Takeda’s Livtencity (Maribavir) Receives Positive CHMP Opinion for Refractory Post-Transplant CMV Infection in the EU

Takeda
Biopharmaceutical Manufacturer

Committee for Medicinal Products for Human Use
Committee for Medicinal Products for Human Use (CHMP)The Committee for Medicinal Products for Human Use (CHMP) is the committee within the European Medicines Agency (EMA) responsible for human medicines. The CHMP replaced the former Committee for Proprietary Medicinal Products (CPMP) in May 2004.The CHMP plays a vital role in the authorization of medicines in the European Union (EU). In the centralized procedure, the CHMP is responsible for: 1) conducting initial assessments of marketing authorization applications across the EU; assessing modifications or extensions to existing marketing authorizations (“variations”); considering recommendations from the Agency’s Pharmacovigilance Risk Assessment Committee regarding the safety of medicines on the market, and, where necessary, advising the European Commission to amend the marketing authorization of a medicinal product, or to suspend or withdraw it from the market.The CHMP also evaluates medicines authorized at the national level that are referred to the EMA, with the aim of maintaining a harmonized position throughout the EU.Furthermore, the CHMP and its working groups promote the development of medicines and pharmaceutical regulation by: providing scientific advice to companies researching and developing new medicines; developing scientific and regulatory guidelines to assist pharmaceutical companies in preparing marketing authorization applications for human medicines; and collaborating with international partners to harmonize regulatory requirements.

Image Source: Shutterstock
News / BIOON / -- Takeda Pharmaceutical Company Limited recently announced that the Committee for Medicinal Products for Human Use (CHMP) of the European Medicines Agency (EMA) has issued a positive opinion, recommending approvalAntiviral Drug Livtencity (Maribavir): For Patients Who Have Undergone HematopoieticStem CellsAdult patients undergoing hematopoietic stem cell transplantation (HSCT) or solid organ transplantation (SOT), for the treatment of post-transplant cytomegalovirus (CMV) infection and/or disease that is refractory to (with or without resistance) one or more prior therapies, including ganciclovir, valganciclovir, cidofovir, and foscarnet.
In patients undergoing SOT and HSCT, CMV infection is a common and serious clinical complication., which can lead to serious consequences, including transplant failure and even death. Data from the pivotal Phase 3 SOLSTICE (TAK-620-303, NCT02931539) trial show:In transplant recipients with refractory, with or without resistance (R/R) CMV infection/disease, maribavir is superior to IAT in clearing CMV viremia, clearing viremia while maintaining symptom control, with lower treatment-related toxicity and fewer patients discontinuing treatment due to treatment-emergent adverse events (TEAE).
The European Commission (EC) will consider the positive opinion of the CHMP and make a final review decision in the coming months.If approved, Livtencity will become the first CMV-specific UL97 protein kinase inhibitor in the European Union (EU) for the aforementioned indications. Livtencity blocks viral replication by inhibiting the activity of the CMV protein kinase pUL97.
In November 2021, Livtencity was approved by the U.S. FDA, becomingThe first drug in the United States for treating post-transplant CMV infections that are refractory to conventional antiviral therapies (with or without genotypic resistance).Livtencity is indicated for: adult and pediatric patients (aged ≥12 years, weighing ≥35 kg) who have received SOT or HSCT, for the treatment of post-transplant CMV infection that is refractory to ganciclovir, valganciclovir, foscarnet, cidofovir (with or without genotypic resistance).
Maribavir Molecular Structure (Image Source: wikimedia.org)
CMV is a β-herpesvirus that commonly infects humans; there is serological evidence of prior infection in 40%-100% of the adult population. CMV usually remains latent and asymptomatic in the body but can reactivate during periods of immunosuppression. Severe disease may occur in individuals with compromised immune systems, including patients receiving immunosuppressive therapy related to hematopoietic cell transplantation (HCT) or solid organ transplantation (SOT). Among the estimated 200,000 adult transplant cases annually,CMV is one of the most common viral infections in transplant recipients, with an estimated incidence of 16-56% in SOT recipients and 30-70% in HCT recipients.
In transplant recipients, the reactivation of CMV may lead to serious consequences, including the loss of the transplanted organ and, in extreme cases, can be fatal. Existing therapies for treating post-transplant CMV infection may exhibit severe side effects, require dose adjustments, or fail to adequately suppress viral replication. Additionally, existing treatments may necessitate or prolong hospitalization due to the administration of the therapy.
Active Pharmaceutical Ingredient of LivtencityMaribavir is an orally bioavailable anti-cytomegalovirus (CMV) compound and the first CMV antiviral drug that targets and inhibits the pUL97 protein kinase and its natural substrates.Current CMV management is associated with difficult trade-offs, including the management of toxicity and viral clearance. Livtencity has the potential to redefine the treatment approach for refractory CMV post-transplant, with or without resistance.
Maribavir belongs to a class of drugs called benzimidazole nucleosides, which can specifically inhibit the pUL97 protein kinase of CMV, potentially affecting several key processes of CMV replication, including viral DNA replication, viral gene expression, capsid formation, and the escape of mature capsids from the nucleus of infected cells.
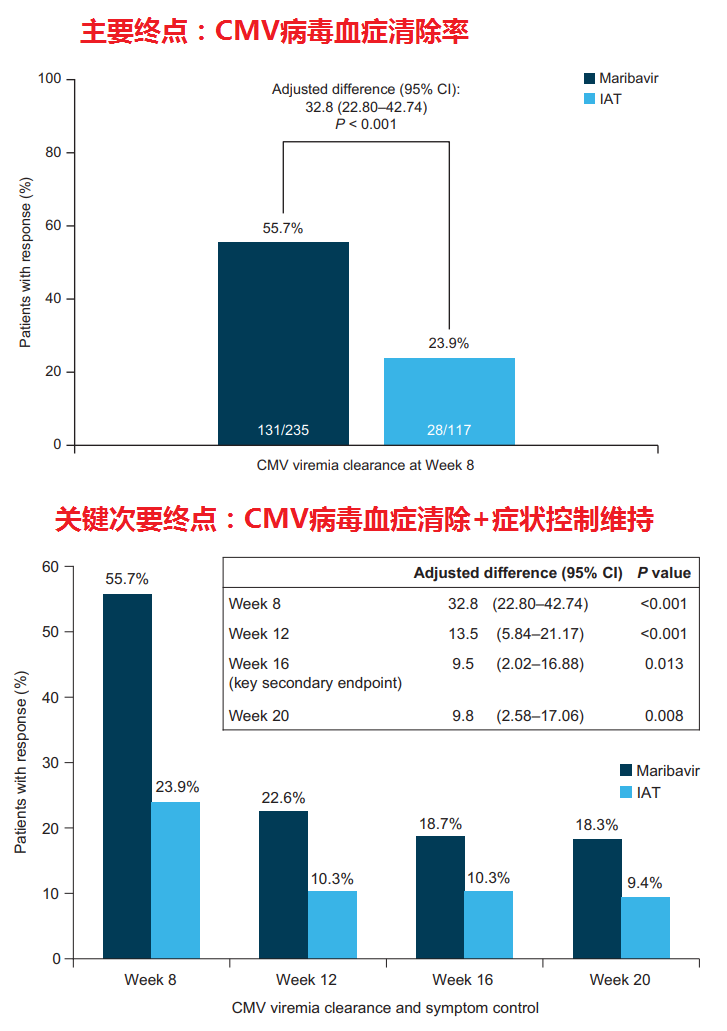
Results of the SOLSTICE Trial (Image source: PMC9464078)
SOLSTICE (TAK-620-303) is an open-label Phase 3 study conducted in transplant recipients with refractory, with or without resistant (R/R), cytomegalovirus (CMV) infection/disease. The study compared maribavir with conventional antiviral drugs (Investigator-Assigned Treatment [IAT], a combination of one or more of the following drugs: ganciclovir, valganciclovir, foscarnet, cidofovir). The primary endpoint of the study was the confirmed CMV viremia clearance rate at the end of Week 8 of treatment, and the key secondary endpoint was achieving CMV clearance and maintaining symptom control until Week 16.
The results showed,The study met the primary endpoint and key secondary endpoints: (1) At the end of Week 8 of treatment, the proportion of patients achieving confirmed CMV viremia clearance was more than double in the maribavir group compared to the IAT group (55.7% vs 23.9%; adjusted difference [95% CI]: 32.8% [22.80-42.74]; p<0.001); (2) The proportion of patients achieving CMV clearance by Week 8 with sustained symptom control through Week 16 was more than double in the maribavir group compared to the IAT group (18.7% vs 10.3%; adjusted difference [95% CI]: 9.5% [2.02-16.88]; p=0.01).
The data from the subgroup analysis shows:In transplant recipients confirmed to have genotypic drug-resistant CMV infection at baseline, the proportion of patients achieving confirmed clearance of CMV viremia at Week 8 of the study (end of the treatment period) was more than three times higher in the maribavir group compared to the IAT group (62.8% vs 20.3%; adjusted difference [95% CI]: 44.1% [31.3, 56.9]).
In the study, the incidence of treatment-emergent adverse events (TEAEs) was similar between the two groups (97.4% in the maribavir group vs 91.4% in the IAT group). Compared with foscarnet, maribavir had a lower incidence of acute kidney injury (8.5% vs 21.3%), and compared with valganciclovir/ganciclovir, it had a lower incidence of neutropenia (9.4% vs 33.9%).Compared with the IAT group (31.9%), fewer patients in the maribavir group discontinued treatment due to TEAEs (13.2%).. One patient in each group experienced a fatal treatment-related TEAE. (Bioon.com)
Source: Takeda Receives Positive CHMP Opinion for Maribavir for the Treatment of Adults with Post-transplant Cytomegalovirus (CMV) Refractory (With or Without Resistance) to Prior Therapies