Semaglutide: Beyond Glycemic Control and Weight Loss — A Multifaceted Therapeutic Powerhouse

Novo Nordisk
Insulin Developer and Manufacturer
Express
On October 10, 2023, Novo Nordisk announced that the Phase III clinical FLOW trial of Semaglutide for treating Type 2 diabetes patients with renal insufficiency and chronic kidney disease was terminated early due to excellent efficacy. The decision to stop the trial was based on the recommendation of the Independent Data Monitoring Committee (IDMC). The clinical results remain blinded to Novo Nordisk and are expected to be unblinded in H1 2024.
Figure 1. Novo Nordisk Official Website News
FLOW is a randomized, double-blind, parallel-group, placebo-controlled Phase III trial designed to compare injectable Semaglutide 1.0 mg with placebo as an adjunct to standard care in preventing the progression of kidney damage, as well as renal and cardiovascular death risks, in patients with type 2 diabetes and chronic kidney disease (CKD). The trial was initiated in 2019 across more than 400 study sites in 28 countries, with a total of 3,534 participants enrolled.
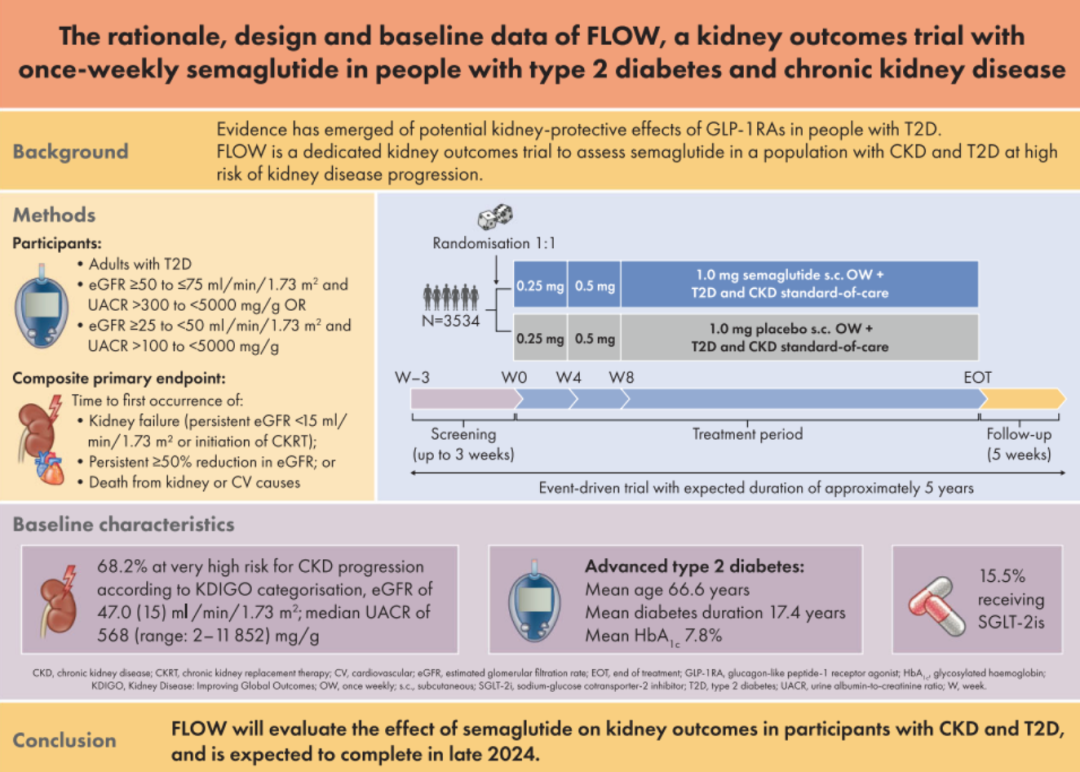
Figure 2. FLOW Clinical Design
The FLOW trial demonstrates Semaglutide's ability to delay the progression of chronic kidney disease and reduce the risk of renal and cardiovascular death through several primary composite endpoints, specifically including: a sustained decline in eGFR1 ≥ 50% from baseline, the time eGFR1 remains <15 mL/min/1.73m², the time to initiation of chronic kidney replacement therapy (dialysis or kidney transplantation), and mortality due to kidney disease or cardiovascular disease in patients with type 2 diabetes and chronic kidney disease. Key secondary endpoints include the annual rate of change in eGFR1, major adverse cardiovascular events (non-fatal myocardial infarction, non-fatal stroke, cardiovascular death), and all-cause mortality risk. The trial protocol specifies an interim analysis when a pre-specified number of primary endpoints are reached.
So why, if a predetermined standard is reached, does a clinical trial need to be stopped?The reason is that during the clinical trial phase, clinical equipoise must be maintained while ensuring patients receive appropriate treatment. Clinical equipoise means that researchers need to keep the potential benefits or risks roughly equal for participants in random group assignments. In most clinical trials, an independent data monitoring committee is entrusted to conduct real-time analysis of the trial. If the interim analysis shows the expected efficacy difference — for instance, if the intervention in the experimental group is observed to be significantly better than the control group — the trial can be terminated early. At this point, the clinical equipoise involved in the comparative therapy has been broken by the existing data. Continuing the trial would obviously be unfair to patients assigned to the less effective group.
The FLOW study is the first GLP-1RA clinical trial to use renal outcomes as the primary endpoint, and its results may have a significant impact on the future treatment of patients with T2DM and CKD.
Exploration of GLP-1RA in the Treatment of Chronic Kidney Disease
Diabetes has become a serious global public health issue, with the number of people affected expected to rise to 700 million by 2045. Persistent high blood glucose levels can lead to systemic vascular damage, affecting the heart, eyes, kidneys, and nerves, and result in various complications. Among these, chronic kidney disease (CKD) is a severe comorbidity of diabetes. CKD is a clinical syndrome characterized by persistent abnormalities in kidney structure and/or function, with a global incidence rate of 8%-16%. Over 40% of diabetes patients may progress to CKD, most of whom are in the early stages (CKD stages 1-2). Some patients will advance to end-stage renal disease requiring dialysis and/or transplantation. Age-stratified analysis shows that the prevalence of CKD among T2DM patients aged ≥65 years is as high as 58.7%, with more advanced stages.Type 2 diabetes is often associated with CKD, which has become one of the leading causes of death among diabetic patients in China.
Figure 3. Stages of CKD Progression
Currently, there is no comprehensive clinical polypharmacy safety guideline for T2DM patients with CKD both in China and internationally. The guidelines that have been issued only consider a single comorbidity, offering limited specific recommendations on managing patients with multiple coexisting conditions. At present, a comprehensive treatment strategy is widely adopted for diabetic patients with CKD, specifically including therapies aimed at reducing serum uric acid levels, lowering blood pressure and lipids, and other treatments used individually or in combination. Among these, glycemic control is the most critical for T2DM patients with CKD. Achieving glycemic targets can alleviate the progression of proteinuria and reduce the proportion of patients progressing to CKD stage 3. Moreover, for patients with substantial proteinuria, it may reverse their condition to microalbuminuria or normal albuminuria.Certain hypoglycemic drugs also have a direct effect on the kidneys, meaning their therapeutic efficacy is not mediated by blood glucose levels. For example, glucagon-like peptide-1 receptor agonists (GLP-1 RA) have been shown in multiple clinical studies to directly impact the kidneys, improving renal outcomes compared to placebo.
The GLP-1RA drug Semaglutide, which had its trial prematurely terminated this time, had already demonstrated therapeutic effects on CKD in previous series of clinical trials.
Post-hoc analysis of the SUSTAIN 1-7 studies found that, compared with placebo treatment, Semaglutide treatment continuously reduced the level of proteinuria in T2DM patients. This effect was observed as early as 16 weeks after treatment and persisted throughout the study period, with the most significant reduction (approximately 50%) observed in patients with both microalbuminuria and macroalbuminuria. Analysis of secondary renal endpoints from a series of clinical trials showed that Semaglutide effectively delayed the onset and progression of diabetic kidney disease in T2DM patients with high cardiovascular risk. It significantly reduced the incidence of new persistent macroalbuminuria or worsening kidney disease and decreased the risk of composite renal endpoint events by 36%, effectively lowering the incidence or progression rate of new kidney disease in T2DM patients.
In the SUSTAIN 6 study, although Semaglutide demonstrated renal protective effects, its primary endpoint was cardiovascular outcomes, not specifically renal outcomes.Therefore, there is almost no research on its efficacy and safety in T2DM patients with CKD. A subsequent multicenter, retrospective, observational real-world study conducted in Spain on the use of Semaglutide in T2DM patients with CKD showed that after 12 months of subcutaneous injection of Semaglutide, in addition to significant improvements in blood glucose, blood pressure, and body weight, patients with a urinary albumin/creatinine ratio >300 mg/g experienced a reduction in urinary albumin levels by more than 50%. This indicates that the use of Semaglutide in T2DM patients with CKD is safe and well-tolerated.The premature halt of the FLOW clinical trial due to efficacy surpassing expectations further validates the efficacy and safety of Semaglutide in treating T2DM with CKD.
In the GLP-1RA therapy for T2DM combined with CKD, Semaglutide's competitor, Lilly, is also actively exploring the indications for CKD.In the REWIND randomized controlled trial for Dulaglutide, compared with placebo, Dulaglutide reduced the risk of renal composite endpoint events by 15% in T2DM patients with a history of cardiovascular events or cardiovascular risk factors. The risk of new-onset macroalbuminuria was reduced by 23%, and the risk of sustained eGFR decline ≥30% was reduced by 11%. However, no significant reduction in the risk of chronic kidney replacement therapy was observed. On February 8, 2023, Lilly recruited 140 obese patients with T2DM and CKD in six countries and regions to participate in a clinical trial (Clinical Trial Identifier: NCT05536804). The aim is to study the efficacy and safety of Lilly's leading product Tirzepatide in treating obese patients with T2DM and CKD. The trial will last for 52 weeks and is expected to be completed on February 26, 2026.
Walking Further on the Path of Expanding Indications
Lowering blood sugar and reducing weight are basic operations.
Basic indications are the moat for Semaglutide to establish its market-leading position.
In the field of diabetes indications,Semaglutide is available in the subcutaneous injection formulation Ozempic and the oral formulation Rybelsus for glucose reduction, which were approved by the FDA for market release in 2017 and 2019, respectively. Ozempic, having been launched earlier and being a long-acting formulation that allows for once-weekly injections, has achieved higher sales compared to the daily oral formulation Rybelsus.
The SUSTAIN series is a large-scale Phase III clinical trial for Semaglutide. The glucose-lowering efficacy of Semaglutide is significantly superior to that of placebo and any comparator drugs, truly standing out as the best. In the SUSTAIN 5 and SUSTAIN 7 studies, Semaglutide 1.0 mg demonstrated an HbA1c reduction of up to 1.8%.
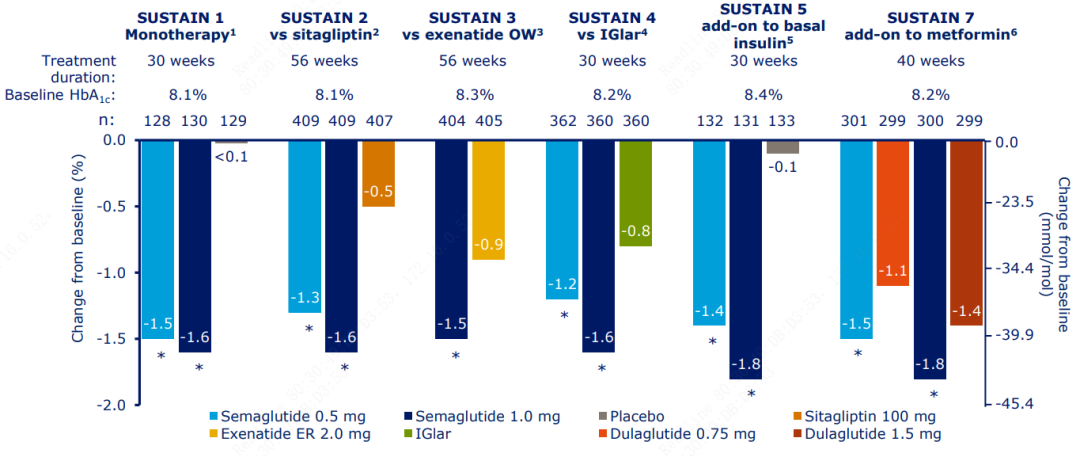
Figure 4. SUSTAIN Series Data
In the field of weight loss indications,On June 4, 2021, the FDA approved Wegovy as an adjunct to diet and exercise for the treatment of obesity. In the SUSTAIN clinical trial, Semaglutide 1.0mg achieved a weight loss of 6.4kg in 30 weeks.
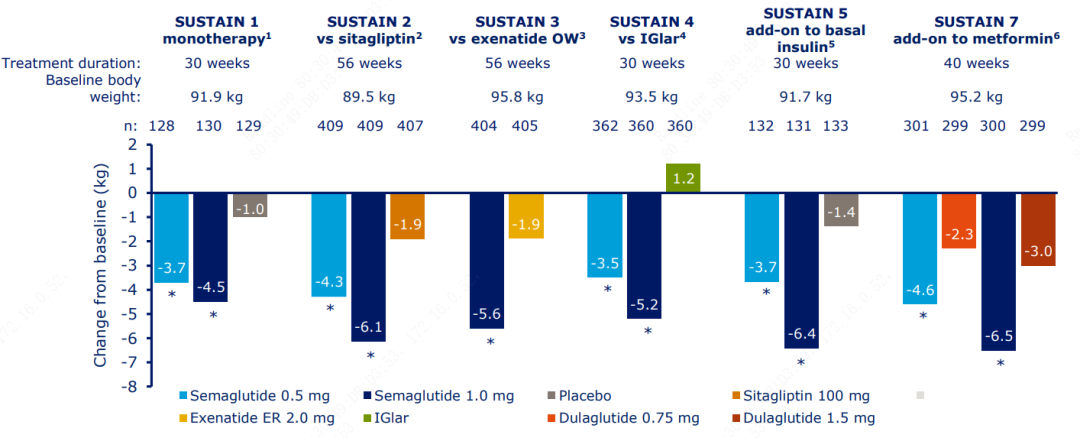
Figure 5. SUSTAIN Series Data
In 2023H1, Novo Nordisk's Semaglutide ranked first on the peptide drug sales list with a significant lead. Its sales in 2023H1 reached $9021.7 Mn, increasing by 85% year-on-year. It is expected that the total sales for 2023 will exceed $20 Bn.The sales of injectable hypoglycemic version Ozempic, oral hypoglycemic version Rybelsus, and injectable weight-loss version Wegovy were DKK 41,741 Mn ($6057.6 Mn), DKK 8,344 Mn ($1210.9 Mn), and DKK 12,081 Mn ($1753.2 Mn), respectively.
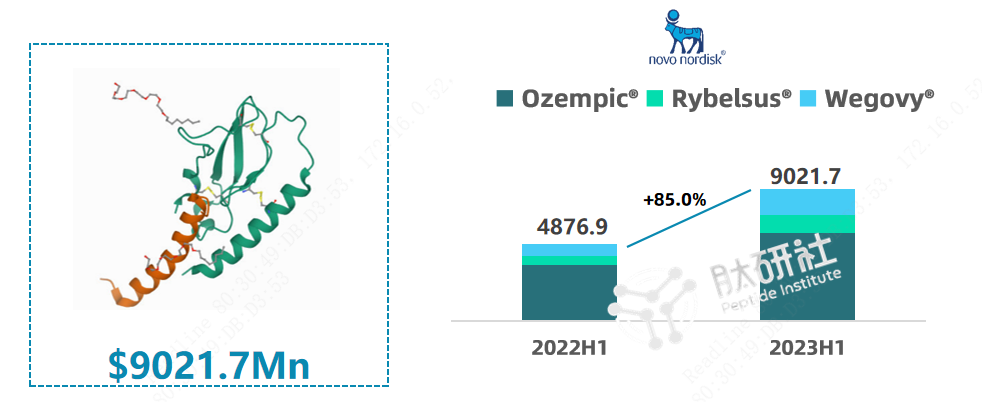
Figure 6. Semaglutide 2023H1 Sales Performance
Semaglutide has become Novo Nordisk's most powerful "cash cow." Led by the Semaglutide product series, Novo Nordisk's stock price has soared, and the company's market value has surpassed that of LVMH Group, the leading enterprise in the global luxury industry, making it the highest-valued company in all of Europe. Moreover, Semaglutide has faced a situation of supply falling short of demand for raw materials lasting up to a year, and related CDMO companies are continuously expanding their production capacity.
Continuous Expansion of Indications
Facing the strong entry of Lilly's Dulaglutide, Tirzepatide, Retatrutide, and Orforglipron — various GLP-1 RA drugs with dual and triple targets — Novo Nordisk's response is to continuously expand the indications of Semaglutide, further explore its potential in metabolic diseases, and build it into an unparalleled BIC product. This is the confidence that allows Novo Nordisk to remain steadfast and avoid being drawn into the multi-target drug arms race.
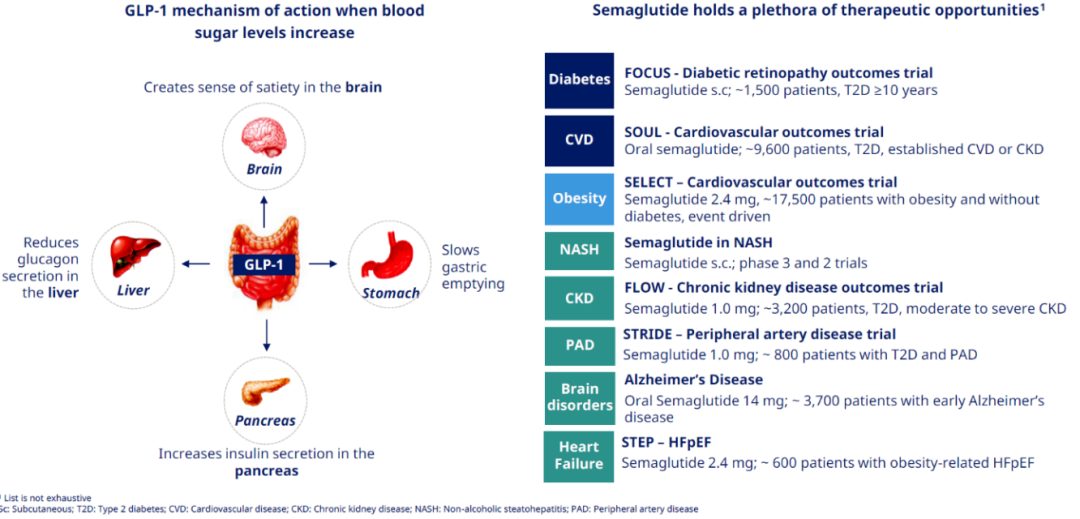
Figure 7. Possible Indications for Semaglutide
Continuously expanding the capability boundary, several key Phase III studies on Semaglutide are currently underway, covering not only CKD but also large-market indications such as heart failure with preserved ejection fraction (HFpEF), Alzheimer's disease (AD), diabetic retinopathy (DR), non-alcoholic steatohepatitis (NASH), and peripheral artery disease (PAD).
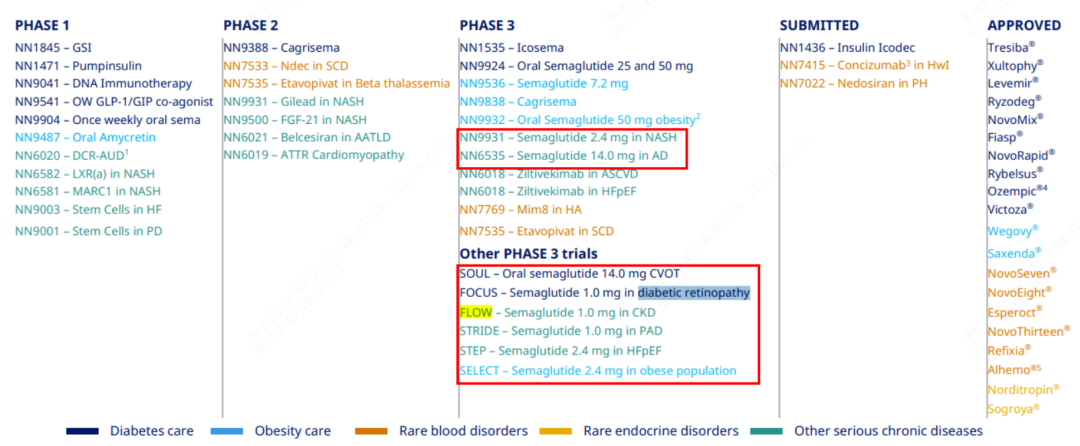
Figure 8. Semaglutide Pipeline for Other Indications
(1) Heart Failure with Preserved Ejection Fraction (HFpEF)
The prevalence of heart failure with preserved ejection fraction (HFpEF) is increasing yearly and is associated with a high symptom burden and functional impairment, particularly in obese patients. HFpEF accounts for half of all heart failure cases, imposing burdens such as fatigue, dyspnea, and limited physical capacity on patients. The majority (80%) of HFpEF patients are overweight or obese, which exacerbates symptoms and reduces quality of life.Currently, there is no treatment regimen specifically for obesity-related heart failure with preserved ejection fraction.
In recent years, the exploration of novel drugs that improve metabolism (such as GLP-1RA, GLP-1/GIP dual receptor agonists, SGLT-2i, and mitochondrial uncoupling modulators, etc.) in the HFpEF field has become a research hotspot, with multiple clinical studies of several drugs currently underway.
On January 16, 2020, the FDA approved the cardiovascular indication for Semaglutide based on the results of the SUSTAIN 6 Phase III clinical trial. Semaglutide is approved for use in patients with type 2 diabetes and established cardiovascular disease to reduce the risk of major adverse cardiovascular events.

Figure 9. Ozempic Instructions
A meta-analysis incorporating the populations from the LEADER, SUSTAIN 6, and PIONEER 6 studies further demonstrated the effect of GLP-1RA class drugs on MACE, suggesting that GLP-1RA can be used as primary or secondary prevention for cardiovascular and cerebrovascular diseases in patients with or without T2DM. In August 2023, the results of the SELECT Phase III clinical trial were announced, showing that a once-weekly subcutaneous injection of 2.4 mg semaglutide reduced the risk of major adverse cardiovascular events by 20% in overweight or obese adults (patients had no history of diabetes). Studies have shown that the cardioprotective effects of semaglutide may be mediated by weight loss, reduced hepatic insulin resistance, improved insulin sensitivity, alleviation of systemic inflammation, lowered blood pressure and lipid levels, and direct effects of GLP-1 receptors on the heart and vascular system.
In the LEADER, SUSTAIN 6, and PIONEER 6 series of clinical data, Semaglutide has demonstrated cardiovascular benefits. In 2021, Novo Nordisk initiated the Phase 3 clinical trial for the HFpEF indication, STEP HFpEF. Between March 16, 2021, and April 18, 2023, a randomized, double-blind, placebo-controlled trial was conducted across 96 sites in 13 countries in Asia, Europe, North America, and South America, recruiting a total of 529 HFpEF patients with BMI ≥30. Participants received either once-weekly Semaglutide (2.4 mg) or a placebo over 52 weeks. The STEP HFpEF trial required enrolled patients to have LVEF >45% and BMI >30%.
Data released by Novo Nordisk on 2023-8-25 showed that the mean change in KCCQ-CSS for the treatment group was 16.6 points, with an average percentage change in body weight of -13.3%, while the mean change in KCCQ-CSS for the placebo group was 8.7 points and the body weight change was -2.6%. In the secondary endpoint analysis, the mean change in 6-minute walking distance was 21.5 meters for the Semaglutide group and 1.2 meters for the placebo group. In the hierarchical composite endpoint analysis, Semaglutide demonstrated clear superiority over placebo. The mean percentage change in CRP levels for the Semaglutide group was also significantly better than that of the placebo group (-43.5% vs. -7.3%).
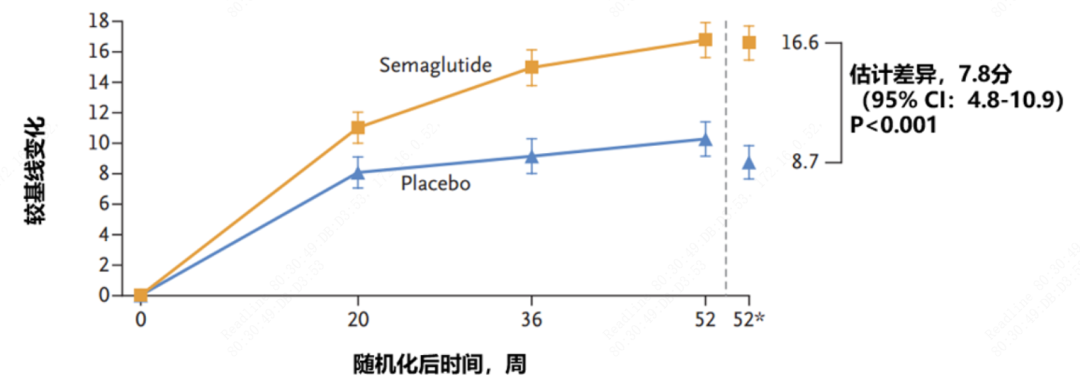
Figure 10. KCCQ-CSS Data
Compared with previous drugs applied to HFpEF (such as SGLT2 inhibitors, sacubitril-valsartan, and spironolactone), Semaglutide has demonstrated greater benefits through KCCQ scores.Weight loss and the accompanying reduction in visceral adipose tissue, favorable anti-inflammatory effects (indicated by decreased CRP levels), and hemodynamic benefits (suggested by reductions in systolic blood pressure and NT-proBNP levels) are likely key mechanisms behind the significant therapeutic benefits of Semaglutide observed in this patient group. Based on high-sensitivity C-reactive protein (hsCRP) testing, Semaglutide also shows potential for reducing inflammation.
(2) Alzheimer's Disease (AD)
The occurrence of AD is related to insulin resistance. Insulin resistance prevents cells from absorbing glucose normally under the guidance of hormones. When blood sugar levels are suboptimal, highly active neurons cannot obtain the energy they require. In this "starved" state, neuronal cells may become dysfunctional and eventually die. The most active neurons, which are those with the highest energy demands, are typically located in learning and memory regions, and their damage leads to neurodegenerative diseases.
Studies show that GLP-1 receptors located within the brain are also involved in cognitive function, synaptic transmission in hippocampal neurons, and apoptosis. Overexpression enhances cognitive abilities and provides neuroprotection, while their absence increases the likelihood of seizures and neurodegeneration. Research has demonstrated that GLP-1RA can directly modulate neurotransmitter release, improving cognitive impairment and neurological deficits associated with T2DM or obesity.Therefore, the GLP-1 receptor is considered a promising target for exploring drugs with better neuroprotective effects and cognitive enhancement capabilities. This also indicates the potential of GLP-1RA in treating neurodegenerative diseases such as AD and PD. In transgenic mouse models of AD, GLP-1RA can prevent the deposition of amyloid plaques, synaptic loss, and cognitive impairment.
In a post-hoc analysis of data from three large cardiovascular outcome trials conducted on Novo Nordisk (LEADER, SUSTAIN 6, and PIONEER 6), which included 15,820 patients with type 2 diabetes and had a median follow-up time of 3.6 years, a total of 47 cases of dementia were identified, with 32 in the placebo group and 15 in the GLP-1 (liraglutide or semaglutide) group. The results showed that the incidence of dementia was statistically significantly reduced by 53% in patients taking GLP-1.
To further confirm the efficacy and safety of Semaglutide in clinical practice, in 2021, Novo Nordisk initiated two Phase III trials.EVOKE and EVOKE Plus, to study the efficacy of Semaglutide in approximately 3,700 patients with early-stage Alzheimer's disease. The EVOKE trial is expected to be completed by September 2025.
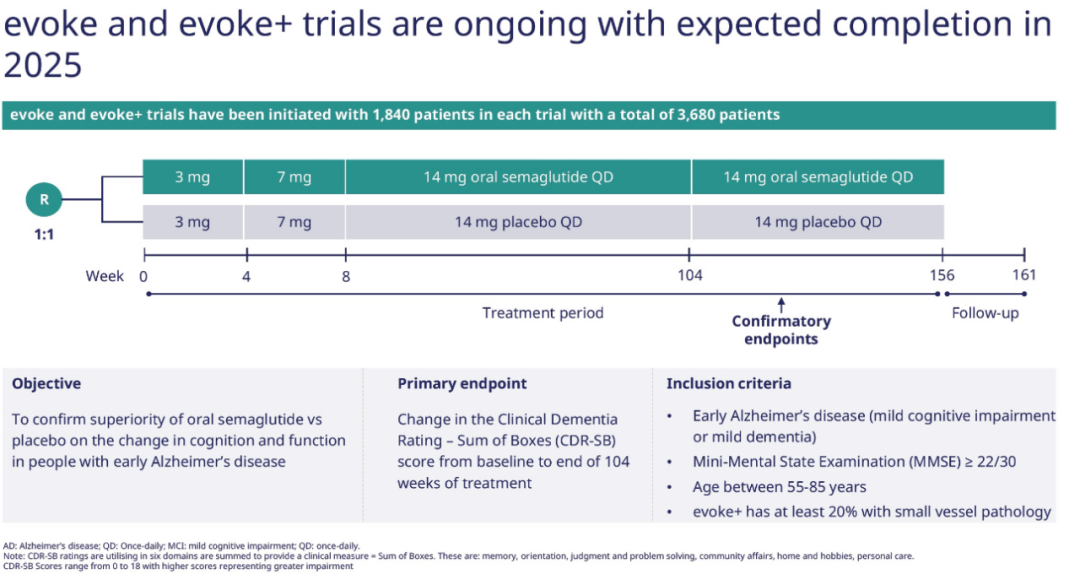
Figure 11. Evoke and Evoke+ Trial Design
(3) Diabetic Retinopathy (DR)
Diabetic Retinopathy (DR) is one of the common chronic complications of diabetes. The duration of diabetes and blood glucose levels are the main risk factors for the progression of DR. The main risk factors for DR include hyperglycemia or significant blood glucose fluctuations, hypertension, hyperlipidemia, long duration of diabetes, diabetic nephropathy, pregnancy, obesity, susceptibility genes, etc. Hyperglycemia is one of the important risk factors for DR or Diabetic Macular Edema (DME), and it is also a key modifiable risk factor.
GLP-1RA not only delays the progression of DR by lowering and stabilizing blood glucose, but also has other mechanisms of action. Some studies have shown that GLP-1RA can prevent the onset or slow the progression of DR through anti-apoptotic and anti-inflammatory mechanisms. GLP-1R agonists can prevent BRB breakdown, reduce the level of intercellular adhesion molecule-1 (ICAM-1) in the retina of Goto-Kakizaki (GK) rats, and decrease the expression of placental growth factor (PLGF) and vascular endothelial growth factor (VEGF), as well as the activation of protein kinase B (AKT) in vitro.
To verify the efficacy and safety of Semaglutide in treating DR, on 2019-5-8, Novo Nordisk initiated a trial named “FOCUS"Phase III clinical trial recruited 1,500 patients with diabetic retinopathy to study the long-term effects of Semaglutide versus placebo on DR. The study will last for 5 years and is expected to conclude on 2027-11-07."
(4) Nonalcoholic Steatohepatitis (NASH)
Non-alcoholic steatohepatitis (NASH), also known as metabolic steatohepatitis, is a severe form of non-alcoholic fatty liver disease (NAFLD). Approximately 15%-25% of NAFLD patients progress to NASH, and the incidence of cirrhosis in NASH patients is as high as 15%-25% within 10 to 15 years. More severe cases can lead to liver cancer. Tens of millions of people are affected, but so far, no drug specifically for NASH has been approved by the FDA or NMPA, and a significant amount of clinical treatment needs remain unmet.
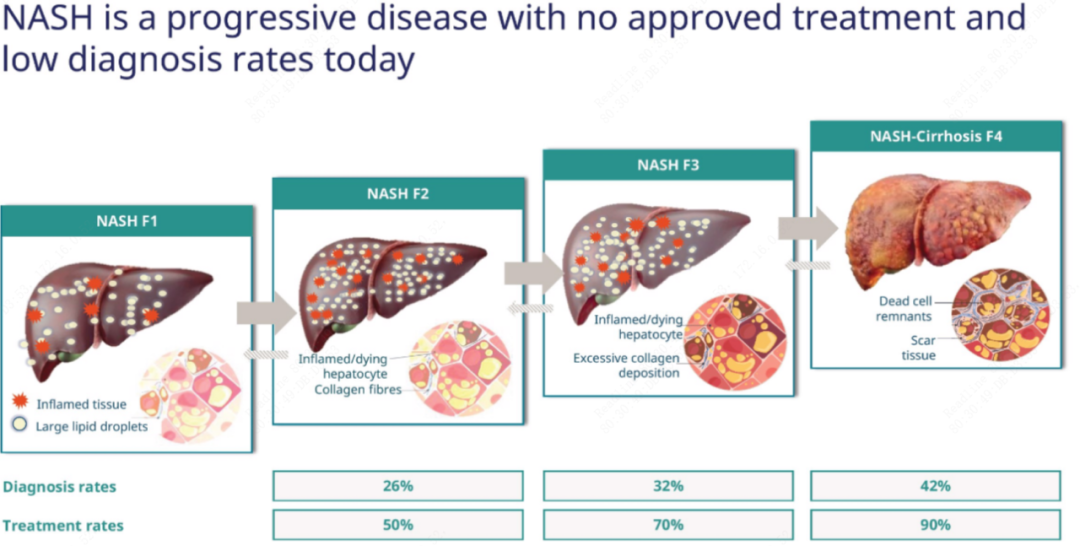
Figure 12. Development and Formation of NASH
GLP-1 can reduce inflammatory response and fibrosis in hepatocytes in nonalcoholic fatty liver disease (NAFLD), effectively delaying the progression of NAFLD; previous studies have found that GLP-1 secretion is impaired in patients with NASH, which has become the basis for the use of GLP-1RA in the management and treatment of NASH.GLP-1RA has demonstrated direct liver protective effects independent of insulin through the gut-pancreas-liver axis, stimulating hepatic lipogenesis, glucose uptake, reducing hepatic gluconeogenesis, and improving insulin resistance.In addition, GLP-1RA reduces hepatic steatosis and hepatocyte injury while demonstrating significant hepato-protective effects by improving hepatic mitochondrial function, insulin sensitivity, and suppressing the stress response of the damaged endoplasmic reticulum. It also decreases the accumulation of free fatty acids and reduces lipotoxicity by promoting autophagy.Studies show that various GLP-1RAs, such as liraglutide, dulaglutide, and semaglutide, can significantly improve NASH.
Semaglutide has been explored for the NASH indication. In the Phase II clinical trial, coded as NCT02970942, a Phase II clinical trial assessed the efficacy and safety of Semaglutide in treating 320 patients with biopsy-confirmed NAFLD over 72 weeks. The results showed that the percentage of patients achieving NASH resolution without fibrosis worsening after once-daily subcutaneous injection of Semaglutide was 40% in the 0.1 mg group, 36% in the 0.2 mg group, and 59% in the 0.4 mg group, compared to 17% in the placebo group. Additionally, 43% of patients in the 0.4 mg group and 33% in the placebo group showed improvement in fibrosis stage.
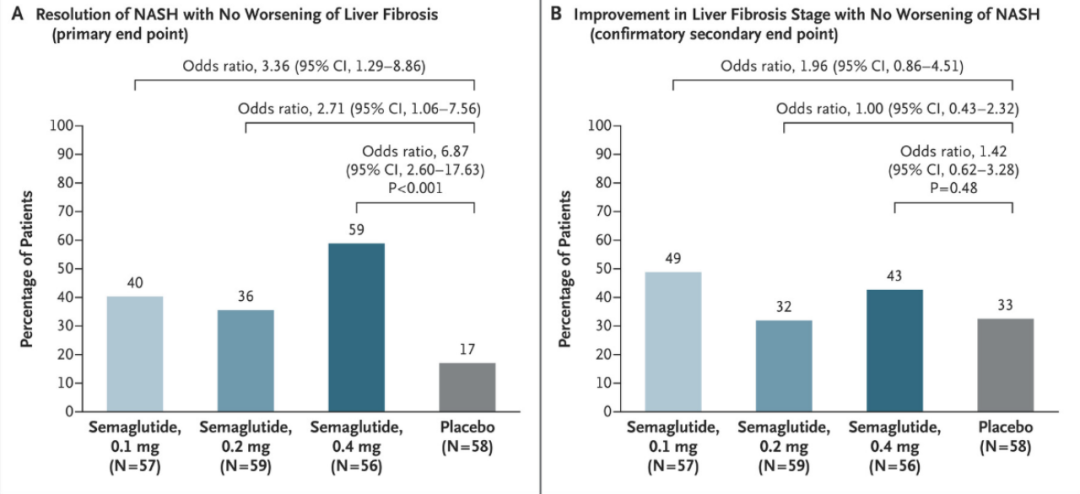
Figure 13. Results of the NCT02970942 Clinical Trial
A Phase IIIa Trial of Semaglutide 2.4mg for the Treatment of NASHESSENCE ClinicalInitiated in 2021 Q1, the trial recruited 1,200 patients to study the efficacy and safety of Semaglutide monotherapy in NASH patients without cirrhosis. It evaluates primary endpoints such as the progression of cirrhosis, the resolution of steatohepatitis, inflammation, and histological changes in ballooned hepatocytes. The trial is divided into two parts: Part 1 lasts for 72 weeks, and Part 2 lasts for 240 weeks. The submission of the marketing application for this indication is expected based on the results from Part 1 and Phase 2 clinical trials.
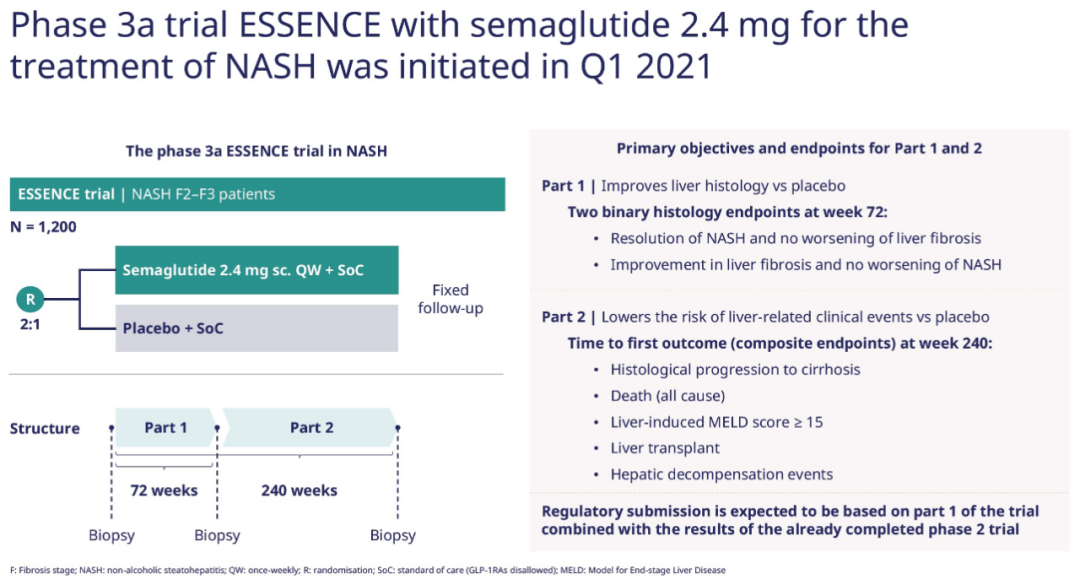
Figure 14. Design of Phase IIIa ESSENCE Trial
(5) Peripheral Artery Disease (PAD)
Approximately 6% of adults worldwide suffer from peripheral artery disease (PAD), with its prevalence on the rise. The main characteristics of PAD include narrowing or occlusion of the arteries in the lower limbs, leading to a decline in quality of life, leg pain, restricted mobility, tissue damage, and an increased risk of major adverse events such as myocardial infarction, stroke, revascularization, amputation, and death. PAD results in functional limitations for patients (e.g., reduced walking distance in the 6-minute walk test [6MWT], decreased scores on the Short Physical Performance Battery), and a decline in health-related quality of life. Shorter 6MWT distances and poorer health-related quality of life are associated with a higher likelihood of disease progression. PAD has been identified as a significant risk factor for loss of mobility.
PAD patients have a high risk of major adverse cardiovascular events (MACE) and mortality. CLTI, poor health-related quality of life, or multiple severe comorbidities are risk factors for MACE and limb events.
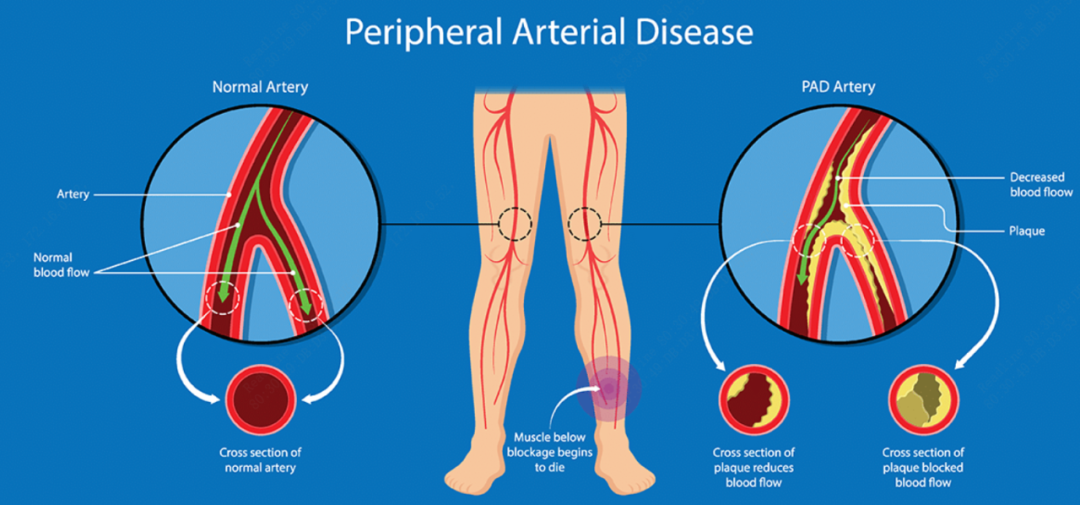
Figure 15. Schematic diagram of PAD etiology
Novo Nordisk Explores the Possibility of Treating PAD from the Semaglutide Series Clinical Data. The results of the cardiovascular (CV) outcome studies LEADER and SUSTAIN 6 indicate that liraglutide and semaglutide can reduce the risk of cardiovascular events in patients with T2DM and high cardiovascular risk. This post-hoc analysis evaluated the impact of liraglutide and semaglutide on cardiovascular outcomes in patients with peripheral artery disease (PAD) at baseline. In the LEADER and SUSTAIN 6 studies, 12.5% (n=1167/9340) and 13.7% (n=453/3297) of patients, respectively, had PAD at baseline. Patients with a history of PAD had a longer duration of diabetes compared to those without PAD. Other baseline characteristics were similar between the PAD and non-PAD subgroups and comparable across different treatment groups. In both studies, regardless of the treatment received, PAD patients had a higher risk of MACE (LEADER: HR 1.35; 95% CI: 1.17-1.57; SUSTAIN 6: HR 1.31; 95% CI: 0.93-1.81) and extended MACE (LEADER: HR 1.27; 95% CI: 1.12-1.44; SUSTAIN 6: HR 1.72; 95% CI: 1.36-2.15) compared to patients without PAD. Both liraglutide and semaglutide reduced cardiovascular risk compared to placebo, regardless of whether PAD was present or absent at baseline.
Therefore, in T2DM patients, a history of PAD is associated with an increased risk of MACE. The GLP-1 analogs liraglutide and semaglutide reduce the risk of cardiovascular events in patients with or without PAD.
Novo Nordisk submitted an application named “STRIDEThe Phase III clinical trial recruited 800 patients with peripheral artery disease (PAD) and type 2 diabetes whose walking ability was affected, aiming to evaluate the impact of Semaglutide treatment on walking ability in these patients. The primary endpoint is the ratio of the change in maximum walking distance from baseline during a constant-load treadmill test. Secondary endpoints include the subsequent change in maximum walking distance from baseline during a constant-load treadmill test, changes in Vascular Quality of Life Questionnaire-6 (VascuQoL-6) scores, and changes in pain-free walking distance during the constant-load treadmill test, among others.
Conclusion
Semaglutide, as a novel long-acting GLP-1RA, not only shows significant effects in lowering blood sugar and reducing weight but also provides cardiovascular protection in multiple aspects, including safeguarding vascular endothelium, reducing blood pressure, improving lipid profiles, alleviating inflammation, and enhancing microcirculation, with good tolerability.
In recent years, Semaglutide has gained immense popularity in the market. However, faced with increasing competition in the GLP-1 market, Novo Nordisk is continuously exploring and expanding the boundaries of Semaglutide's indications. Multiple clinical trials for various indications such as NASH, AD, HFpEF, DR, and PAD have been initiated, aiming to develop BIC products for each indication.
Semaglutide Fully Displays Its "Wonder Drug" Potential. When we thought the oral formulation was the trump card, Novo Nordisk unveiled cardiovascular benefits from an ultra-large clinical trial involving 17,000 participants; as the echoes of cardiovascular benefit evidence lingered, Novo Nordisk moved on to secure heart failure, preparing to capture the SGLT-2 market; while people were still reveling in the impressive efficacy for heart failure, Novo Nordisk announced the early completion of a clinical trial for T2DM with CKD. Semaglutide currently has over 300 trials underway globally, and as these trials progress, semaglutide is expected to bring more surprises. Both academia and industry are watching with bated breath.
[1] PharmaTimes: Seven years ago, liraglutide failed miserably in two heart failure trials against placebo; now semaglutide has succeeded...
[2] Chinese Journal of Diabetes: Advances in the Clinical Application of Semaglutide
[3] PharmaDJ: Not Just for Weight Loss and Diabetes! The Next Indication for GLP-1 Peptides: Alzheimer's Disease
[4] Novo Nordisk Official Website
[5] Peptide Research Society: Heavyweight | 2023H1 Global Peptide Drug Sales List
- END -

Flagship Report
Column Recommendation




Peptide Research Society
In-depth Research Report on Medical Health
"Strategy Team Organization" New Consulting