Dawn Breaks for 'Undruggable' KRAS Target: Elicio Therapeutics Files IPO Prospectus Highlighting ELI-002 Cancer Vaccine Pipeline

Elicio Therapeutics
Developer of Novel Immunotherapy
Breaking News
2023-09-05, Elicio Therapeutics, focused on developing cancer immunotherapies, announced that additional data from the Phase I study (AMPLIFY-201) of its lead pipeline candidate ELI-002 will be presented in a poster session at the AACR Special Conference on Pancreatic Cancer held in Boston from 2023-09-27 to 2023-09-30. This data will supplement the interim results Elicio presented at the ASCO Annual Meeting in June 2023.
The AMPLIFY clinical program for ELI-002 currently includes the ELI-002 2P (2-peptide) and ELI-002 7P (7-peptide) formulations: The 2P formulation is designed to position ELI-002 as a monotherapy targeting patients with two KRAS mutations, G12R and G12D, which are the most common variants in pancreatic cancer, colorectal cancer, non-small cell lung cancer, ovarian cancer, cholangiocarcinoma, and gallbladder cancer; the 7P formulation aims to expand the therapeutic potential to include the seven most common KRAS mutations: G12D, G12V, G12R, G12C, G12S, G12A, and G13D.
The first-in-human Phase I AMPLIFY-201 clinical trial evaluated the safety, immunogenicity, and anti-tumor activity of the therapy (ELI-002 2P) in patients with minimal residual disease (MRD) after standard local treatment. Enrolled patients had elevated ctDNA and/or tumor markers (CA19-1/CEA) and KRAS/NRAS mutations. Data presented at the ASCO Annual Meeting in June 2023 showed that ELI-002 was well tolerated, with no dose-limiting toxicity or cytokine release syndrome; a significant proportion of patients experienced a reduction in tumor biomarkers (77%), with 32% achieving complete clearance; robust mKRAS-specific T-cell responses were induced in 87% of patients.
About the anticancer peptide vaccine ELI-002
1. A Potential Breakthrough for KRAS—ELI-002
KRAS is the most frequently mutated gene in cancer and is also considered by the medical community as an "undruggable target." Statistics show that the probability of KRAS gene mutations in patients with pancreatic cancer, colon cancer, endometrial cancer, and lung adenocarcinoma are 61%, 43%, 21%, and 26%, respectively. Moreover, if cancer patients have an activating mutation of KRAS in their tumors, the efficacy of conventional EGFR-targeted therapies, such as Cetuximab and Gefitinib, tends to be generally poor. Patients with KRAS-activating mutations usually have a poor prognosis, with survival times often significantly shorter than those without KRAS-activating mutations.
The reason why KRAS remains unconquered is that the KRAS protein has a featureless, nearly spherical structure with no obvious binding sites, making it difficult to synthesize a compound that can specifically target and inhibit its activity.
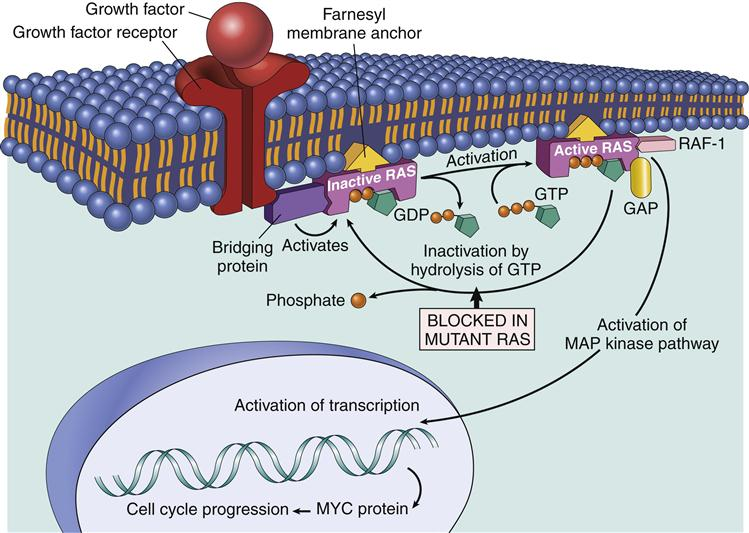
Figure 1. KRAS Target Mechanism
For the "undruggable" target KRAS, ELI-002 takes a different approach by employing cancer immunotherapy (Cancer Immunotherapy or Immuno-oncology) to effectively deliver antigen peptides into the lymphatic system, activating the body's immune system to kill tumor cells. It is expected to become the first anticancer peptide vaccine capable of eliminating KRAS-mutant solid tumors.
Specifically, the ELI-002 therapeutic cancer vaccine developed based on Elicio's AMP platform consists of two components: one is KRAS mutant peptide antigens modified by the AMP platform, where ELI-002 2P uses a 2-peptide formulation targeting two mutation sites, and ELI-002 7P uses a 7-peptide formulation targeting seven mutation sites; the other component is ELI-004, an immunostimulatory oligonucleotide adjuvant modified by the AMP platform and developed by Elicio.
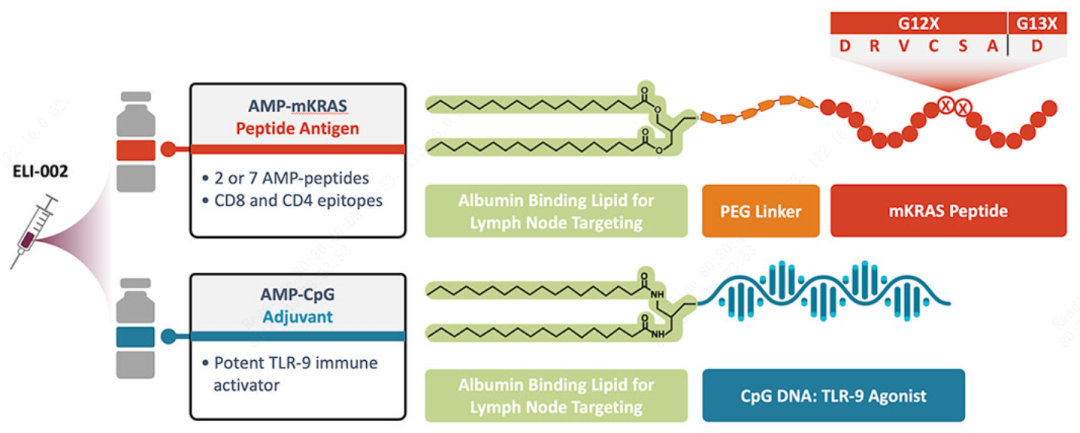
Figure 2. Composition of ELI-002
Among them, the KRAS mutant peptide antigen plays a role in activating specific immunity: the complex formed by the antigen and lipids (PEG) is linked to albumin and enters the lymphatic circulation through injection. When circulating to the lymph nodes, the albumin-antigen complex will be processed by antigen-presenting cells such as dendritic cells, presenting the antigen to CD4+ T cells and CD8+ T cells, thereby leading to the secondary activation of T cells, fully activating the T cells. The activated T cells kill specific cells based on the antigen, achieving an anti-tumor effect.
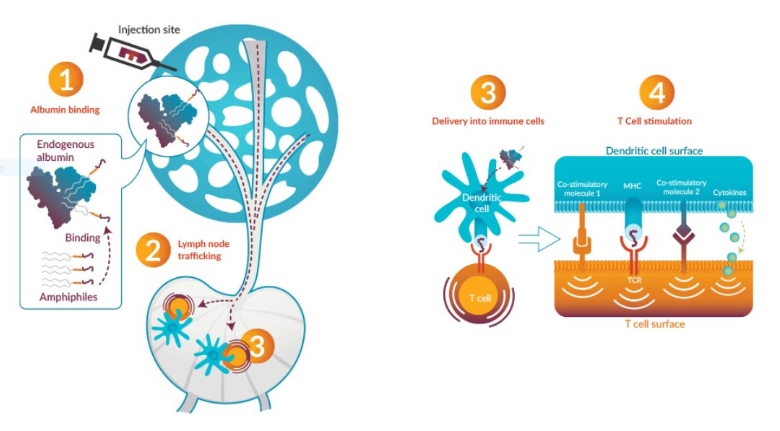
Figure 3. Mechanism of Action of ELI-002
Another component is ELI-004, which plays a role in enhancing the immune response: ELI-004 consists of an AMP complex and CpG DNA, with the former used for lymph node targeting and the latter, CpG, being a common immune enhancer to boost the immune response. As an antigen, it stimulates CD4 T and CD8 T cells to initiate proliferation and differentiation programs to generate an immune response, strongly inducing the production of pro-inflammatory cytokines. Preclinical study results have demonstrated the immune-enhancing capability of ELI-004, showing greater immune enhancement strength compared to other immune enhancers.
From the preclinical results, ELI-002 demonstrated strong and effective therapeutic capabilities. After modification by the AMP platform, ELI-002 showed an over 400-fold increase in immune response for KRAS G12D and over a 60-fold increase for KRAS G12R compared to directly injecting unmodified antigen peptides and CpG DNA.
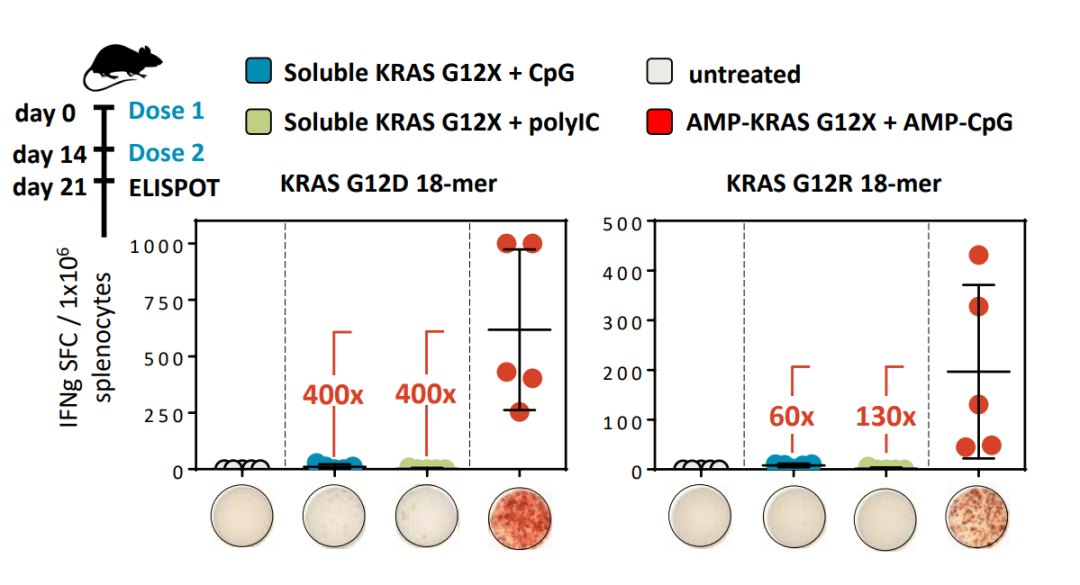
Figure 4. ELI-002 Preclinical Data
2. Elicio's Core Technology—AMP Modification Platform
The reason why ELI-002 immunotherapy can demonstrate such a powerful cancer cell-killing effect is inseparable from the contribution of the lymph node-targeting amphiphile (AMP) technology platform.
AMP is essentially a bioconjugation technology platform composed of three parts: combining Albumin-binding Lipid with Payload through a Polymeric Linker to form a macromolecular complex, enabling stable and efficient targeted delivery of antigen peptides into the lymphatic system to take effect. The payload modified by AMP can be small molecules, peptides, nucleic acids, proteins, etc. This platform is the core technology platform of Elicio Therapeutics, and Elicio currently owns all patent rights to the AMP platform.
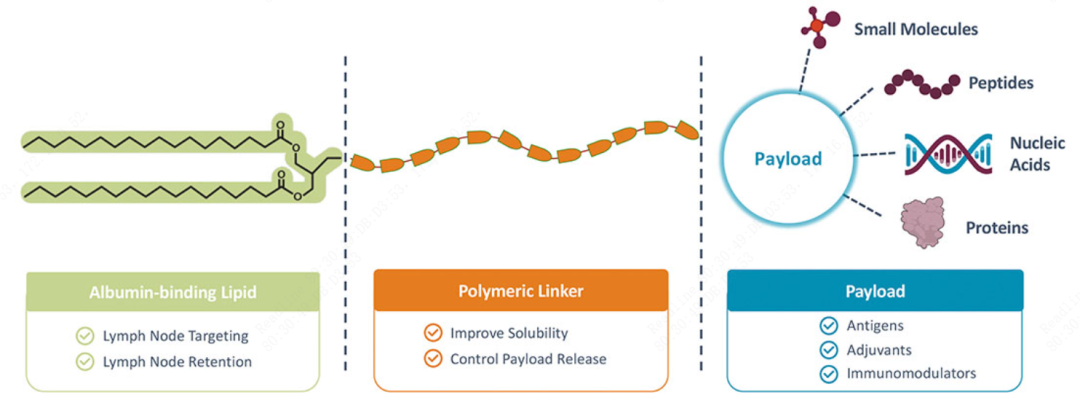
Figure 5. AMP Modification Platform Architecture
Darrell Irvine, the founder of Elicio Therapeutics, is the Deputy Director of the MIT Koch Institute, a professor of Biological Engineering and Materials Science and Engineering, as well as an investigator at the Howard Hughes Medical Institute. He focuses on the development of innovative immunotherapies. Prior to founding Elicio, Darrell Irvine conducted a series of research experiments addressing two critical issues in current CAR-T cell therapy for solid tumors: antigen heterogeneity and the loss of tumor target antigens. These efforts laid the technical foundation for the AMP platform.
Enhanced CAR–T cell activity against solid tumors by vaccine boosting through the chimeric receptor
The study identified the underlying technology of the AMP platform: one achievement is a targeted delivery technology for the lymphatic system, and the other involves addressing tumor cell escape mechanisms caused by the cessation of target antigen expression through the administration of antigen peptides. This approach also drives an antigen spreading (AS) response, which helps engineered CAR-T cells attack tumors.
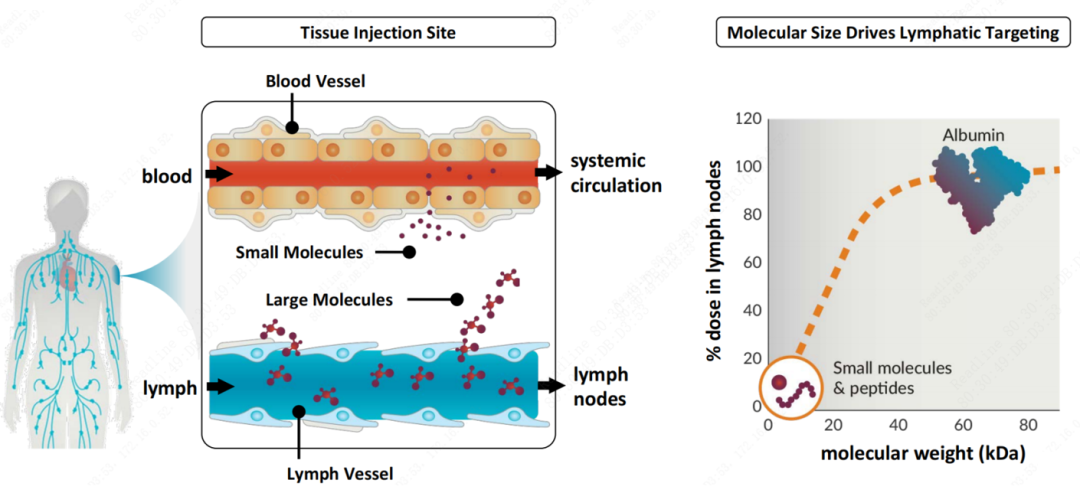
Figure 6. Serum albumin can effectively achieve efficient delivery to the lymphatic system.
Overall, Elicio has built a proprietary AMP immunotherapy platform based on a series of research trial results, giving it the advantages of reproducibility, interchangeability, multifunctionality, applicability to various diseases, long-lasting effects, and high potency. Specifically, covalently conjugated macromolecular complexes modified through the AMP platform have three characteristics:
① More Accurate: Albumin, after being modified with lipids, enhances its targeting specificity to lymph nodes;
② More stable: Conjugating the target antigen with albumin can enhance antigen stability and promote targeted antigen release;
③ More Flexibility: Antigen selection is flexible, allowing for the initial choice of antigens with optimal functionality through chemical/structural simulation. Since albumin-loaded antigens can include small molecules, peptides, nucleic acids, proteins, and other types of antigens, this broadens the range of antigen selection.
Progress in the Development of Peptides in the Field of Cancer
Malignant tumors pose a serious threat to human health, with their incidence and mortality rates continuing to rise in recent years. The global situation for cancer prevention and control remains severe. Despite breakthrough progress in immunotherapy in recent years, surgery, radiotherapy, and chemotherapy are still commonly used clinical treatments for cancer. Finding safe, rational, and effective cancer treatment methods is an urgent issue that needs to be addressed in the field of cancer treatment.
Peptide drugs have the advantages of low immunogenicity, good tissue permeability, ease of synthesis and modification, high safety, and low tendency to accumulate in tissues. They have shown significant efficacy in anti-tumor, antibacterial, chronic metabolic diseases, cardiovascular diseases, and immune diseases. Moreover, the anti-tumor mechanisms of peptide drugs are diverse, inhibiting tumor occurrence and development through promoting tumor cell apoptosis, suppressing tumor angiogenesis, and activating the body's anti-tumor immune response, indicating broad application prospects.
1. Classification of Anti-Cancer Peptide Drugs
Anticancer peptides (ACPs) have a highly diverse range of sources and are widely present in various organisms, including mammals, amphibians, insects, plants, and microorganisms. Anticancer peptide drugs offer numerous advantages in tumor treatment, such as low molecular weight, simple structure, high anticancer activity, high selectivity, fewer side effects, multiple administration methods, and a lower likelihood of inducing multidrug resistance.
From the perspective of the mechanism of action, anticancer peptide drugs can be divided into the following four categories:
The first class of anticancer peptide drugs slows down the growth of tumor cells and disease progression by inducing hormonal castration to control the development of the condition, including luteinizing hormone-releasing hormone (LHRH) and somatostatin (SST) types.Such as Goserelin, a representative drug of synthetic gonadotropin-releasing hormone (GnRH) agonists, is a decapeptide analog of luteinizing hormone-releasing hormone (LHRH). For a long time, androgen deprivation/suppression therapy represented by gonadotropin-releasing hormone (GnRH) agonists has been the cornerstone treatment for prostate cancer and breast cancer patients. Medical castration involves the long-term and continuous suppression of sex hormone activity through hormone therapy drugs to control disease progression.
As early as 1971, the medical community had discovered and elucidated the structure of LHRH. Subsequently, researchers began synthesizing LHRH analogs with higher activity, achieving breakthrough progress in a short period. Following this, drugs like goserelin and buserelin emerged rapidly, driving the prosperity of this class of medications. Since then, hormonal drugs have been continuously updated and replaced, with manufacturers striving to create "me better" products by improving formulations, such as sustained-release microspheres. For example, in 1986, the French company Ipsen developed triptorelin sustained-release microspheres, and on June 30, 2023, Luye Pharma's goserelin microsphere was approved. These advancements represent upgrades to existing formulations, enhancing drug efficacy and patient compliance.
From the perspective of marketed drugs, (GnRH) agonist anti-cancer polypeptide drugs have the longest marketing time and the largest number of marketed drugs, which is related to the indications they mainly target, such as prostate cancer and breast cancer.Globally, prostate cancer is the second most common malignant tumor in men, second only to lung cancer. Breast cancer is a common malignant tumor in women, with its incidence and mortality ranking first and fourth, respectively, among malignant tumors in Chinese women. Due to hormone therapy being the preferred treatment for prostate and breast cancer, it has driven the increase in sales of GnRHa peptide drugs. Taking AstraZeneca's Zoladex (goserelin) alone, it has dominated the market for more than two decades. Although its global sales from 2001 to 2021 have seen some fluctuations, overall, it remains an "evergreen drug," maintaining continuous growth over five years, with sales reaching $927 million in 2022 and $948 million in 2021.
Somatostatin (SST) analogs, including Lanreotide and Octreotide, are primarily indicated for neuroendocrine tumors and gastroenteropancreatic neuroendocrine tumors. Their mechanism of action is similar to that of endogenous somatostatin, inhibiting the release of anterior pituitary hormones, including thyroid-stimulating hormone and growth hormone, as well as hormones of the gastrointestinal endocrine system, such as insulin and glucagon. In terms of drug sales, Lanreotide has maintained steady growth over the past three years, with sales reaching $1,218 million in 2022; Octreotide sales have slightly declined over the past three years, with sales amounting to $1,238 million in 2022.
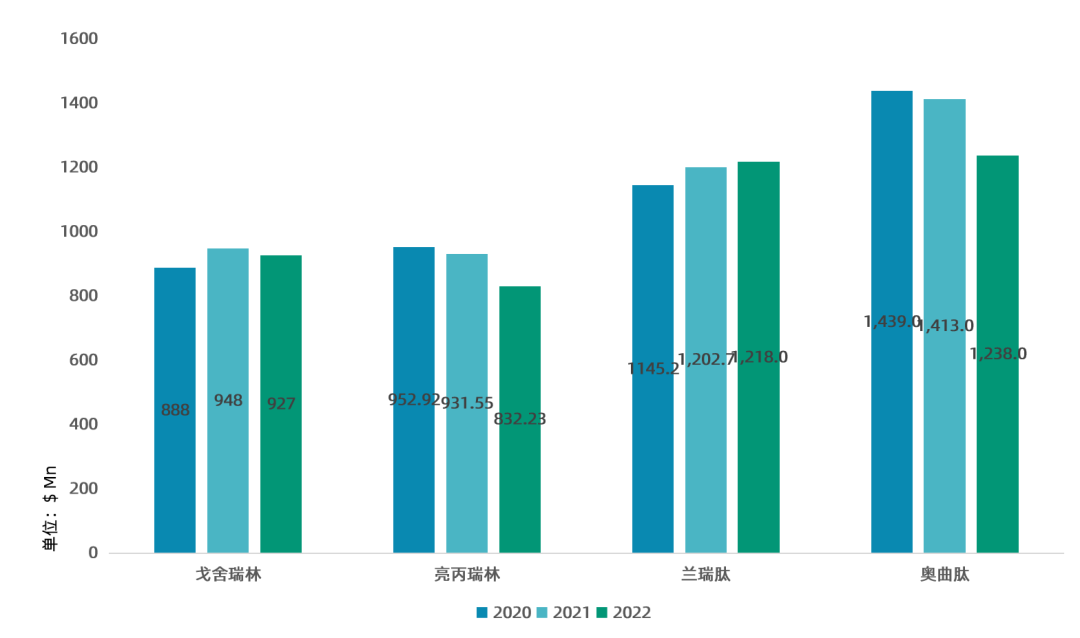
Figure 7. Sales of Hormonal Anticancer Peptide Drugs
From this perspective, hormone-related peptide drugs are common treatments for tumors influenced by sex hormones, such as breast cancer, prostate cancer, and neuroendocrine tumors. The clinical advantage of these products lies in the organic combination of the drug's physicochemical properties and formulation technology, upgrading the original efficacy through advancements in formulation types. Despite their significant role in clinical practice due to their proven efficacy and long history of use, hormone-related peptide drugs have substantial drawbacks in terms of drug resistance and targeting. The use of hormone-based anticancer drugs ultimately leads to certain resistances. For example, nearly all patients with advanced prostate cancer will eventually progress to castration-resistant prostate cancer (CRPC) after receiving androgen deprivation therapy. Metastatic castration-resistant prostate cancer (mCRPC) is the primary cause of mortality, and the prognosis for metastatic prostate cancer that has developed resistance to castration therapy is very poor, with a 5-year survival rate of approximately 30%. Therefore, the development of peptide anticancer drugs with stronger targeting capabilities and the ability to directly kill cancer cells is an inevitable direction.
The second class of anticancer peptide drugs are peptides that play a role in targeting and positioning cancer cells, and the representative drug is PDC conjugate.PDC drugs covalently link specific peptide sequences to cytotoxins via a linker. Homing peptides, acting as the "precision guidance system" of PDC drugs, possess high specificity and strong binding affinity to overexpressed receptors on the surface of cancer cells. Depending on the radionuclide payload of PDCs, PDC conjugates serve two major functions: therapy and diagnosis. The most significant feature of PDC drugs is their ability to "quickly, precisely, and powerfully" eradicate cancer cells.
Table 2. Partial PDC Drug Pipeline Status
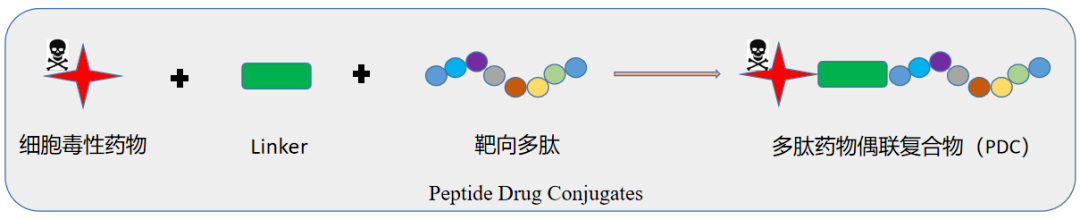
Figure 8. PDC Drug Structure
PDC Drugs Become an Important Direction in the Field of Precision Oncology. On March 23, 2022, Novartis' targeted radioligand therapy Pluvicto was approved for the treatment of patients with metastatic castration-resistant prostate cancer positive for prostate-specific membrane antigen (PSMA). This is also the first FDA-approved targeted radioligand therapy for treating such patients.Pluvicto was in short supply as soon as it was launched, with sales of $271 million in 2022. Sales in 2023 are expected to exceed $900 million, representing a year-on-year increase of 332%.
PDC, as a novel therapeutic approach, can overcome certain limitations of current ADCs, demonstrating significant advantages in cell penetration, metabolic rate, large-scale synthesis speed/cost, and immunogenicity.
The third class of anticancer peptide drugs exerts immune activation and immune targeting effects.Personalized cancer vaccines like ELI-002 can be used for direct injection, stimulating autologous T cells while combining with CAR-T therapy to specifically kill tumor cells, achieving the effect of treating tumors or preventing postoperative recurrence. Mifamurtide, a synthetic muramyl tripeptide phosphatidylethanolamine (L-MTP-PE), is a component of mycobacterial cell walls and has natural immunogenicity in humans. After being taken up by macrophages in the body, Mepact® releases mifamurtide, which kills tumor cells by activating macrophages. Clinical studies have shown that the combination of mifamurtide with chemotherapy drugs such as cisplatin can reduce the mortality rate of osteosarcoma patients by 30%, with 78% of patients surviving more than six years after treatment.
Tumor immunotherapy has shown great anti-cancer potential, activating the immune system to target malignant tumors. Long peptide (SLP) vaccines are a primary method in neoantigen-based tumor therapy. Synthetic peptide-based neoantigen vaccines have been applied in multiple clinical trials, and some trials have already demonstrated the anti-tumor efficacy of peptide neoantigen vaccines.
In addition to ELI-002, iNeo-Vac-P01, an injectable developed independently by China's Nuo Anjin Biotechnology, has also received clinical trial approval and entered Phase I clinical trials for the treatment of patients with high recurrence risk after radical surgery for solid tumors. On September 29, 2022, Nuo Anjin Biotechnology published a clinical study titled "Combination Treatment of Radiofrequency Ablation and Peptide Neoantigen Vaccination: Promising Modality for Future Cancer Immunotherapy" in the journal *Frontiers in Immunology*. The disclosed results showed that if patients with advanced pan-cancer underwent local radiofrequency ablation (RFA) within six months prior to receiving iNeo-Vac-P01 treatment, it could further improve the tumor microenvironment and enhance clinical efficacy. The research team also validated the anti-tumor synergistic effects of RFA and iNeo-Vac-P01 through mouse models; they further discovered that the combination therapy of RFA, iNeo-Vac-P01, and immune checkpoint inhibitors could enhance antigen-specific immune responses and improve tumor suppression, providing a feasible and effective new immunotherapy combination regimen for patients with advanced solid tumors who failed standard treatments.
The fourth class of anticancer peptide drugs refers to peptides that exert inhibitory effects on cell growth and proliferation or directly target and kill cancer cells through various mechanisms.Among the marketed drugs, one type exerts RNA inhibitory effects similar to nucleoside analogs, while the other type acts as proteasome inhibitors. For instance, Dactinomycin D (trade name Cosmegen) can inhibit RNA synthesis, interfere with the transcription process of mRNA in cells, and when used in combination with radiotherapy, it can enhance the sensitivity of tumors to radiation treatment.
Bortezomib is a first-generation proteasome inhibitor, and carfilzomib is a next-generation tetrapeptide epoxyketone proteasome inhibitor of the 26S proteasome following bortezomib. This drug inhibits the 26S proteasome, preventing the targeted proteolysis of ubiquitinated proteins, and the disruption of this normal pathway can affect multiple signaling pathways within cells, leading to cell death. Carfilzomib is used to treat patients with multiple myeloma whose condition continues to progress after treatment with other anticancer drugs. Since its launch in 2012, sales have been increasing year by year, reaching $1247Mn in 2022, making it the highest-selling anticancer peptide drug of that year.
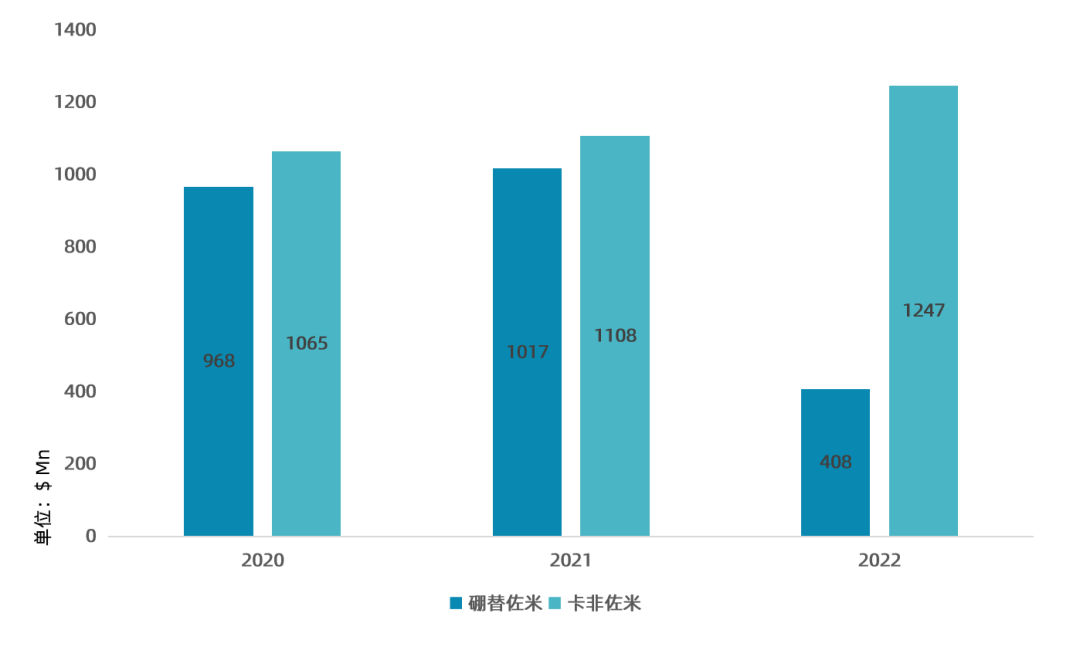
Figure 9. Sales of Peptide Drugs with Proteasome Inhibitors
2. Market Landscape of Anti-Cancer Peptide Drugs
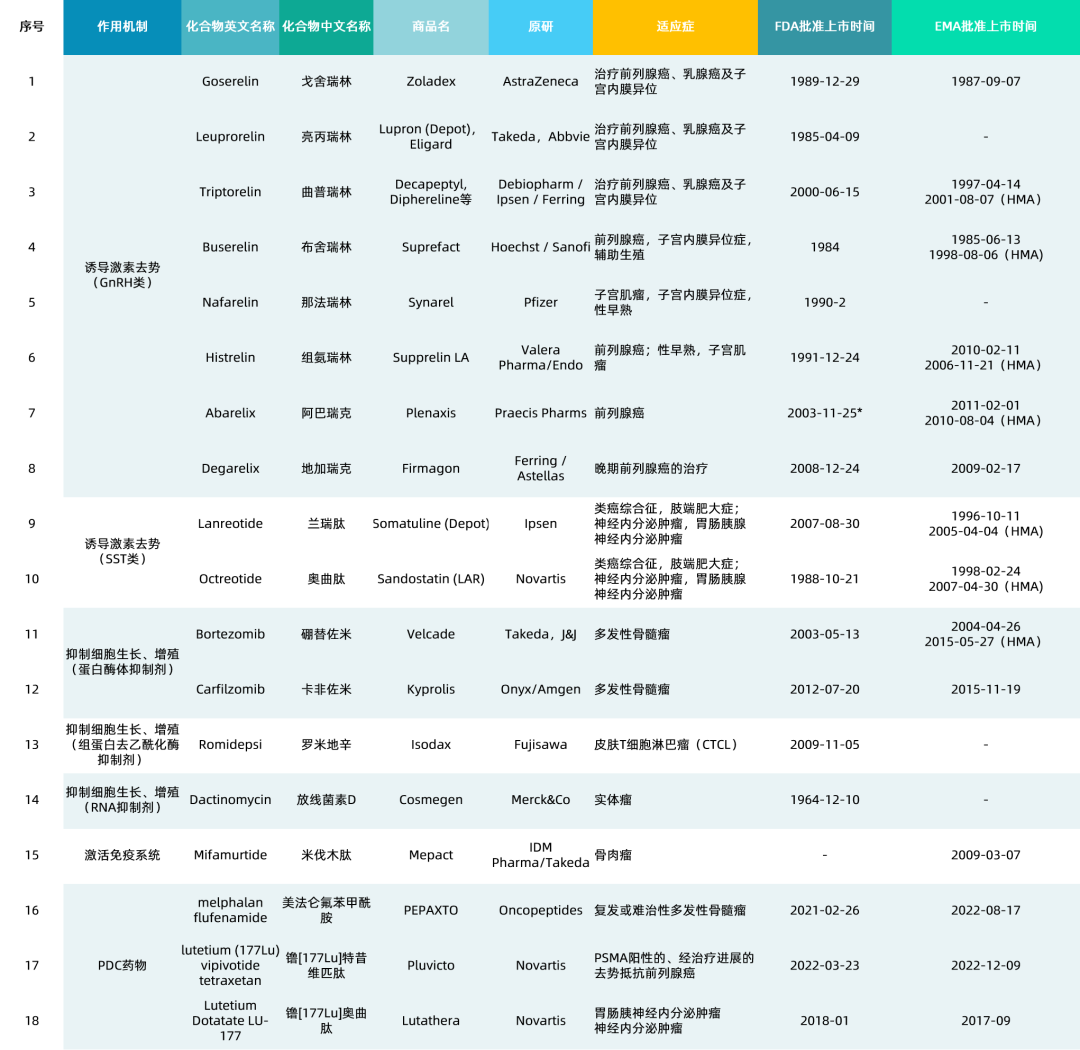
According to the above four classification mechanisms, Peptide Research Society has collected 18 anti-cancer peptide drugs. From the perspective of the number of marketed anti-cancer peptides, the largest proportion is occupied by peptide-induced hormone drugs for castration therapy, among which there are 8 Gonadotropin-releasing hormone (GnRH) drugs and 2 Somatostatin (SST) drugs, totaling 10 drugs, accounting for 49% in total; There are 6 anti-cancer peptides (including proteasome inhibitors, histone deacetylase inhibitors, and RNA inhibitors) that inhibit cell growth and proliferation, accounting for 34% in total; There are 3 PDC anti-cancer drugs on the market, namely PEPAXTO, Pluvicto, and Lutathera, accounting for 5%; There is only one drug, Mifamurtide, that achieves anti-cancer effects by activating the immune system, which accounts for the smallest proportion.
From the data, there is currently no anticancer peptide vaccine on the market, and the market potential remains to be tapped.
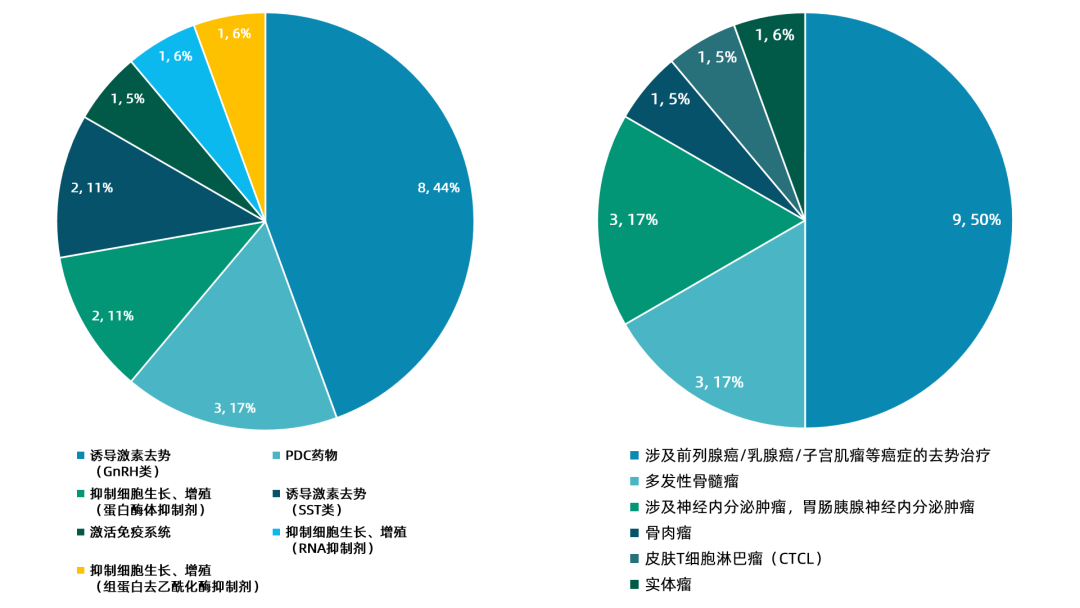
Figure 10. Number and Indication Distribution of Marketed Anti-Cancer Peptide Drugs
In terms of indications, since the number of anticancer peptide drugs in the classes of luteinizing hormone-releasing hormone (GnRH) and somatostatin (SST) is relatively large, the indications for prostate cancer and breast cancer account for the largest proportion, reaching 50%. Multiple myeloma and neuroendocrine tumors are the second largest indications, with three drugs each, accounting for 17% respectively. Osteosarcoma, solid tumors, and cutaneous T-cell lymphoma (CTCL) each have one drug. It can be seen that there are currently fewer anticancer peptides targeting the clearance of solid tumors, with only Actinomycin D available.
If ELI-002 can successfully come to market in the future, it will be a strong addition to the anticancer peptide immunotherapy drug market.
Table 1. Overview of Marketed Anti-Cancer Peptide Drugs
Summary
Compared with small-molecule chemical drugs, polypeptide drugs have the advantages of good selectivity and specificity, and low toxic and side effects. Compared with monoclonal antibody drugs, they have the advantages of low cost, good tissue permeability, and easy modification, etc., thus receiving extensive attention in the research of tumor treatment drugs. In recent years, important progress has been made in tumor immunotherapy, which is also inseparable from the role played by polypeptides. Polypeptides can not only act as tumor antigens to activate anti-tumor immunity, but also block immune checkpoint molecules.
Currently, the majority of anti-tumor peptide drugs on the market are hormone analogs, while there are relatively fewer drugs that act as target-blocking agents. The main reasons are the short half-life of peptide drugs and the difficulty in achieving sufficiently high effective concentrations. The future development of peptide drugs will continue to build on existing peptide leads, utilizing methods such as bioinformatics and high-throughput combinatorial chemistry for rational and effective design and screening, aiming to improve their retention time in the body, targeting ability, and physicochemical properties.
[1] Peptide Research Society: Anti-Tumor Peptides (10) —— An Overview of Marketed Anti-Tumor Peptides
[2] Custom Peptides: Advances in the Mechanism of Action of Anticancer Peptides
[3] Oncology Society: Latest Research Progress in KARS Targeted Therapy
[4] Elicio Therapeutics Official Website
- END -

Flagship Report
Column Recommendation




Peptide Research Society

In-Depth Research Report on Medical Health
"Strategy Team Organization" New Consulting