment of patients with gastric or gastroesophageal junction adenocarcinoma (GA/GEJA).
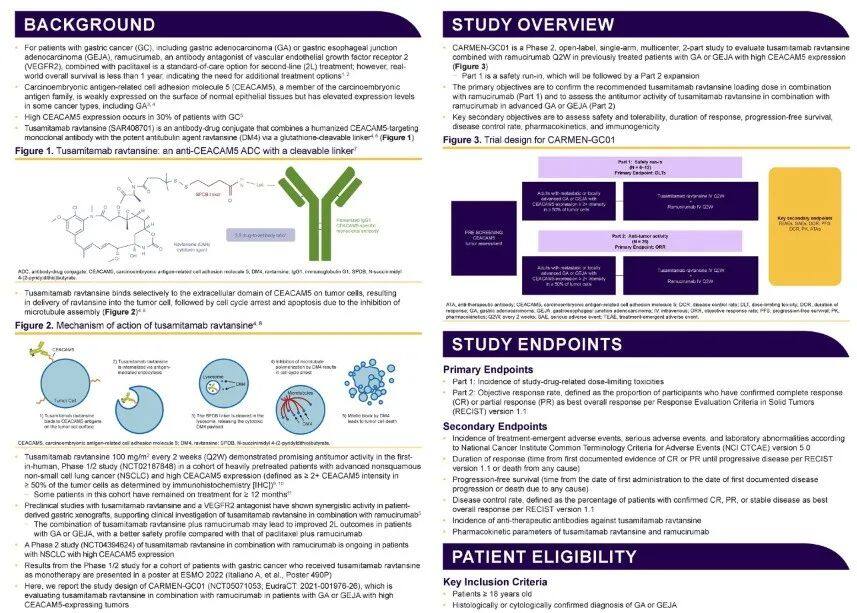
Another is tusamitamab ravtansine in the expression of carcinoembryonic antigen-related cell adhesion molecule 5 (CEACAM5)Colorectal CancerOrStomach CancerSafety and efficacy clinical data in patients. Carcinoembryonic antigen-related cell adhesion molecule 5 (CEACAM5) is a glycoprotein that is highly expressed in various tumor tissues, including those of the gastrointestinal tract, lungs, and breast, compared to its expression levels in normal epithelial tissues.
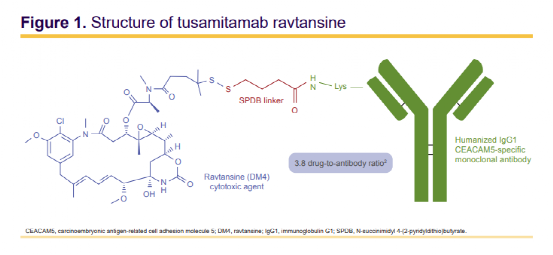
Tusamitamab ravtansine is an antibody-drug conjugate formed by linking a humanized monoclonal antibody targeting CEACAM5 with the potent anti-tubulin agent DM4 (a maytansine derivative) via a glutathione-cleavable linker, with a DAR of 3.82.
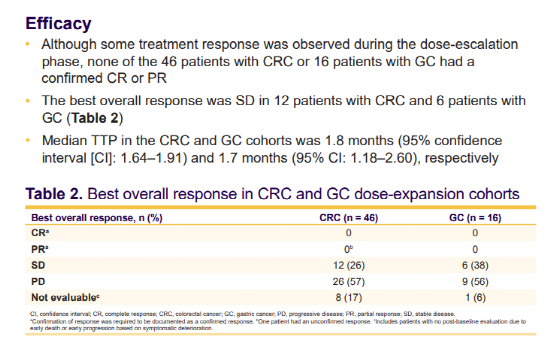
The data from this study showed that, despite observing treatment responses during the dose-escalation phase, no confirmed CR or PR was reported among 46 CRC patients and 16 GC patients. The best overall response was SD for 12 CRC patients and 6 GC patients, with a median TTP of 1.8 months for the CRC cohort and 1.7 months for the GC cohort.
Currently, the research on tusamitamab ravtansine in the NSCLC field has reached Phase III. Further development of tusamitamab ravtansine in CRC and GC patients will focus on combination therapy. Whether tusamitamab ravtansine can open another "door to oncology" for Sanofi is certainly worth attention.
ULK: Potential Pan-KRAS Target

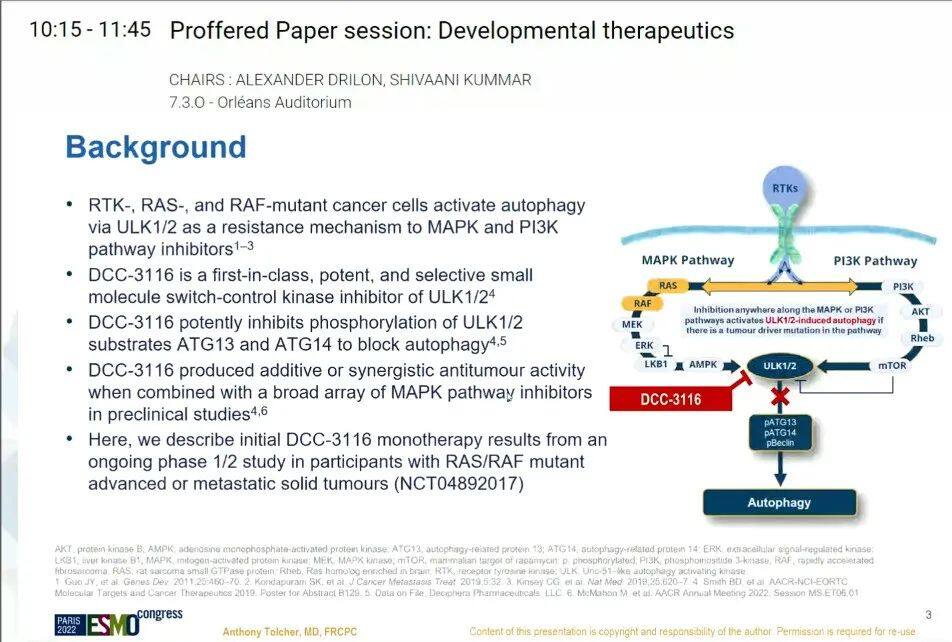
Mitogen-Activated Protein Kinase (MAPK) Pathway Inhibition Activates Unc-51 Like Autophagy Activating Kinase (ULK) 1/2 and Initiates Autophagy to Promote Survival in RAS/RAF Mutant Cancers.
5. DCC-3116
DCC-3116 is a FIC drug as a potential selective ULK1/2 inhibitor and currently the only clinical drug targeting this pathway. DCC-3116 effectively inhibits the phosphorylation of ULK1/2 substrates ATG13 and ATG14 to block autophagy, and when combined with MAPK pathway inhibitors in preclinical studies, it demonstrates enhanced or synergistic anti-tumor activity.
At this year's ESMO conference, the main announcement was the clinical data on the single-agent activity of DCC-3116. The results showed that DCC-3116 as a single agent in colorectal cancer,Pancreatic CancerPreliminary clinical signs have been observed in various tumor types carrying different KRAS subtypes mutations, with some patients achieving disease stabilization.
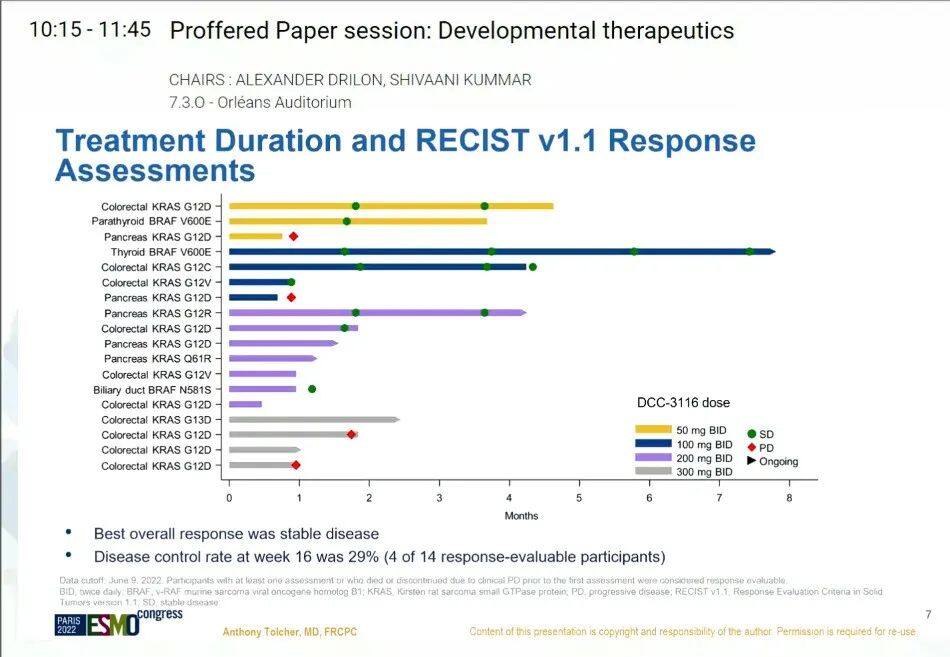
DCC-3116 was well-tolerated at doses of 50-300 mg BID, with no dose-limiting toxicity or treatment-related serious adverse events observed. Dose expansion at 100-300 mg BID is ongoing to further characterize safety, PK, and PD, and to determine the starting dose for dose escalation when DCC-3116 is combined with MEK or KRAS G12C inhibitors.
FGFR2: The Dawn of High Selectivity Has Arrived

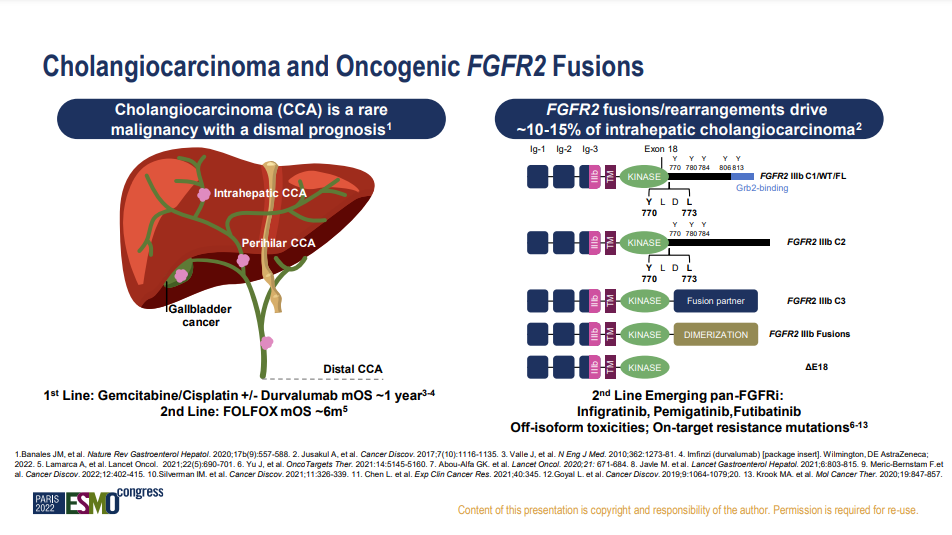
Fibroblast Growth Factor Receptors (FGFR) belong to a subfamily of the receptor tyrosine kinase superfamily, consisting of four highly conserved transmembrane receptor tyrosine kinases (FGFR1~4) and one receptor, FGFR5 (also known as FGFRL1), which can bind to FGF ligands but lacks an intracellular kinase domain. Targeting FGFR has become a promising strategy for the treatment of cholangiocarcinoma (CCA), but the lack of selective FGFR inhibitors can easily lead to adverse events such as hyperphosphatemia caused by FGFR1 inhibition.
6. RLY-4008
Cholangiocarcinoma (CCA) is the most common biliary malignancy. Based on its location, CCA can be divided into intrahepatic, perihilar, or extrahepatic CCA, with early symptoms being insidious and often presenting at an advanced stage upon diagnosis. Although FGFR inhibitors have shown significant activity, current FGFR inhibitors are only effective for 10-15% of CCA patients with FGFR2 fusions and rearrangements, but they exhibit non-selective toxicity and off-target resistance mutations.
RLY-4008 is a highly potent and selective oral small-molecule FGFR2 inhibitor currently under clinical investigation for the treatment of intrahepatic cholangiocarcinoma. Preclinical data show that RLY-4008 exhibits excellent selectivity for FGFR2.
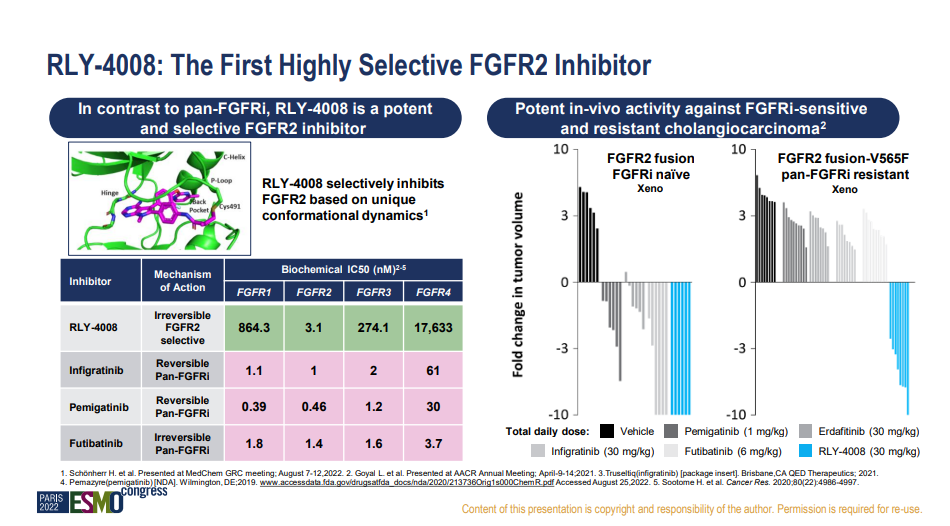
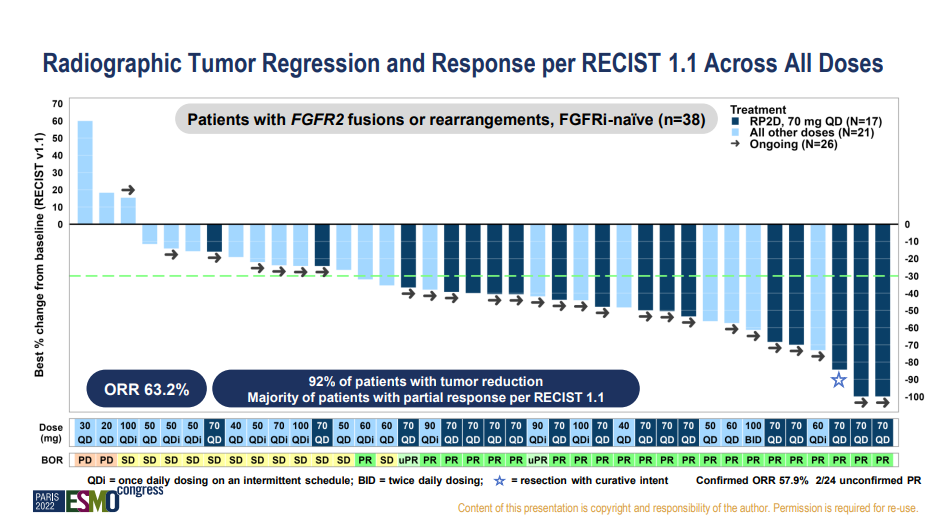
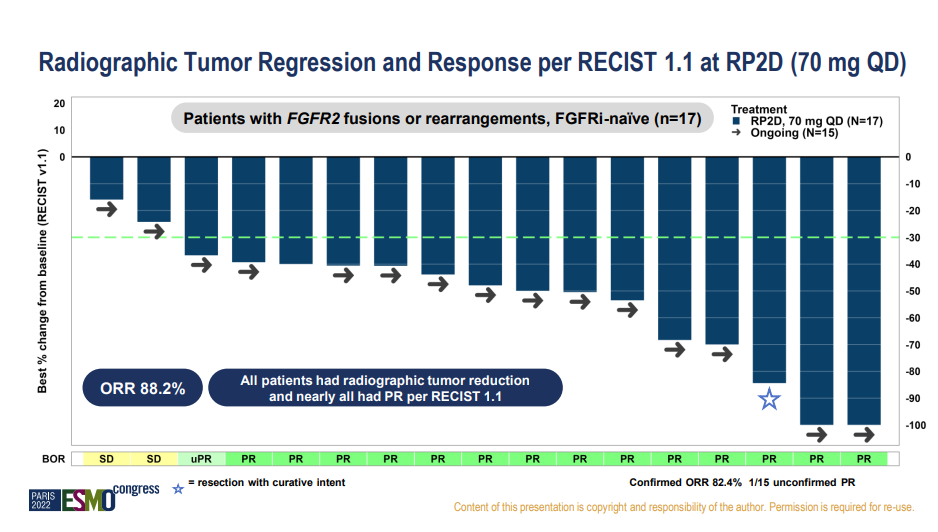
In the clinical data released at the 2022 ESMO conference, RLY-4008 achieved tumor shrinkage in 92% of FGFR inhibitor-naïve patients with FGFR2 fusions and rearrangements in cholangiocarcinoma, with an ORR reaching 63.2%. At the RP2D dose, the ORR was as high as 88.2%, significantly outperforming the efficacy of non-selective FGFR inhibitors that are already on the market or under regulatory review.
In terms of safety, RLY-4008 also demonstrated good tolerability, with no Grade 4 or 5 adverse events reported, and no occurrence of hyperphosphatemia. RLY-4008 has the potential to change the treatment paradigm for CCA. Encouraged by this data, Relay Therapeutics' stock price closed up 23% on the 8th.
Currently, there are not many highly selective FGFR2 small molecule inhibitors in clinical research. CGT0292, an FGFR2 inhibitor developed by Cogent Biosciences, has also demonstrated significant selectivity advantages in preclinical data.

SERD: The Convenience of Oral Administration

Selective Estrogen Receptor Degraders (SERDs), with the advantage of oral administration, are considered to have convenience in replacing the injectable drug fulvestrant. However, the consecutive failures of Sanofi and Roche have cast a shadow over SERDs. On the contrary, elacestrant (RAD1901) has become the first and currently the only oral SERD showing mPFS benefits superior to fulvestrant and has already submitted an application for marketing approval. The same target, the same small molecules, but different fates. Apart from drug design and clinical trial design, how many other issues need to be considered?
7. Elacestrant
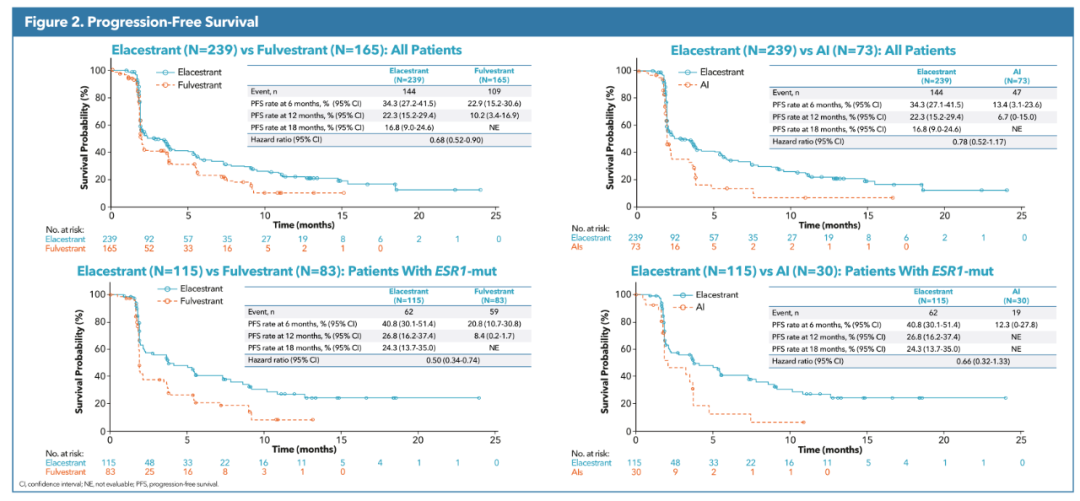
At this year's ESMO conference, Elacestrant continued to release subgroup analyses of the EMERALD study, but the eagerly awaited OS data has yet to appear.
Elacestrant has announced mPFS data, showing its advantage in the ESR1 mutation population. However, such an advantage is not absolutely guaranteed, and whether it can translate into OS benefits still requires final data to prove.
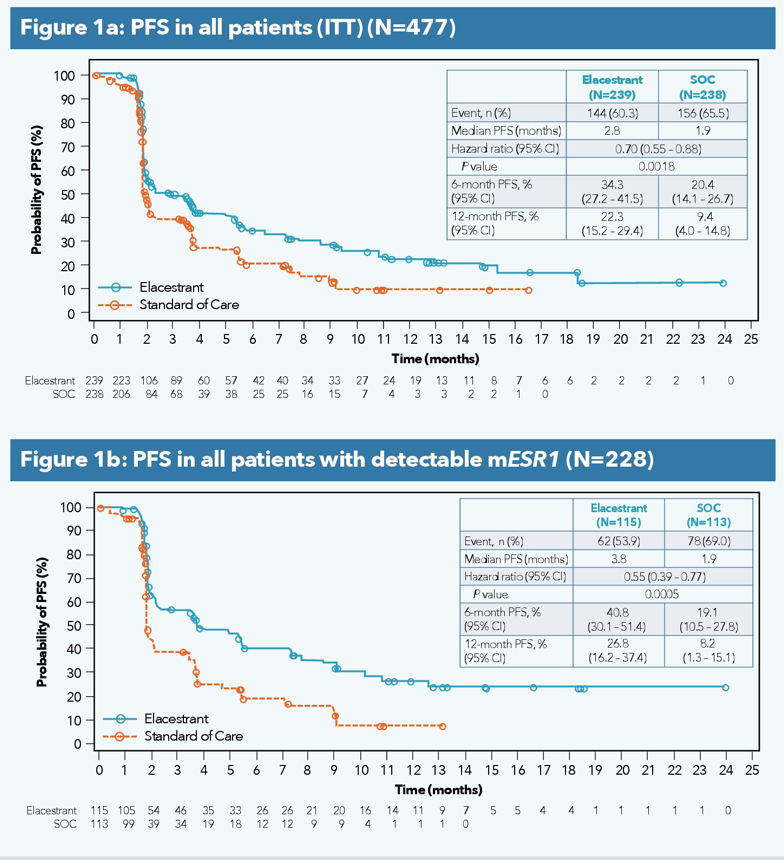
Subgroup analysis presented at the ASCO meeting showed that, in the ESR1-mutated population who did not receive chemotherapy, elacestrant demonstrated a more pronounced mPFS benefit (5.32 vs 1.91 months).
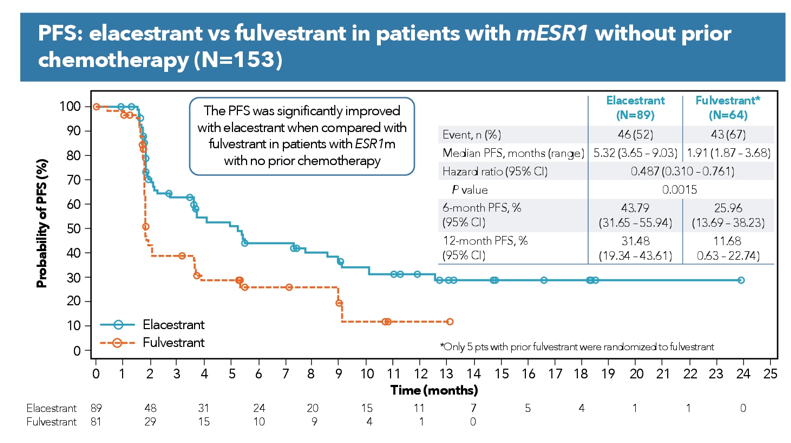
At the ESMO conference, Elacestrant continued to release subgroup analysis results of the PFS rate from the EMERALD study. In terms of data, Elacestrant still maintains its leading advantage. Notably, the trend of PFS rate change significantly slowed in the ESR mutant population after 12 months.
However, the ultimate clinical value of Elacestrant still needs to be measured by survival benefit data. Although Elacestrant offers the convenience of oral administration, its more frequent dosing regimen correspondingly increases the economic burden. Meanwhile, Elacestrant does not appear to have significant safety advantages; on the contrary, it seems to increase the probability of grade 3/4 adverse events compared to Fulvestrant.
8. giredestrant (GDC-9545)
Giredestrant announced two clinical progress data at this year's ESMO conference: the biomarker subgroup analysis of the neoadjuvant therapy coopERA study and the results data of the acelERA study, which has already been declared a failure.
In April, Roche revealed in its 2022 Q1 financial report that the Phase II acelERA trial of giredestrant (GDC-9545) for the treatment of ER+/HER2- locally advanced or metastatic breast cancer did not meet the primary endpoint of progression-free survival (PFS). Detailed data from the acelERA study were presented at the 2022 ESMO conference. The results showed that although giredestrant demonstrated a slight advantage in the 6-month PFS rate, it did not show differentiation in median PFS (mPFS). However, in the sensitivity analysis, giredestrant and fulvestrant appeared to exhibit similar trends.
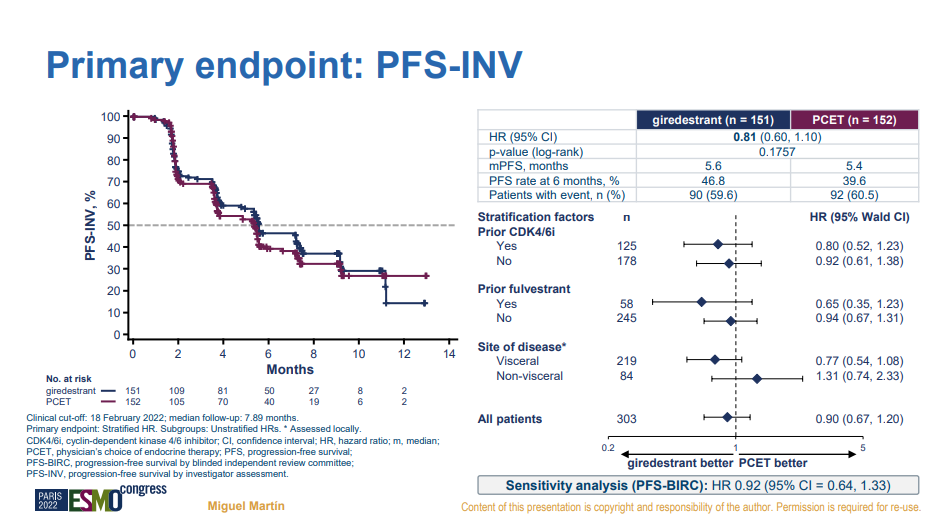
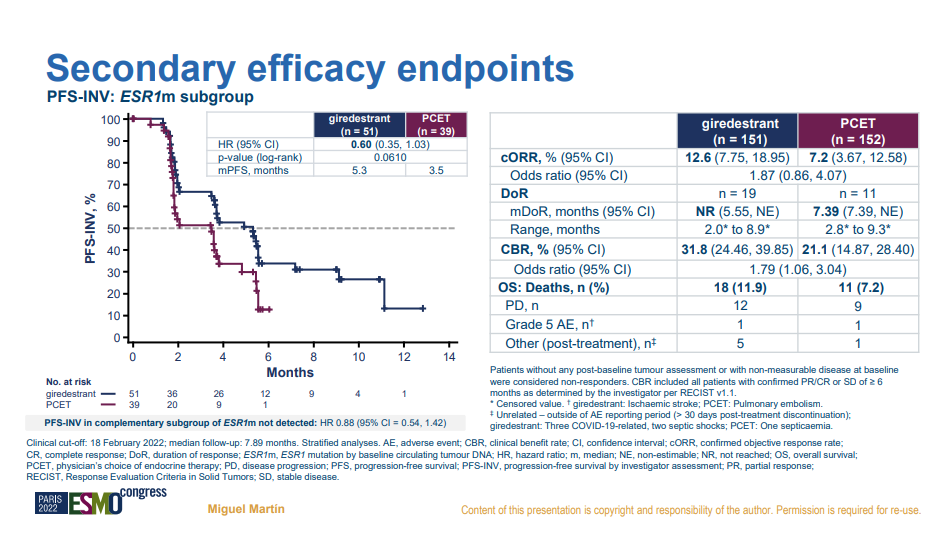
In the subgroup analysis of ESR1 mutations, giredestrant also showed a numerical advantage (mPFS: 5.3 vs 3.5 months), but unfortunately, it did not reach statistical significance in p-value.
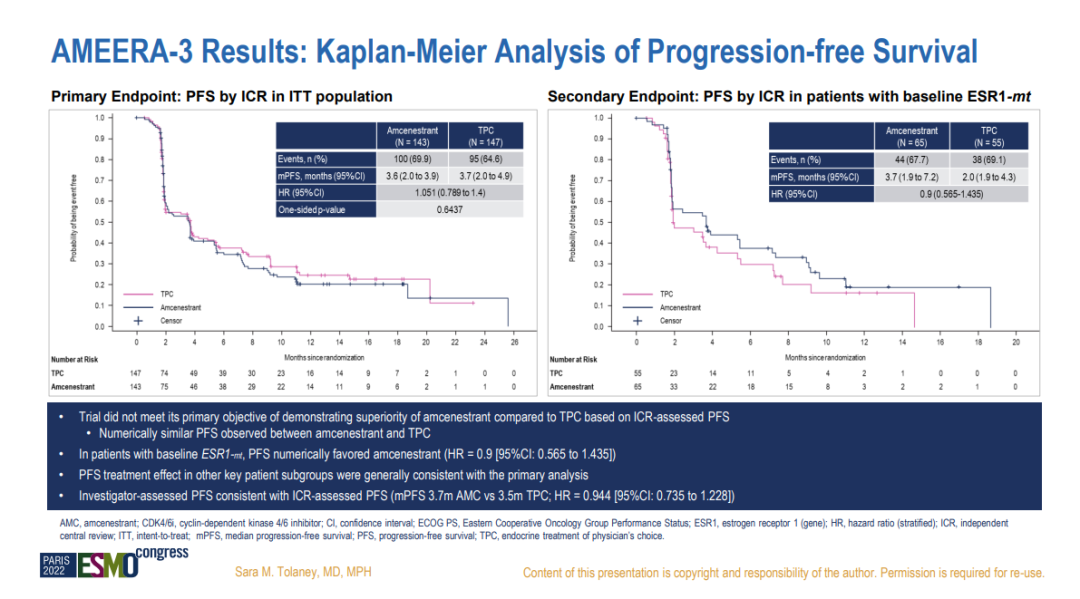
9. amcenestrant
The successive failures of the AMEERA-3 and acelERA studies also led Sanofi to terminate the clinical development of amcenestrant. Detailed results of the AMEERA-3 study were presented at this year’s ESMO conference.
Data show that amcenestrant also has the potential benefit advantage in the ESR1 mutant population, with mPFS extended by 1.7 months, but it did not reach a significant difference.
Both giredestrant and amcenestrant are SERD drugs that reported failed study outcomes at this conference. However, in terms of the absolute extension of mPFS, giredestrant did not differ much from the successful elacestrant (1.8 vs 1.9 months). Although there were differences in patient baseline characteristics, the similar absolute values yielded vastly different outcomes. Whether this is due to factors in clinical design, differences in patient baseline, or issues with the selection and allocation of control group drugs are all potentially debatable factors.
HER2: Not All ADCs Are Enhertu

August 5,FDAApproval of Enhertu (T-DXd, DS-8201) for a new indication to treat patients with unresectable or metastatic HER2-low breast cancer. This is the first approved therapy for patients with the HER2-low breast cancer subtype, redefining the HER2-negative breast cancer subtype. On the 11th, the FDA once again granted accelerated approval for Enhertu to treat adult patients with unresectable or metastatic HER2-mutation-positive non-small cell lung cancer (NSCLC) who have previously received systemic therapy, making it the first FDA-approved drug for HER2-mutation-positive non-small cell lung cancer. Enhertu continues to pave one transformative path after another.
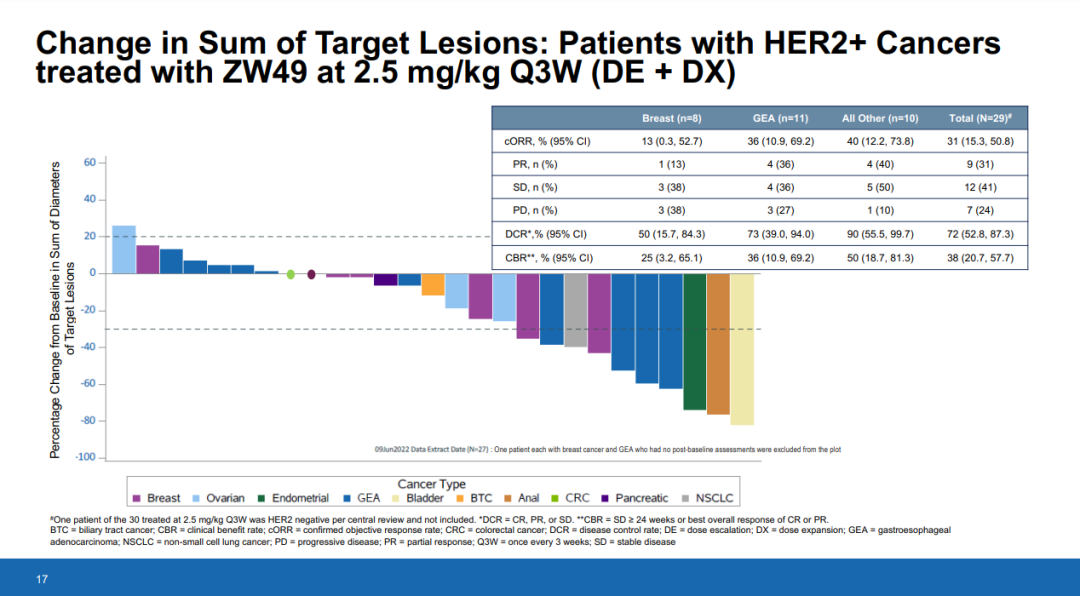
10. Zanidatamab zovodotin
Zanidatamab zovodotin (ZW49) is a HER2-targeted ADC drug developed by Zymeworks. It consists of a HER2-specific bispecific antibody with the same antibody sequence as ZW25, linked to a proprietary auristatin payload through a protease-cleavable valine-citrulline linker, with a DAR of 2.
Data show that in a Phase I study of 76 patients with HER2+ cancers, including gastric cancer (27%) and breast cancer (22%), the majority of treatment-related adverse events (TRAEs) for ZW49 were Grade 1 or 2. Among the seven patients who experienced Grade 3 or higher TRAEs, two cases were Grade 4 events, including infusion-related reactions and decreased neutrophil count; three patients discontinued treatment due to TRAEs. No treatment-related patient deaths or cases of interstitial lung disease were reported.
In terms of clinical efficacy, the ORR of ZW49 in HER2-positive breast cancer is only 13%. Such data, following Enhertu, raises doubts that ZW49 may sooner or later be terminated from development. Even though this patient had previously used Enhertu and achieved PR with ZW49, it does not mean it is worth further development for the indication.
Currently, there are more than 30 HER2 ADC drugs in global clinical trials or on the market, with 23 of them being independently developed or introduced in China. Among such a large number of HER2 ADC drugs, efficacy and safety are naturally important benchmarks for evaluating their clinical value. However, these two aspects cannot be assessed in isolation; discussing safety without considering efficacy holds no value. After Enhertu, determining how to position different HER2 ADC products in clinical practice is the most worthwhile strategy to explore.