How AstraZeneca Boosted Its R&D Success Rate from 4% to 19% in Five Years

AstraZeneca
Biopharmaceutical Manufacturer
AstraZeneca's R&D Director and Biopharmaceuticals R&D Head, Mene Pangalos, recently announced plans to retire in March next year.
Pangalos is responsible for all R&D activities at AstraZeneca except for oncology. In 2010, when Pangalos joined this British pharmaceutical giant, the company was facing an existential threat: declining sales, a weak pipeline, and Pfizer's attempt to acquire the company. During his tenure, AstraZeneca's revenue continued to grow, and its stock price also climbed.Increased by more than 500%.
Pangalos identified the biggest issue: AstraZeneca's research was not yielding results. AstraZeneca's success rate in Phase III clinical trials was 4%, lagging behind the industry average of 6%.He promoted the emphasis on quality over quantity,From 2012 to 2016, despite the industry average dropping toBy 4%, but this emphasis on quality has put AstraZeneca'sThe success rate has been pushed up to 19%.
AstraZeneca CEO Pascal Soriot commented on Pangalos, "He has driven the transformation of AstraZeneca's R&D."
This inevitably brings up the famous work promoted by Pangalos when he joined AstraZeneca in 2010, with results published in Nature Reviews in 2014.Drug Discovery
"If I look at the performance of this company from 2005 to 2010, it was no different from other companies, where quantity was the priority. We studied pipeline projects from 2005 to 2010 to try to identify some factors that influence R&D success rates," Pangalos said in a recent interview with foreign media. "This forms the basis of the '5R' framework:The right target, the right patient, the right tissue, the right safety, and the right commercial potential.
The sixth factor is the right culture.In our decision-making process, we have already implemented the '5R' principle quite well.These years, the cultural shift has reached its peak."Pangalos emphasized.
"The R&D productivity crisis" is a widely discussed topic in the industry, and practitioners may be familiar with AstraZeneca's "5R" framework, which might sound like a cliché. However,In China, this "R&D productivity crisis" takes on another form: target point saturation, non-differentiated competition, and ultimately, even if the product makes it to market, commercial failure.
AstraZeneca has observed in its research that this is due to the transformation of R&D organizations towards "industrialization of R&D.", The purpose of this shift is to improve efficiency while ensuring quality, but some organizations use quantity-based metrics to boost productivity. The assumption is simple: if one out of every ten candidate drugs entering clinical development makes it to market, then doubling or tripling the number of candidate drugs entering development should double or triple the number of approved drugs. However, this has not happened, so R&D costs have increased while output (measured by the number of marketed drugs) has remained unchanged.
AstraZeneca noted in the paper that this quantity-based approach not only undermines the quality and sustainability of the R&D pipeline but, more importantly, also damages the health of the R&D organization and its underlying scientific curiosity. This is because scientists and clinicians shift their focus away from higher-level goals, such as gaining a deeper understanding of disease pathophysiology and therapeutic opportunities, toward achieving quantity-driven targets.And determine the development of unprecedented backup drugs and "me-too" candidate drugsIn this environment, the "pursuit of truth" in understanding disease biology may be replaced by the "pursuit of R&D progress."
Although this is only one company's assessment based on a limited number of projects within a limited time frame, it can be said that,Everything we discussed today, including differentiated competition and clinical demand orientation, was systematically elaborated in this study, especially AstraZeneca's insight into the industry culture that emphasizes "quantity over quality."Today remains highly enlightening for our industry.
1
As part of its strategic review in 2011, AstraZeneca conducted a comprehensive review of 142 drug development projects to understand the root causes of attrition of drug candidates by examining project data and decisions.
The review covered projects across all therapeutic areas from 2005 to 2010, starting from the stage following the completion of preclinical studies through the end of Phase II clinical trials. The primary objective of the review was to understand the main reasons for project terminations and identify project characteristics associated with successful outcomes. For two reasons, the comprehensive review did not extend its scope to Phase III. First, successfully passing the proof-of-concept stage (Phase II) remains the phase with the highest attrition rate across the industry and needs improvement. Second, individual companies have too few projects in Phase III to draw valid conclusions, and this number becomes even smaller when considering products that successfully reach the market.
The review was conducted by a cross-functional group composed of scientists and clinicians from the project team, in a peer-to-peer manner. To ensure objectivity, a structured questionnaire with over 200 questions covering various aspects of the project (e.g., scientific rationale for the drug candidate, target validation, and physicochemical properties) was used during interviews with the team. In addition to the written survey, in-depth peer interviews were conducted with the project team. A team of experienced scientists and clinicians rigorously peer-reviewed the responses from both the questionnaires and interviews to ensure consistent evaluation across all projects. Furthermore, to avoid any potential bias, senior leadership involved in management decisions did not participate in the review during the assessment period.
In the analysis, the drug development process is divided into four distinct phases: Preclinical (GLP toxicity to IND), Phase I (completion of first-in-human trials, including safety, tolerability, and dose evaluation), Phase IIa (early assessment of drug activity), and Phase IIb (proof-of-concept stage, dose-response).
At each stage, projects are categorized as "active" (still in that stage), "terminated" (failed at that stage), or "successful" (transitioned from that stage to the next). Each project is analyzed separately at every stage of its development path; for example, a project that has entered Phase III trials is analyzed four times throughout its development process.
Overall, out of 142 reviewed AstraZeneca projects, 94 were terminated during the evaluation period, with 33 terminated before clinical trials and 61 during clinical trials. The remaining projects were still ongoing at the time of review.
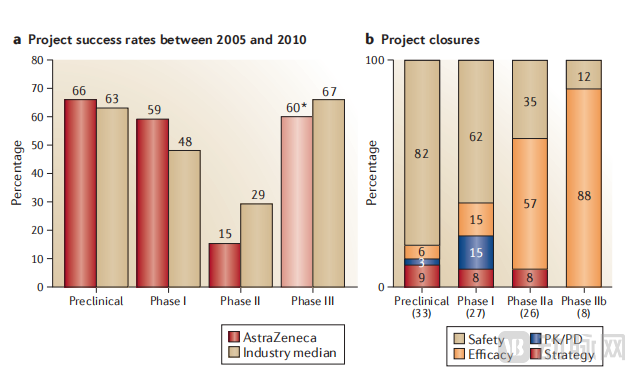
AstraZeneca compared the success rates of its projects with pharmaceutical industry benchmarks provided by the Pharmaceutical Benchmarking Forum. The success rate during the preclinical stage (defined as the percentage of projects completing this phase and moving to the next stage of development) was in line with the industry benchmark (66% VS 63%). Data showed that AstraZeneca had a higher success rate in completing Phase I compared to the industry benchmark (59% VS 48%), but a significantly lower success rate in completing Phase II (15% VS 29%). Additionally, the success rate for Phase III was also below the industry average (60% VS 67%), although the number of projects in this phase was small. As a result, AstraZeneca allowed more projects to enter the later stages of development, only for these projects to fail subsequently. Overall, during the period from 2005 to 2010, AstraZeneca’s success rate in bringing candidate drugs to market was significantly lower than the industry median (2% VS 6%).
2
Safety issues outside the acceptable range are the most important reason for project failure, accounting for more than half of all terminated projects.The majority of these failures occur before clinical trials (primarily during GLP toxicology testing), with 82% of preclinical program terminations being due to safety concerns (note that this is the percentage of program terminations, not the percentage of all programs; two-thirds of programs successfully complete the preclinical phase and enter the clinical phase).
In Phase I clinical trials, safety issues are also a primary cause of failure, with 62% of projects being terminated at this stage due to safety concerns. Safety issues remain a significant reason for project termination in subsequent development phases: among all terminated projects, 35% were halted in Phase IIa due to safety problems, and 12% were terminated in Phase IIb. Overall, 30% of projects were terminated in Phase II due to safety issues, a figure significantly higher than the reported overall industry levels (the proportion of project failures between 2008 and 2010 was 19%, and between 2011 and 2012 it was 22%). Additionally, safety issues indirectly led to project terminations as they restricted the testing dose of compounds in humans, thereby impeding adequate drug exposure and target engagement.
Most preclinical projects terminated due to safety concerns can be attributed to toxicity in specific organs. Cardiovascular toxicity is the most common cause of such terminations (17%), followed by hepatotoxicity (14%), nephrotoxicity (8%), and central nervous system (CNS) toxicity (7%). Overall, the reasons for safety failures are consistent with observations in other industries.
During preclinical trials, 75% of projects terminated due to safety concerns were related to compounds (i.e., due to the "off-target" or other characteristics of the compound), rather than the primary pharmacological effects of the target. In contrast, during the clinical stage, the proportion of safety issues related to the target increased significantly, accounting for nearly half of the project terminations due to safety concerns. Such failures are often due to an excessive gap between the predicted effective dose and safety outcomes, meaning that unacceptable safety risks would need to be assumed in order to achieve the desired target effect or patient benefit.
Moreover, studies have found that programs with safety signals in the preclinical stage are often terminated due to clinical safety issues, whereas programs with few safety signals in the preclinical stage are rarely terminated for this reason. However, it should be noted that the absence of preclinical safety signals is not sufficient to predict the success or failure of a program in later-stage development.
Overall,The analysis shows that the team needs to focus on safety signals in the preclinical stage, which is an intuitive but crucial task., while also emphasizing that, as the project progresses, safety issues will increase, potentially causing delays. The analysis further indicates,Some molecular research progress could have been terminated earlier by adopting stricter standards.
The second highest reason for project termination is the lack of efficacy in the selected disease indications.In all failed projects, more than half of Phase IIa project failures and 88% of Phase IIb project failures were due to lack of efficacy.Overall, 65% of Phase II clinical trials fail due to efficacy issues: this percentage is slightly higher than the industry-wide data (51% of projects failed between 2008 and 2010, and 59% between 2011 and 2012).
AstraZeneca conducted an investigation into the team to understand the reasons why the project failed to achieve clinical efficacy. The reasons were complex, and teams typically reported multiple contributing factors. The "most definitive" cause of failure was when a project could clearly demonstrate that pharmacological engagement with the proposed mechanism of action did not result in clinical efficacy for the patient population being tested. In these cases, 40% of project responses indicated that teams lacked evidence of a clear link between the target and the disease or lacked a well-validated animal model for the disease. Projects in this category were considered to have poor understanding of the role of the target in the underlying disease pathophysiology; however, they were also considered to be..."Beneficial" Failure,Because the hypothesis was tested and proven to be incorrect.
By contrast, 29% of project responses indicated that the properties of the compound either limited the dosage or made it impossible to determine the exposure of the compound in the relevant target tissue. For example, AZD3778 is a novel chemokine receptor antagonist developed for the treatment of asthma, but its pharmacokinetic properties were suboptimal, with a high protein binding rate and a much shorter half-life in humans than expected. Additionally, safety concerns associated with this compound restricted the dosing levels in humans. AZD3778 failed to demonstrate efficacy in clinical proof-of-concept studies, and due to the characteristics of the compound, it was impossible to confirm whether sufficient receptor exposure had been achieved. As a result, the research team made no progress in validating the effectiveness or ineffectiveness of the method or target. Among the 21% of projects classified as having failed due to lack of efficacy in Phase II clinical trials (especially in the field of neuroscience), target engagement or pharmacodynamic activity could not be determined. In all these cases, the absence of evidence regarding compound exposure and/or target tissue pharmacodynamic engagement left it unclear whether the mechanistic hypothesis had been adequately tested.These projects are classified as "non-beneficial" failures., because they failed to validate or refute the target hypothesis, the research team's understanding of their target hypothesis did not improve.
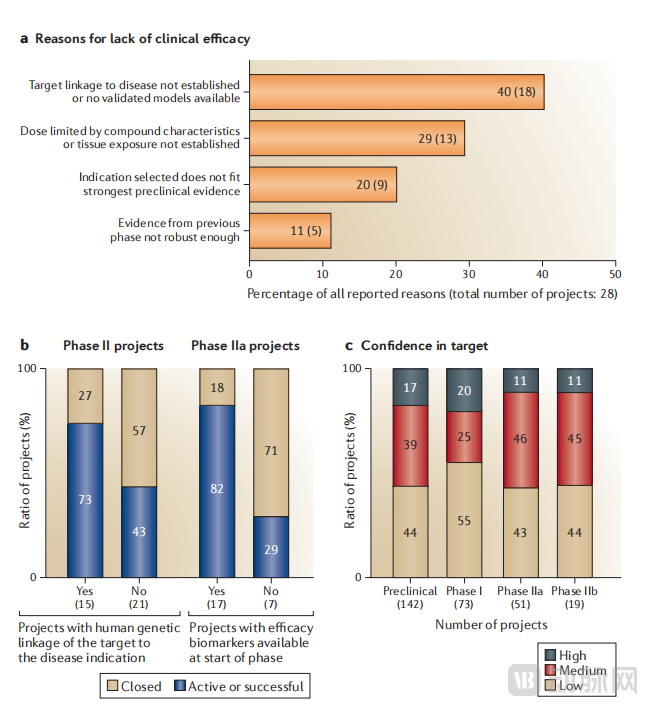
For projects that are more confident in target validation, the genetic link between the target and disease, or the understanding of the target's role in disease pathogenesis, the likelihood of failure due to lack of efficacy is lower. 73% of projects with some genetic linkage data between target and disease are active or successful in Phase II, compared to only 43% for projects without such data. Patient selection is also a factor influencing project success; high confidence in patient selection is positively correlated with active projects in Phase IIb, while low confidence in patient selection is negatively correlated with projects terminated at the same stage due to lack of clinical efficacy.
Surprisingly,Some projects (9 out of 28) indicated that, based on the scientific understanding of the disease at the time, their development plans did not target the optimal patient population.To better understand this, we examined how teams' confidence in their targets for disease indications and patient populations changes based on scientific evidence, comparing it with their confidence in perceived commercial value. In the early stages of development, project teams show greater confidence in identifying the most appropriate indications and patient populations for the research target, while confidence in commercial value remains low. Conversely, in later stages, project teams exhibit high commercial confidence but low confidence in whether the project aligns with scientifically-supported optimal indications and patient groups. This suggests that, aside from researching the most suitable patient populations based on the prevailing scientific understanding of diseases at the time, some teams are also driven by commercial value.
One surprising factor that led to the project's failure was moving the project to the next phase without sufficient reliable data.For example, 18% of the projects that failed in Phase II (5 out of 28 projects) were determined to have advanced to this stage without sufficient clinical evidence due to a lack of clinical efficacy, indicating inadequate project management. One potential reason for this situation, as mentioned earlier, could be the use of quantity-based metrics, which encourage project teams and leadership groups to push projects into the next phase in order to meet annual targets.
Only 5% of projects fail due to candidate molecules lacking the necessary drug properties (e.g., properties related to drug metabolism, pharmacokinetics, bioavailability, etc.). This is consistent with previous analysis results, indicating a reduction in failures caused by such compound-related reasons over the past two decades.
The remaining failed projects were categorized as "strategic" terminations, which were halted due to non-technical or non-scientific reasons. For instance, AstraZeneca exited the osteoarthritis research and development area during the study period, leading to the termination of multiple projects in this indication (primarily before entering GLP toxicology testing). Strategic terminations accounted for 7% of all project closures (7 projects), with 4 clinical projects terminated for strategic reasons during the evaluation period. This figure is significantly lower than the industry-wide published rates (between 2008 and 2010, the Phase II termination rate was 29%; between 2011 and 2012, it was 16%), partly because we made efforts in our analysis to uncover the root causes of "strategic" terminations and often reclassified them as "safety" or "efficacy" failures. As a result, AstraZeneca's failure rates in these two categories are notably higher than the industry benchmarks. However, it should be noted that repeated strategic shifts in disease focus can also lead to increased staff turnover and reduced productivity.
In summary, these data indicate that,At every stage of early development, scientists and clinicians must understand and be confident in disease biology, the relationship between targets and disease indications, and the mechanism of action of potential drugs within the appropriate patient context.
3
According to the analysis data, AstraZeneca identified five key factors that are crucial to the success or failure of a project. These factors include: the right target, the right tissue, the right safety, the right patient, and the right commercial potential, and these five categories are referred to as the 5 "R"s.
The Right Target
This highlights the importance of solid biological and disease knowledge. Lack of efficacy is the most significant reason for the failure of clinical trial programs. Clearly, selecting a biological target for a drug discovery program is one of the most critical decisions a team must make. If a team chooses the wrong target for a disease of interest, even the safest and most effective molecule will fail. Given the importance of target selection, one would expect that confidence in the target will increase as the program progresses through the pipeline stages, driven by a range of evidence. This may include direct evidence linking the target to human disease, genetic evidence from animal models, an understanding of the biological basis of the target and/or disease etiology, confidence in preclinical and clinical data generated using animal models, data generated using tool compounds in preclinical or clinical settings, and validated efficacy biomarkers.
In our analysis,A high level of confidence in the biological role of the target in human disease is a predictor of project success.For example, projects that obtain human genetic data linking targets to diseases before candidate drug nomination are more commonly active in Phase II (73% of projects with evidence of a genetic link between the target and the disease remain active or successfully completed in Phase II), whereas projects lacking such data are more frequently terminated (57% of projects failing due to efficacy lack any genetic validation evidence). A similar association exists regarding the availability of biomarkers for drug efficacy; 82% of projects with biomarkers indicating drug efficacy are active or successful in Phase IIa, compared to less than 30% for projects without such biomarkers.
In addition to rigorous human validation, our confidence in the "right target" is also based on a solid evidence foundation established in preclinical studies, particularly on the level of confidence in whether these research data can be successfully translated into human diseases.
In summary, understanding the biological and clinical evidence supporting target selection is crucial, as it provides a basis for guiding further research to strengthen or refute scientific hypotheses. A surprising finding in our analysis is that,For most projects, the confidence in the biological role of the target does not increase from the selection of preclinical candidate drugs to the progress of Phase II. In fact, as previously mentioned, despite the limited understanding of target biology, some projects still continue to advance.
Correct Tissue
Prove the exposure and pharmacological activity of candidate drugs in target organs. In addition to selecting the "right target," if it is possible to demonstrate the exposure and sufficient pharmacological activity of candidate drugs in target organs by establishing appropriate pharmacokinetic/pharmacodynamic (PK/PD) models in preclinical and clinical models, the probability of success will increase. In AstraZeneca's analysis, this is referred to as the "right tissue."Including pharmacokinetic properties, target engagement, and pharmacological activity, as well as an appropriate understanding of pharmacokinetics/pharmacodynamics (PK/PD), integrating these characteristics with the target organ.
AstraZeneca's analysis shows that only a few projects directly failed due to pharmacokinetics/pharmacodynamics (PK/PD) (i.e., the candidate drug did not have the required pharmacological properties). However, project questionnaires indicate,Not yet10% of the projectsHigh confidence in the drug's favorable characteristics (e.g., bioavailability, pharmacokinetics/pharmacodynamics (PK/PD), formulation, etc.) and robust pharmacological endpoints (e.g., target occupancy and evidence of pharmacological modulation).
Another analysis of the factors behind the successful development of Pfizer's drug candidates (during 2005-2009) confirmed the importance of the "right organization" concept. The analysis showed that the drug candidates most likely to test mechanisms of action and have a higher probability of surviving Phase II trials were those that comprehensively understood three key principles: drug exposure at the site of action, binding of the drug to the pharmacological target, and expression of pharmacological activity at the site of action. These principles are referred to as the "three pillars of survival."
Correct Safety
In AstraZeneca's analysis, safety issues are the most important reason for project termination. Therefore, establishing confidence in the "right safety" profile for a specific molecule is key to improving overall success rates. However, this is not a small issue, as it depends on various factors such as disease indications and unmet clinical needs. There is no such thing as "absolute drug safety"; a safety profile considered acceptable for one indication may be unacceptable for another.
Safety assessments need to address both hypothesis-driven components (e.g., predicted or potential risks associated with modulatory targets) and non-hypothesis-driven components (e.g., observed toxicological signals or adverse events caused by compounds). The latter can only be determined after the candidate drug or lead series enters extensive preclinical or clinical trials; moreover, these components may only emerge during later stages of development or post-marketing. Given that not all safety signals can be predicted, it is unsurprising that safety concerns have become a primary cause for project termination between preclinical and clinical phases. However, the situation where more than half of projects fail due to safety issues seems unsustainable.
Analysis of safety failures shows that the causes can be divided into two main categories: one is the failure to detect safety signals, and the other is the failure to appropriately assess the risks associated with safety signals. The failure of preclinical screening to detect safety signals accounts for about 40% of safety failures. These failures highlight the limitations of preclinical safety screening and the necessity to continue developing new testing methods to identify safety risks.
The second type of failure is more complex. Projects that fail in clinical development often lack confidence in preclinical safety, and the reasons for failure are usually directly related to preclinical safety observations. There are three main reasons for this type of failure.FirstOne reason is that the predicted exposure between safety and the effective dose was overestimated, which could not be translated into an increase in human dosage.SecondOne reason is that safety signals are unclear or difficult to translate from preclinical data to patients. For example, the cannabinoid receptor (CB1) antagonist program was terminated due to the withdrawal of rimonabant — an effect that could not have been predicted in preclinical models.ThirdOne reason is that the team observed and took into account the safety signals, but the project continued because there was a rationale to believe that these signals were acceptable and manageable within the indication. In this case, 11 out of 14 projects with preclinical safety signals were later terminated in the clinic due to safety issues, indicating that the team was overly optimistic and did not give sufficient weight to the preclinical signals.
AstraZeneca also observed "disease area bias" among the reasons for safety-related terminations. For example, the study found that 24% of cardiovascular projects terminated for safety reasons were due to cardiovascular safety concerns, 24% of central nervous system projects terminated for safety reasons were due to central nervous system risks, and 31% of respiratory projects were terminated due to pulmonary safety issues. This reflects, to a certain extent, the relative distribution of targets across different disease areas, while also highlighting the challenges in predicting the risk-benefit profiles of targets. It underscores the need and opportunity to tailor safety assessment protocols according to different therapeutic areas.
The industry is still a long way from being able to predict the full safety profile of a molecule before clinical trials; therefore, it is crucial to at least have strong predictions of effective exposure, which can then be explored in clinical trials relative to the safety exposure range. Finally,It is important to continue developing biomarkers that predict safety, providing early insights into potential risks.
The Right Patient
That is, testing drugs in the right patient population. In AstraZeneca's analysis,For those projects that failed in Phase II clinical trials, there is often a lack of confidence in whether they were tested in the right patient population; whereas projects with clear patient stratification plans are more likely to succeed.AstraZeneca believes that confidence in identifying and studying the "right patient" population is another key success factor, which not only affects the probability of successfully transitioning to later-stage trials but, more importantly, influences the ability to demonstrate clinical benefit.
Ideally, patients can be selected through predictive biomarkers throughout the entire clinical development process. This requires a thorough understanding of the target’s biological characteristics, as is the case with the PARP (poly ADP-ribose polymerase) inhibitor olaparib, which targets tumor cells with DNA repair defects, such as those involving the BRCA1 and BRCA2 genes. Preclinical trials demonstrated that cell lines with BRCA1 or BRCA2 deficiencies are highly sensitive to PARP inhibition. Olaparib showed encouraging results in a Phase I trial, where patients were enriched based on germline mutations in BRCA1 and/or BRCA2. However, in the Phase II study of serous ovarian cancer, patients were not selected based on BRCA1 or BRCA2 mutations (as it was initially considered too narrow a patient population), and the results were disappointing.
For those cases where the understanding of target biology is not yet deep enough to identify candidate biomarkers based on the drug’s mechanism of action, an alternative approach is to select patients based on known disease stratification markers. In all these examples, the development plan benefits (or could have benefited) from identifying appropriate clinical biomarkers to select the "right patients" during clinical development. To succeed, teams should plan and implement patient selection strategies early on, which should become an integral part of the development program.
Correct Commercial Potential
That is to ensure that scientifically feasible projects also have commercial potential and industry competitiveness. The last theme identified by AstraZeneca in the analysis is the understanding of a project's commercial potential and how to use this understanding to guide the development of the project. The term "correct commercial potential" is used to describe the confidence that a project will ultimately deliver a product with clinical differentiation and commercial viability.
AstraZeneca's analysis found that for many projects in the early portfolio, there was a lack of confidence in the dimension of "right commercial potential," either because these projects were not competitive relative to other drugs under development, or because they lacked clear differentiation in terms of unmet clinical needs.In these cases, the program is driven by a "quantity-based" culture.
Interestingly, for projects in the preclinical and Phase I stages, the research team has high confidence in finding the right target in the right patient population but very low confidence in commercial potential. In contrast, as projects move into Phase II, the team's confidence in finding the right target in the right patient population significantly decreases, while their confidence in commercial potential noticeably increases. The main reason is that these projects are pushed toward indications considered to have higher commercial potential, but these indications have weak scientific and medical foundations. Three-quarters of these projects fail in the later stages of development due to efficacy issues.
Ultimately, "the right business potential" emphasizes the necessity of providing differentiated drugs.It covers many important factors,Including market opportunities based on unmet clinical needs, the size and geographic distribution of the patient population, competitive positioning, payment environment, costs to reach specific decision points, costs of submitting regulatory filings for differentiated and reimbursable drugs, time to market, and of course, the overall risk of the plan as well as the probability of gaining FDA approval. Evaluating these factors requires clear communication between the company’s commercial and scientific teams, and such communication must always be grounded in scientific understanding and clinical needs.
Correct Culture
“The "correct culture" advocates for the pursuit of truth rather than clinical progress.Through review and analysis, we found that one important reason for the poor results of the product pipeline is,Team behaviors and decisions are encouraged and rewarded based on the number of targets. As discussed earlier, the research goals of many companies focus on quantity, such as the number of candidate drugs or the number of IND drugs that have entered clinical trials.In practice, this has led to projects focusing more on achieving phased results for candidate drugs, while paying less attention to the understanding of target biology, disease pathophysiology, the correct patient population, and a clear vision of how to develop a differentiated (and ultimately commercializable) drug.
In the analysis, the impact of a "quantity-based" strategy can also be seen in the approach to selecting alternative drugs. Typically, backup molecules are developed for critical projects with higher biological credibility, and their structures should be diverse to mitigate risks associated with compound-related issues in preclinical or early development stages, and/or offer certain substantial advantages over lead molecules. When used appropriately, this strategy can save time and maintain project momentum. However, since research institutions reward scientists based on the number of candidate drugs,We found that the backup molecules of some projects are not structurally diverse and do not show substantial improvement over the lead molecules.Although all backup candidate drugs meet the chemical standards for entering clinical trials, and the research team is considered to have achieved quantity-based goals, these molecules did not contribute to reducing project risks or improving the success rate of the project. As a result, all backup candidates in a "family of compounds" may ultimately fail for the same reasons as the lead compound, and in fact, their probability of success is no higher than that of the initial lead molecule.
In an extreme case,AstraZeneca identified seven backup molecules within a project's compound family, all of which were considered successful delivery candidates but failed due to the same preclinical toxicology findings.
This situation has led to an overly high number of backup candidate drugs in the project portfolio. At the time of writing this report, about 50% of AstraZeneca's pipeline portfolio consisted of backup molecules.
4
Since then, AstraZeneca has undergone significant reforms to learn from past experiences and has made the "5R" framework a core part of its project framework and operational model.ThisThis means that we are consciously shifting from a strategy based on high output that we previously used in R&D to one that focuses on project quality and depth of understanding as key drivers of success."." The paper emphasized.
The adoption of the "5R" framework has directly led to a significant reduction in the scale and shape of research and early development project portfolios. For the remaining or upcoming projects, each project team needs to clearly articulate their confidence in each component of the "5R" framework, identify gaps in knowledge understanding, and work hard to fill these gaps during project implementation. This, in turn, has improvedDecision-making level and transparency in project advantages and risks.
In addition to adopting this framework,AstraZeneca has also made substantial investments in certain key capabilities.For example, the ability to build personalized healthcare and biomarker support to help identify and provide data with the "right patient" dimension. As a result, 85% of projects now include personalized healthcare strategies, and our preliminary analysis shows that projects with forward-looking personalized healthcare approaches (e.g., companion diagnostics) are four times more likely to succeed (data not shown). Additionally, AstraZeneca has implemented a model-based drug discovery platform, utilizing state-of-the-art modeling and simulation methods to better understand and predict the pharmacokinetic/pharmacodynamic (PK/PD) properties of molecules, enhancing not only our understanding of the "right tissue" dimension but also our grasp of the "right target" and "right safety." Finally, by establishing payer-relevant databases, we have improved our understanding of payers and reimbursement landscapes, thereby enhancing our insight into the "right commercial potential" within the 5R framework.
Ultimately, the 5R framework does not require absolute certainty in every aspect; however, by using this framework, teams can identify key risk areas that need to be addressed during the development process. They can conduct a more objective evaluation of the project and engage in more transparent discussions with regulatory authorities. The 5R framework captures issues that may be considered critical technical aspects of a project and helps support teams in making optimal decisions at the right stage.However, the team also needs to work in the "right culture." It is crucial to ensure that the team is encouraged and rewarded when raising "critical questions," scientific quality is recognized, good connections with the external scientific community are maintained, and support is provided by experienced leaders with sound judgment.
In interviews conducted by AstraZeneca with the project team, a recurring theme emerged: the necessity of maintaining the scale of the pipeline portfolio tied individual and team rewards to project progress rather than to behaviors focused on "seeking truth." However, the scientists and clinicians within the project team needed to believe,Their personal success and career development are not inherently tied to project timelines but are related to scientific quality, prudent risk-taking, and sound decision-making.
References:David Cook 1, Dearg Brown 1, Robert Alexander, et al. Lessons learned from the fate of AstraZeneca's drug pipeline: a five-dimensional framework. Nat Rev Drug Discov. 2014 Jun;