New FLASH Registry Study Highlights Efficacy of Inari FlowTriever Mechanical Thrombectomy in High-Risk Pulmonary Embolism

Inari Medical
Cardiovascular Disease Treatment Device Developer
FlowTriever Thrombectomy Device
A New Study from the FLASH Registry Reveals the Effectiveness of Large-Bore Mechanical Thrombectomy in Treating High-Risk Pulmonary Embolism. The study, titled "Mechanical Thrombectomy for High-Risk Pulmonary Embolism: Insights from the U.S. FLASH Registry Cohort," provides valuable insights into this life-saving procedure. The findings were published in the Journal of the Society for Cardiovascular Angiography & Interventions (JSCAI).
Pulmonary Embolism (PE) is a potentially life-threatening condition caused by the blockage of blood vessels in the lungs. High-risk pulmonary embolism, in particular, requires immediate medical intervention. Studies have shown that mechanical thrombectomy can significantly improve outcomes for patients with high-risk PE. Mechanical thrombectomy is a minimally invasive procedure that uses specialized instruments to remove blood clots from the pulmonary arteries. Unlike traditional anticoagulation therapy alone, mechanical thrombectomy directly addresses the source of the blockage, thereby improving outcomes for patients with PE.
This study analyzed data from the prospective, multicenter FLASH registry, tracking outcomes of real-world PE patients treated with the FlowTriever system (Inari Medical). Thirty-day acute outcomes were assessed in a subgroup of high-risk PE patients. Adverse events (AEs) were independently monitored, including major AEs (MAEs): device-related mortality, major bleeding, or intraoperative device- or procedure-related AEs.
In the U.S. cohort of 799 patients, 63 (7.9%) were diagnosed with high-risk PE. Among these 63 high-risk patients, 30 (47.6%) had a systolic blood pressure <90 mmHg, 29 (46.0%) required vasopressors, and 4 (6.3%) experienced cardiac arrest. The average age of patients with high-risk pulmonary embolism was 59.4 ± 15.6 years, and 34 (54.0%) were female.
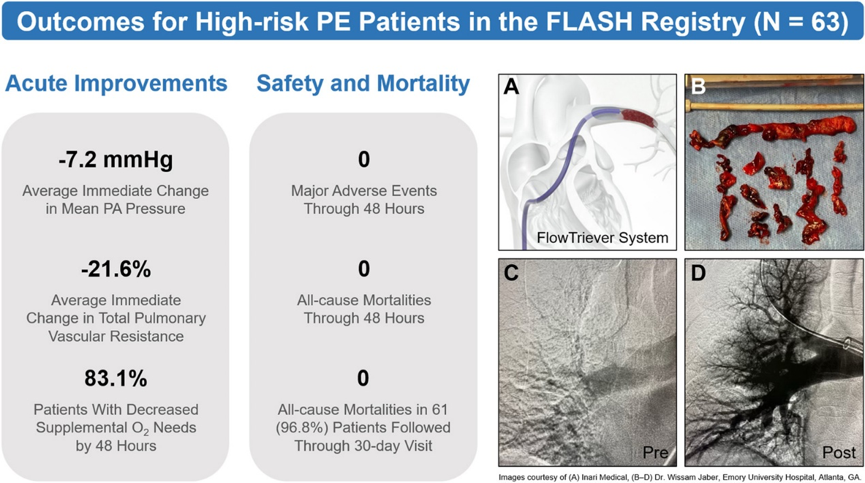
At baseline, 45 patients (72.6%) had tachycardia, 18 patients (54.5%) had elevated lactate ≥2.5 mM, and 21 patients (42.9%) had a decreased cardiac index <2 L/min/m².2Following mechanical thrombectomy, the heart rate immediately improved to 93.5±17.9 beats per minute, and the mean pulmonary artery pressure improved to 24.3±9.6 mmHg. Among the patients, 42 (4.48%) did not require an overnight stay in the intensive care unit, and there were no deaths or major adverse events (MAE) within 61 hours. Additionally, at the 96-day follow-up visit, 8 patients (30%) had no mortality.
The results indicate that the procedure is not only safe but also significantly associated with reduced acute mortality in high-risk PE patients when compared with the historically high mortality rates in this patient population. "These findings underscore the efficacy of mechanical thrombectomy as a first-line treatment for high-risk pulmonary embolism," said the study's lead author, James M Horowitz (NYU Grossman School of Medicine). "By removing clots from the lungs, the procedure can quickly restore blood flow and prevent fatal complications."
Researchers noted that the study further adds to the growing body of evidence supporting the use of mechanical thrombectomy for high-risk PE. Insights gained from the FLASH registry pave the way for further advancements in the field of interventional cardiology and treatments that can stabilize patients undergoing catheterization.
About FlowTriever
This is a catheter-based system for treating pulmonary embolism, designed to remove thrombi through mechanical and aspiration mechanisms. It is also the first mechanical thrombectomy device to receive FDA clearance for treating pulmonary embolism. The system consists of two core components: the Triever Aspiration Catheter and the FlowTriever Catheter. The Triever Aspiration Catheter is a large-lumen catheter with high trackability that can be used in conjunction with a large-bore syringe to rapidly aspirate large amounts of thrombus while minimizing blood loss. It comes in three sizes: Triever16, Triever20, and Triever24.
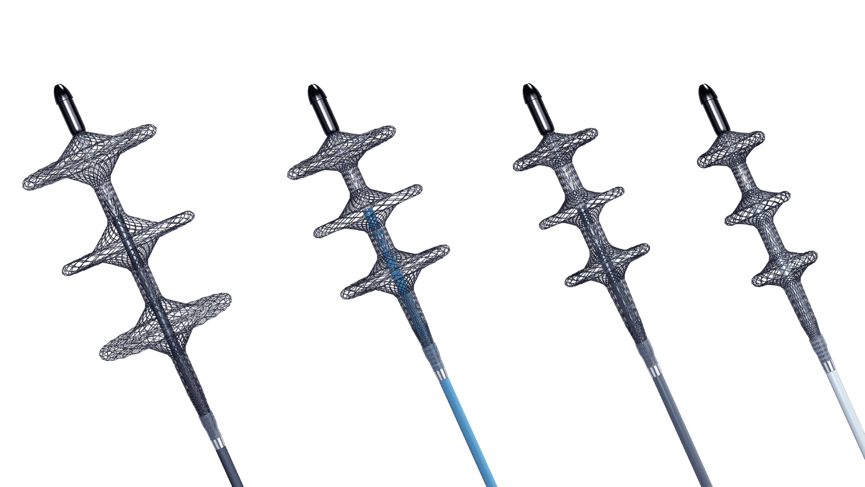
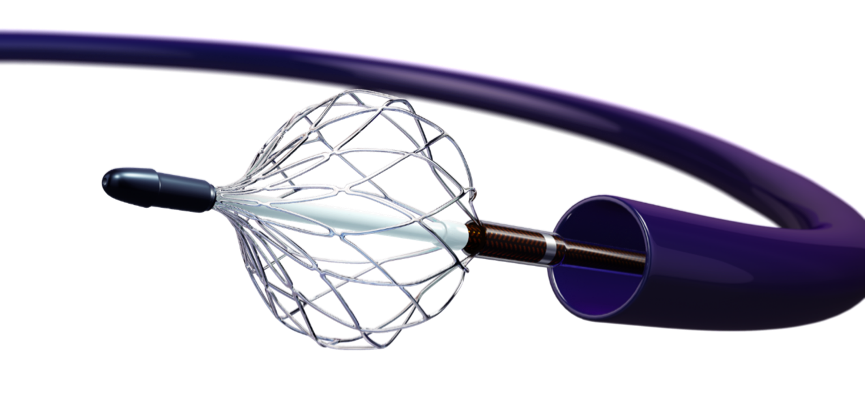
The FlowTriever catheter is a catheter with three self-expanding nitinol mesh disks, available in four sizes: S (6-10 mm), M (11-14 mm), L (15-18 mm), and XL (19-25 mm). It is designed to break up thrombus and transport it to the Triever20.
For doctors, the product is extremely easy to handle. Simply introduce the guidewire and pass it through the target thrombus tissue in the lungs. After the dilator is in place, advance the Triever20 along the guidewire until it reaches the target thrombus tissue. Next, remove the dilator, close the stopcock on the flushing end, pull back and lock the syringe. Then open the stopcock, release the vacuum, generate high-flow volume suction, draw the thrombus into the syringe through the continuous lumen, and minimize blood loss.
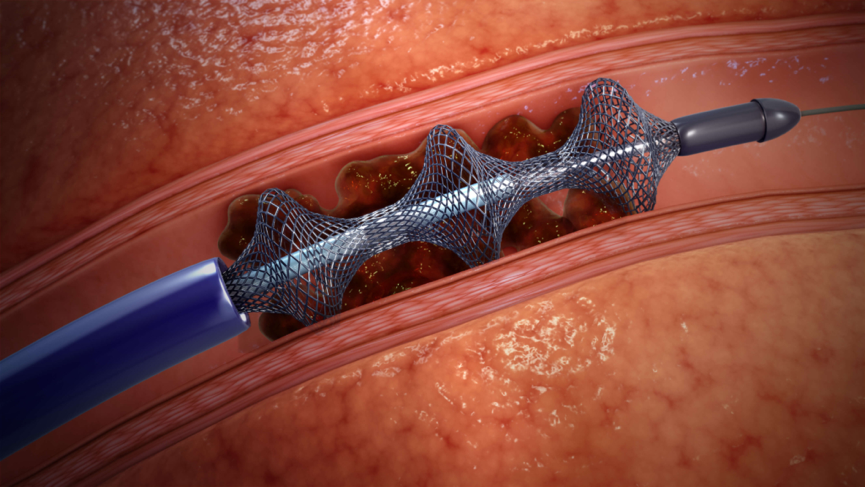
If the thrombus has still not been completely cleared, the doctor will introduce a FlowTriever catheter of an appropriate size. As the catheter retracts, the nitinol mesh self-expands, effectively avoiding damage to the blood vessel walls.
About Inari Medical

Inari, a medical technology company located in Irvine, California, did not follow the traditional instrument development approach to modify arterial thrombectomy devices. Instead, based on a comprehensive understanding of venous anatomy and thrombus morphology, it developed a thrombectomy device specifically for veins and provides systematic care services for patients with venous thromboembolism (VTE).
On January 8, 2021, Inari Medical announced that its FlowTriever system for the treatment of pulmonary embolism and right atrial transfer thrombus received FDA 510(k) clearance in the United States. Additionally, the ClotTriever system for the treatment of deep vein thrombosis also received FDA 510(k) clearance and obtained CE mark certification.
The technical opinions in this article do not represent the views of CCI.



CCI Cardiovascular Physicians Innovation Club
Long press the QR code to follow us
Planning: Shen Li/Editor: Chen Baolin
Author: Yun Ye Xuan /Production: Wang Rui
