Medtronic Faces Setbacks in the Multi-Billion-Dollar RDN Market: Clinical Trial Design Flaws and Industry-Wide Challenges

Medtronic
Medical Device Manufacturer
On August 22 and 23, 2023, the RDN (Renal Denervation) field witnessed a milestone moment.
The Circulatory System Devices Panel (CSDP, hereinafter referred to as the Panel) of the FDA held review hearings on August 22 and 23 for two representative products in the RDN field — ReCor Medical's Paradise uRDN System and Medtronic's Symplicity Spyral System. Although the Panel's voting results, or recommendations, from the review hearings are not legally binding, the final decision on whether these two products will be officially approved for marketing still rests with the FDA, which will consider the Panel’s recommendations when reviewing the products to make a final legally binding decision. It should be noted, however, that the FDA's decisions are generally consistent with the Panel's voting recommendations in most cases.
VCBeat (WeChat ID: vcbeat) interviewed Professor Wang Jie from Jiangsu Provincial People's Hospital about the results of the aforementioned meetings. Professor Wang Jie watched and listened to both meetings in their entirety. According to Professor Wang, the hearing, which lasted from 9 a.m. to 6 p.m., followed a procedure similar to that of a court trial: fair, strict, and transparent.
The voting results (see table below) showed that ReCor’s Paradise uRDN System gained clear recognition from the Panel in terms of safety, efficacy, and benefit-risk ratio. The Panel acknowledged the safety and efficacy of the Symplicity Spyral System but had a lower level of recognition for its benefit-risk ratio.
This resulted in Medtronic losing to ReCor overall. This outcome had a significant impact on the RDN industry, triggering a series of chain reactions and casting concerns and shadows over the further development of the RDN industry.
As is known to all, Medtronic and ReCor's RDN products have adopted completely different technical routes: the Symplicity Spyral system uses radiofrequency energy for renal denervation, while the Paradise uRDN system employs ultrasound energy to ablate the renal artery.
Whether the difference in voting results is due to clinical trial data or the superiority of technical approaches significantly influences the direction of industry R&D investment.

FDA Expert Panel Voting Result Statistics (Note: Panel Chair Dr. Lang cast an additional opposing vote in the event of a tie on the benefit-risk ratio for the Symplicity Spyral system, resulting in: 6 votes in favor, 7 votes against, and 1 abstention)
Medtronic has been laying out the RDN treatment for hypertension since 2010. The principle of RDN in treating hypertension is to control elevated blood pressure by blocking sympathetic nerve pathways and adjusting sympathetic nerve activity.
Medtronic estimates that a 1% market penetration rate represents a $1 billion business opportunity. They predict that the global market revenue for this technology will be at least $500 million by 2026 and at least $2-3 billion by 2030.
However, Medtronic has experienced many ups and downs in the process of developing RDN for the treatment of hypertension.In 2014, the pivotal clinical trial SYMPLICITY-HTN-III for Medtronic's first-generation RDN product failed, showing no difference in blood pressure reduction between the RDN group and the sham control group. This result dealt a severe blow to confidence in the RDN industry. In 2017, Medtronic introduced a redesigned product and a new clinical trial methodology, continuously releasing positive clinical trial data, which brought new momentum to the RDN hypertension treatment sector.
Why hasn't Medtronic, upon its return, gained more positive recognition from experts like the ReCor RDN product?
One of the key reasons is that clinical trials for RDN treatment of hypertension have extremely high execution difficulty.Few other cardiovascular disease treatment devices have undergone such long-term and large-scale clinical trials before product launch like RDN, yet still have not been approved for marketing in the United States.
Professor Wang Jie said: "The implementation difficulty of RDN studies lies in the interaction of two confounding factors: the interference of antihypertensive drugs with the blood pressure-lowering effects of RDN and blood pressure measurement.Requiring patients to not adjust their medications when their blood pressure exceeds 150 mmHg at enrollment during a six-month clinical trial follow-up period is against patient interests and unethical. However, adjusting the medication would prevent the observation of the net effect of RDN on blood pressure.
In addressing this challenge, ReCor pre-specified the blood pressure at 2 months post-operation as the primary clinical endpoint, since it is feasible to control patients without changing antihypertensive drugs within 2 months.
Medtronic extended this time frame to 6 months, and the results showed that a large number of patients in its On-Med trial switched medications, leading to numerous protocol violations and causing the 6-month results of the On-Med trial to fall short of the expected clinical endpoint.
Measuring blood pressure in RND trials also presents significant challenges:We see that ReCor has ingeniously pre-designed to use daytime systolic blood pressure in ambulatory blood pressure monitoring as the primary clinical endpoint to address this challenge, significantly reducing the execution difficulty; whereas Medtronic uses 24-hour ambulatory systolic blood pressure as the primary clinical endpoint. It can be observed that at 6 months, not only is there significant interference from medications, but also a large amount of missing data for 24-hour ambulatory blood pressure due to the high execution difficulty, which has led to repeated inquiries from the Panel members on how to handle the missing data."
In 2022, Medtronic reported that in its pivotal clinical trial, the SPYRAL HTN-ON MED Expansion trial, the 6-month follow-up results showed a 6.5 mmHg reduction in 24-hour ambulatory systolic blood pressure in the RDN group and a 4.5 mmHg reduction in the control group (between-group treatment difference: -1.9 mmHg, p=0.119), failing to reach the pre-specified endpoint. They attributed the cause to the impact of the COVID-19 pandemic, which prevented proper execution of the trial protocol and led to excessive use of antihypertensive medications in the sham control group.
Professor Wang Jie believes: "This is precisely the result of underestimating the difficulty of maintaining drug adherence over a six-month period and preventing patients from adjusting their medications, which led to experts continuously questioning Medtronic during the hearing."
Although ReCor's clinical trials were relatively small in scale, they had clear objectives. Among the three clinical trials conducted, including two Off-Med trials, Radiance II and Radiance-HTN SOLO, and one On-Med trial, Radiance TRIO, the primary efficacy endpoint was the daytime ambulatory systolic blood pressure at two months. According to ReCor’s interpretation, all three trials reached their pre-specified clinical endpoints (see figure below). The consistent results of these three clinical trials indicate that the Paradise uRDN system can safely and effectively reduce patients' blood pressure. This is a key factor for ReCor’s product gaining expert recognition.
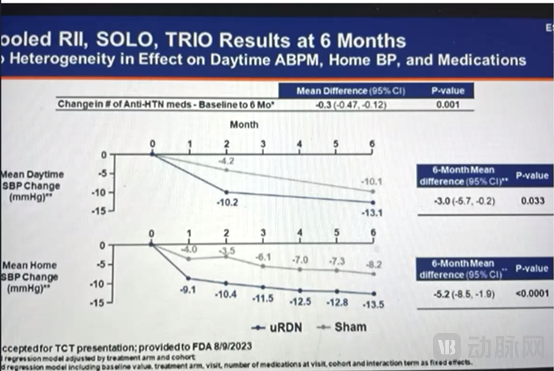
Professor Wang Jie believes: "Compared to Medtronic using the 24-hour ambulatory blood pressure change over six months as the endpoint, using the daytime ambulatory systolic blood pressure at two months as the primary efficacy endpoint can better control drug interference. Daytime ambulatory blood pressure is also relatively easier to obtain. Although the number of patients treated with the Paradise uRDN System in ReCor's three clinical trials did not exceed 300, Recor’s clinical trial design clearly demonstrated to the Panel members that its results fully met the expected clinical trial endpoints."
Imagine if Medtronic had set the 24-hour ambulatory systolic blood pressure or even office systolic blood pressure at 3 months as the primary clinical endpoint for its On-Med trial, instead of using the 24-hour ambulatory systolic blood pressure result at 6 months as the primary clinical endpoint. If they had been more patient and waited instead of conducting an interim analysis upon obtaining data from 40 pairs of patients, there is a good chance the results could have been completely different."
Professor Wang Jie further explained: "I believe that Medtronic's setback is due to the flaws in the clinical trial design, not the failure of its RDN radiofrequency ablation system.This conclusion is drawn from the very similar response rates to RDN treatment among hypertensive patients in the ReCor and Medtronic trials (RADIANCE II 64%, SOLO 66%, TRIO 61%; Spyral Off-Med 65%; On-Med 61%. Based on a blood pressure reduction of >5mmHg), especially when comparing the Off-Med results between the two, as this represents the net effect of RDN on blood pressure without drug interference. Another perspective is that neither the ReCor nor the Medtronic On-Med trials reached their pre-specified clinical endpoints (according to the FDA's analysis of ReCor TRIO’s two-month results, which did not meet the anticipated endpoint). This outcome also highlights the challenges of conducting On-Med clinical trials for RDN in treating hypertension. Therefore, several members of the Panel repeatedly suggested during discussions that composite clinical endpoints incorporating both blood pressure and medication load should be applied in future trials.

The final voting result of the Panel does not represent the FDA's approval decision on the two RDN devices under review. Overseas analysts believe that Medtronic's RDN Spyral system still has a chance to be approved for marketing. For example, in the statements made by Panel members after the vote, including Chairman Dr. Lange, they all indicated that if Medtronic modifies its requested indications, they would change their decisions.
Due to the differences in Panel members' recognition of ReCor and Medtronic's RDN products, almost all relevant people in China believe that this indicates the superiority of the ultrasound ablation technology route over the radiofrequency ablation technology route, with ReCor’s product achieving better clinical outcomes. Can this conclusion be drawn from the data disclosed at the FDA review meeting?
A large amount of efficacy data for the Simplicity Spyral system and Paradise uRDN system was presented at the FDA expert hearing, providing us with the possibility to compare clinical trial data from both systems.
In clinical trials without medication from both companies, Medtronic's SPYRAL-HTN OFF MED trial results showed,The average 24-hour ambulatory systolic blood pressure in the RDN group decreased by 4.7 mmHg at three months post-operation, compared to a 0.6 mmHg reduction in the sham control group, with an intergroup difference of -4.1 mmHg.; The changes in office systolic blood pressure were: -9.2 mmHg in the RDN group, -2.5 mmHg in the control group, with an intergroup difference of -6.7 mmHg.
Results of ReCor’s RADIANCE SOLO trial showed that at 2 months, the reduction in daytime ambulatory systolic blood pressure was -8.5 mmHg in the RDN group and -2.2 mmHg in the sham group, with an intergroup difference of -6.3 mmHg. The 24-hour ambulatory systolic blood pressure reduction at 2 months was -7.0 mmHg vs -3.1 mmHg, with an intergroup difference of -4.1 mmHg.

Comparing the 24-hour dynamic systolic blood pressure of the two companies, the intergroup difference for ReCor was -4.1 mmHg; for Medtronic, it was also -4.1 mmHg.
According to the data released at the expert review meeting, the difference in daytime ambulatory systolic blood pressure between the Recor surgical group and the sham surgery control group was only -3 mmHg six months post-operation, with questionable statistical significance. However, the change in medication load between the groups showed a statistically significant difference (p < 0.001). See the figure below.
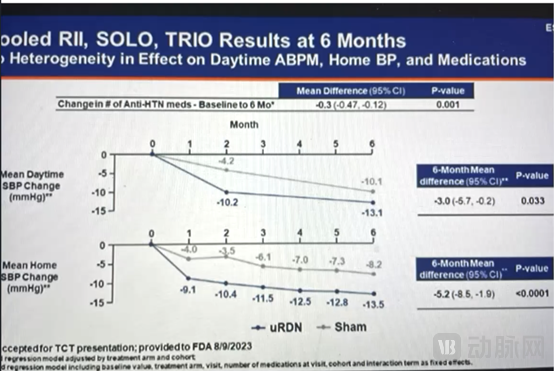
Therefore, based on the clinical trial data of both, it cannot be concluded that ultrasound technology is superior to radiofrequency technology.In addition to the blood pressure-lowering effect, ReCor's product did not further increase the patients' antihypertensive response rate (see above). The products of both companies are at the same level in this indicator. Whether it is ReCor or Medtronic, the clinical trial response rates are slightly higher than 60%.
Radiofrequency ablation has been widely used in clinical practice. Ultrasound ablation is not as widely applied in clinical settings as radiofrequency ablation. The challenge faced by ultrasound ablation technology lies in the complexity of product structure and manufacturing processes, including balloons, ultrasound transducers, and cooling systems. In an ultrasound balloon catheter, piezoelectric crystals must be reasonably arranged, and to avoid damaging the vascular anatomy, it is necessary to circulate cooling water within the balloon. This further increases the complexity of the process and manufacturing.
During the two-day long review meeting, what issues in the RDN field did the Panel members think need further resolution?
First is the necessity of continuous research after market launch.。During ReCor's review meeting, the Panel members unanimously and clearly stated that if the RDN device is approved, post-marketing studies will provide further clinical evidence needed to complete the RDN therapy and related technologies, to address many of the remaining issues with this therapy, particularly the duration of efficacy and benefits. The Panel members were especially concerned about the safety and effectiveness of using RDN to treat hypertension in minority groups such as the African American population.
Professor Wang Jie also pointed out that post-marketing research and continuous follow-up are very important. We need to establish a complete and long-term chain of evidence from China.
Chinese companies should learn from the experiences of ReCor and Medtronic, paying attention to the design and operability of clinical trial protocols.Particularly in two expert meetings, most experts mentioned the drug index and the clinical endpoint design combining blood pressure and drug dual indicators. In this aspect, Chinese scholars have taken the lead globally by applying a dual clinical endpoint that incorporates both blood pressure and drug load index, launching RCT trials for RDN treatment of hypertension to verify the safety and efficacy of domestically produced RDN products.
As the medical device industry in China continues to develop and reach the global stage, what we learn should not only be technology but also reference fair, rigorous, and transparent review processes.
There are four parties involved in the FDA review hearing: the Sponsor, FDA officials and professionals, the public, and Panel members, including those with voting rights and those without. Panel members include interventional cardiologists, hypertension specialists, nephrologists, statisticians, public representatives, and industry representatives. The Panel has a chairperson who can cast an additional vote to break a tie in the event of a deadlock during voting on a particular issue.
The discussion procedure for the two products at the meeting was identical: First, the manufacturer presented the data and then answered questions. Next, the FDA analyzed the data submitted by the manufacturer independently, presented the same set of data, and responded to questions; the analysis of certain data might differ from that of the manufacturer. The time allocated to the manufacturer was exactly the same as the time given to the FDA. This was followed by public comments, Panel members asking questions to the manufacturer, and the FDA listing several questions directly related to the three voting questions. Each Panel member with voting rights was asked individually for their clear opinions on these questions to guide their stance on the final three voting questions.
For example, the FDA asked ReCor and Medtronic 9 and 10 questions respectively. The answers to these questions directly determined the Panel members' opinions on the three major issues of product safety, efficacy, and risk/benefit. After the final vote, each voting member had to explain the reasons for their Yes or No vote. In this "court trial," the role of the Panel was equivalent to the "jury," while the role of Dr. Zuckerman, Director of the FDA's Office of Cardiovascular Devices, was similar to that of a "judge," but not identical. His role was to provide explanations and make decisions when discussions involved certain regulatory-related disputes. The statements made by the manufacturers and the FDA were equivalent to the cross-examination of both parties by the "jury," which is the Panel.
The Panel's opinions can help companies developing RDN products improve their products, design reasonable and feasible clinical trials, and address encountered issues, forming a new consensus on how to validate the safety and efficacy of RDN. It is hoped that this detailed process of "observing" international peers thoroughly evaluate a cutting-edge product in the cardiovascular field will inspire and promote the research and development of medical devices in China.