Pfizer Pivots to Once-Daily Oral GLP-1 Agonist Danuglipron Amid Safety Concerns with Twice-Daily Regimen

Pfizer
Pharmaceutical R&D Developer
Breaking News
"Danzuglipron has a high degree of structural similarity to Lotiglipron, and it is possible that Danuglipron may encounter similar safety issues in Phase III clinical trials as those seen with Lotiglipron." The Peptide Research Society team stated in 'Breaking News | Pfizer Terminates Lotiglipron, What's the Impact on the Small Molecule GLP-1RA Landscape?》In the article, it was written.
Sure enough, after half a year, Pfizer hit the pause button on Danuglipron.On December 1, 2023, Pfizer announced the preliminary results of the Phase IIb clinical trial of the oral GLP-1 agonist Danuglipron (PF-06882961) for the treatment of adult obesity.Halt the Phase III clinical trial of the twice-daily formulation of this drug and instead advance the optimization of the once-daily Danuglipron formulation and conduct pharmacokinetic studies.
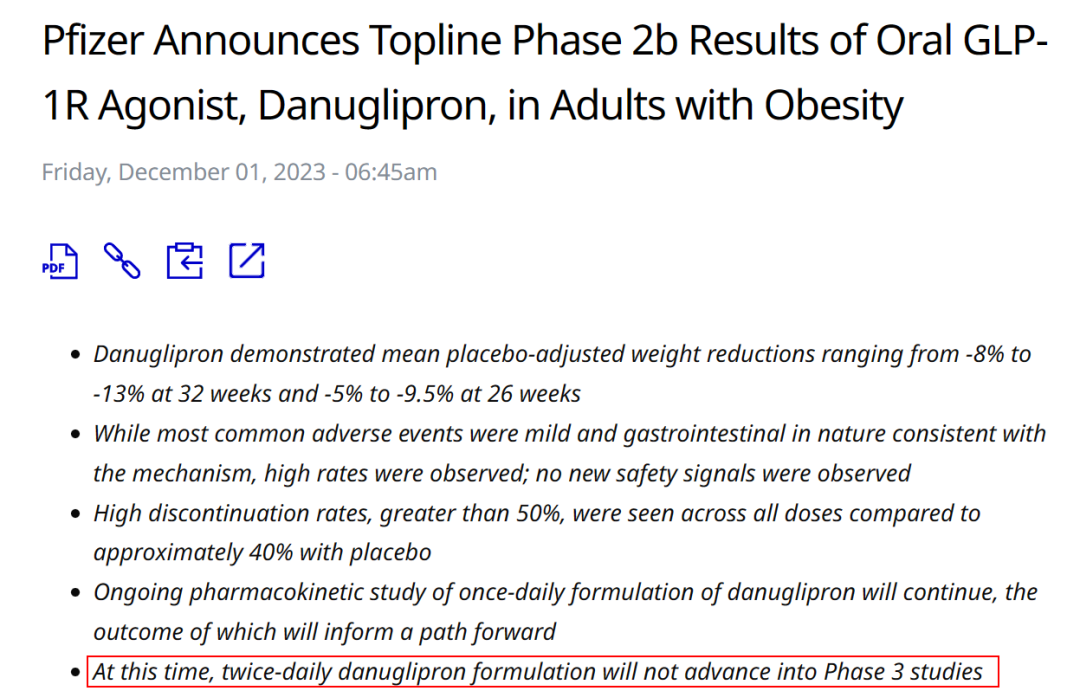
Figure 1. Pfizer Issues Termination Announcement
The Tragedy of Pfizer's Oral Small Molecule
Danuglipron is an oral small-molecule agonist originally developed by Pfizer. The research and development team screened and optimized it from 2.8 million compounds based on high-throughput assays. It has a half-life of 4.3-5.7 hours and is taken orally twice daily.
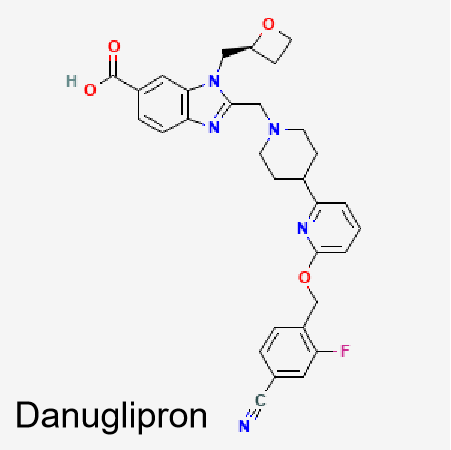
Figure 2. Structure of Danuglipron
In terms of efficacy results, the data for Danuglipron twice daily shows itsIndeed, it is close to the injectable version of Semaglutide and the oral small molecule agonist Orforglipron:The maximum weight loss was 11.7% within 32 weeks; after placebo adjustment, the maximum weight loss rate of Danuglipron at 32 weeks was -13.1%, and the maximum average weight loss rate at 26 weeks was -9.5%.
Compared with the injectable version of GLP-1 drugs, the placebo-adjusted weight loss is close to the 68-week data of injectable Semaglutide but falls short of the 72-week clinical data of the dual-target agonist Tirzepatide. Compared with oral GLP-1 drugs, the placebo-adjusted weight loss of Danuglipron is on par with the 36-week data of Lilly's oral small molecule agonist Orforglipron, but both far exceed the 62-week data of oral Semaglutide.
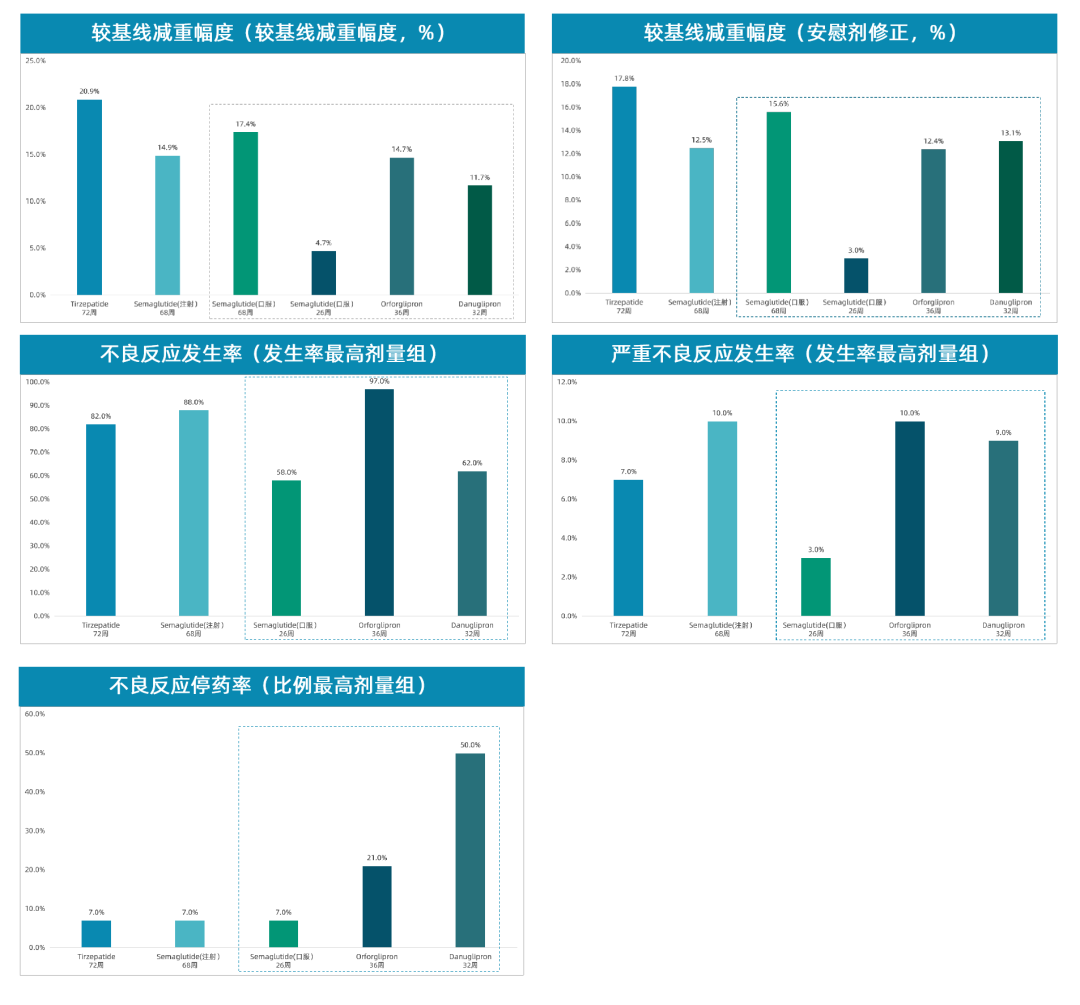
Figure 3. Horizontal comparison of clinical data for GLP-1 drugs
In Phase Ⅱb clinical trials, 73% of patients experienced nausea, up to 47% experienced vomiting, and up to 25% experienced diarrhea. The discontinuation rate was high across all doses. At first glance, the AE (Adverse Events) and SAE (Serious Adverse Events) of Danuglipron appear comparable to many GLP-1 drugs, which is a common issue among GLP-1 drugs, but generally improves over time with continued use.But the discontinuation rate of Danuglipron is indeed shocking, with over 50% indicating significant side effects that could not be alleviated in later stages. This became the major reason for Pfizer halting the Phase III advancement. Moreover, the placebo group’s discontinuation rate exceeding 40% raises suspicions of whether any incidents occurred.
From this perspective, safety issues seem to have become a common problem for orally administered small molecules.GLP-1 Oral Small Molecule Drugs in the Mid-to-Late Pipeline Include Pfizer's Lotiglipron, Danuglipron, and Lilly's Orforglipron. The Clinical Safety Data for All Three Are Actually Not Very Good, with High Discontinuation Rates. Orforglipron’s Discontinuation Rate Also Exceeds 20%, and Its Safety Is Inferior to Injectable GLP-1 and Oral Semaglutide.
In fact, if the effect of oral small-molecule agonists is slightly inferior to the injectable version, but can solve the problem of injection fear through daily oral administration, it can improve patient compliance to a certain extent. However, if oral administration brings safety issues, it is really not as good as getting an injection once a week.
In the announcement, Pfizer did not directly abandon this new drug but instead turned to research a once-daily modified-release formulation of Danuglipron. Future research results will guide improvements in tolerability and optimize study design. Danuglipron is a potent drug, and if patient tolerability can be improved through formulation adjustments, it is believed that it will also have a certain market in the future.The only problem is time. With the Phase I clinical trial just starting now, the future market competition will only become more intense, and the window of opportunity for Pfizer is already limited.
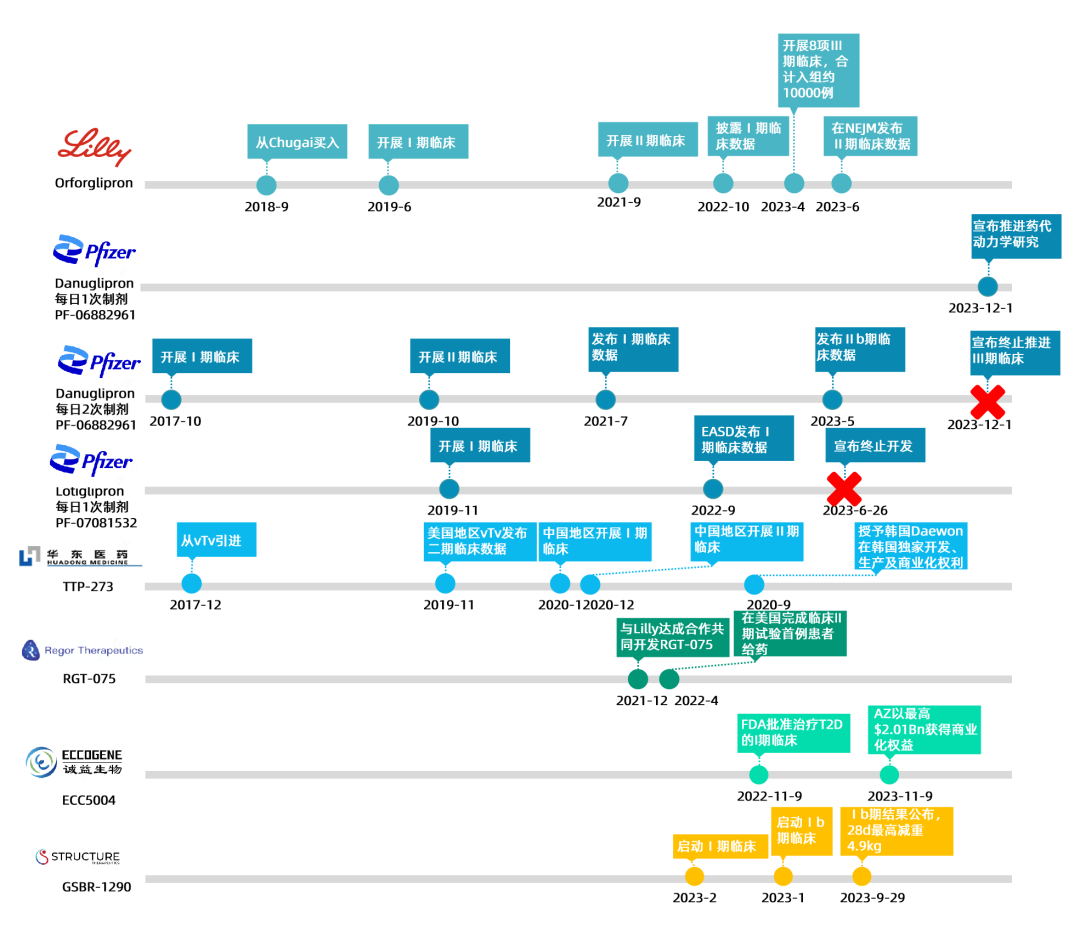
Figure 4. Progress in the Development of Oral Small Molecule GLP-1 Drugs
A review of the development progress of oral small molecules for GLP-1 reveals Pfizer's "pain" — the earliest to develop, the earliest to end, and repeated failures.
Danuglipron and Lotiglipron are a pair of tough brothers.In October 2017, Pfizer took the lead in advancing Danuglipron into Phase I clinical trials, becoming the first company to develop an oral small-molecule GLP-1 agonist. In November 2019, Lotiglipron, screened by its partner Sosei Heptare, also entered Phase I clinical trials. After three years, Phase I data was released in September 2022, and one year later, the pipeline was discontinued due to issues such as drug interactions and elevated transaminase levels. In the Phase IIb clinical trial results published in May 2023, the discontinuation rate in the 120mg group reached 34%, foreshadowing the eventual pipeline termination.
At this point, the originally dual-power competing oral small-molecule mid-to-late stage pipeline now has only Lilly's Orforglipron in the lead.A 15% weight loss at 32 weeks is impressive. If Phase III clinical trials can better verify safety issues, it has the potential to become the first oral small-molecule GLP-1 weight loss drug to reach the market. Joon Lee, a pharmaceutical analyst at Truist Securities, stated: "Lilly's Orforglipron appears to have the best overall performance. Although it may still be years away from commercialization, it could give Lilly a lead over Novo Nordisk in the development of small-molecule oral weight loss drugs."
Of course, besides the once-daily Danuglipron, Pfizer could also abandon its in-house project and instead achieve a leapfrog advance through acquisitions.After all, Orforglipron was also acquired by Lilly from Chugai, a subsidiary of Roche; similarly, AstraZeneca (AZ), which has faced consecutive failures in GLP-1, has also chosen the route of licensing-in. Eventually, it reached an exclusive $2.01 billion collaboration with China's Biotech company Eternity Bioscience on the oral small-molecule GLP-1 drug ECC5004. However, regardless of the approach, the precondition for approval is to significantly enhance safety in order to create value space.
The Difficulty in Developing Oral Weight-Loss Drugs
Compared with injectables, oral medications have natural advantages, offering more convenient administration and higher patient compliance, especially for patients with needle phobia.

Figure 5. Rybelsus developed by Novo Nordisk
Oral peptide weight-loss drugs inherently possess an extremely high development threshold. Peptide drugs exhibit poor permeability and are prone to degradation by proteases in the gastrointestinal tract. For peptide molecules to be successfully absorbed from the gastrointestinal tract into systemic circulation, they must pass through intestinal epithelial cells while avoiding degradation, and then be delivered to the lymphatic system or bloodstream. This process requires circumventing various structural and functional barriers.
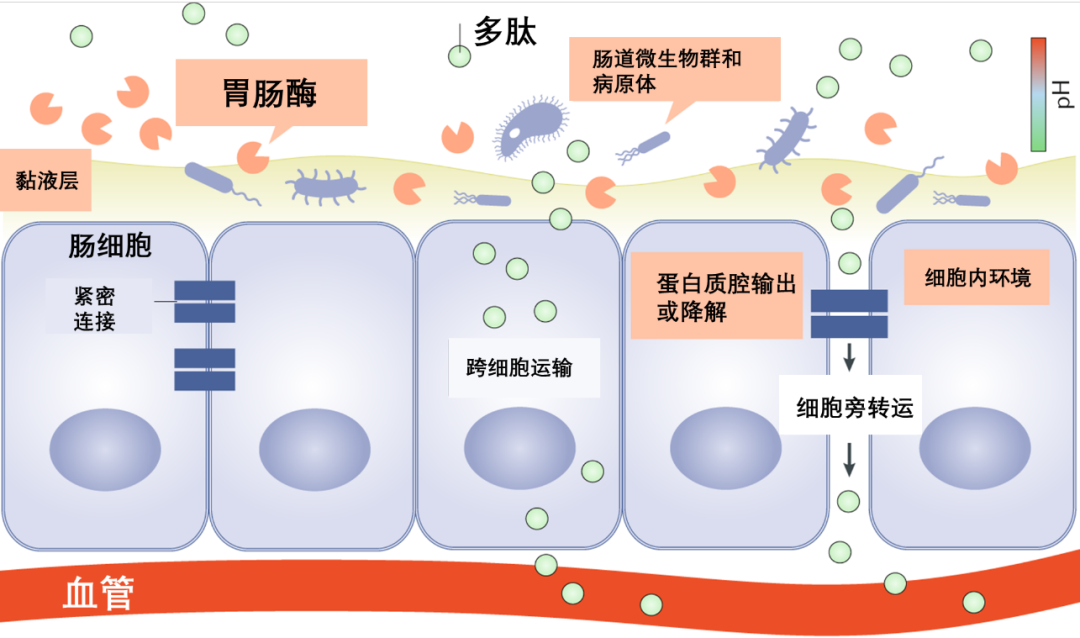
Figure 6. Schematic diagram of intestinal structure and challenges for oral peptide absorption
Although Novo Nordisk has developed an oral version of semaglutide, Rybelsus, oral peptide drugs have many restrictions on medication timing and diet, requiring fasting and water restriction. Although this peptide drug uses a special formulation, SNAC, to enhance gastric epithelial absorption and improve oral bioavailability, the bioavailability is only around 0.4~1%.
Due to the imperfect delivery technology, the bioavailability of orally administered peptide drugs is low, and the amount of active drug that can ultimately exert therapeutic effects is highly unstable. Only a few companies have successfully broken through the challenges of oral peptide formulations. Moreover, oral peptides generally require high doses. Since this year, the production capacity of semaglutide and tirzepatide has been insufficient, and the active pharmaceutical ingredients will be prioritized for the low-dose injectable versions, further limiting the production capacity of the oral versions.
The advantages of small-molecule GLP-1 receptor agonists (GLP-1-RA) are very obvious: they can avoid the technical bottleneck of oral peptides while improving patient compliance. In terms of production capacity, most small-molecule drugs are synthesized through liquid-phase processes, which do not have the limitations of solid-phase peptide synthesis. Regarding cost, the raw materials for small-molecule drugs and their Process Mass Intensity (PMI) offer significant advantages over peptides, making their costs lower as well. Therefore, if orally-administered small molecules can be successfully developed, they will also attract a segment of the audience.
But the development of oral peptides is difficult, and the development of small molecules is actually not simple either. The key lies in the issue of safety.
GLP-1 drugs are typically modified human GLP-1 molecules, which are molecules naturally produced by the body. Techniques such as amino acid substitution and the introduction of fatty acid chains are often used to reduce immunogenicity, making their safety relatively controllable. From a global R&D perspective, it is extremely rare for peptide pipeline products to fail to pass Phase I clinical trials.
Small-molecule drugs, on the other hand, need to be designed and screened from scratch. They are entirely new molecular entities for the human body, and their potential reactions within the body remain unknown, thus posing a safety blind spot. If the therapeutic effect turns out to be unsatisfactory or safety issues arise, it would mean that small-molecule weight-loss drugs could be at a competitive disadvantage.
Sure enough, Pfizer and Lilly's oral small molecules have encountered safety issues. Therefore, the threshold, cost, and risk of taking an alternative path also need to be balanced.
Conclusion
With its left and right arms broken, Pfizer has only two soldiers left in the GLP-1 small molecule track:One is Danuglipron, which is being restarted with once-daily dosing, and its pharmacokinetic studies are continuing to progress; the other is PF-06954522, another oral small-molecule GLP-1 receptor agonist developed in collaboration with Sosei Heptares. On November 6, 2023, it was announced that this drug had advanced to Phase I clinical trials. It was discovered through a multi-target research collaboration between Pfizer scientists and Sosei, utilizing Sosei's proprietary StaR® (stabilized receptor) technology. This drug is one of the key pipeline medications highlighted in Pfizer's recently disclosed Q3 2023 earnings report.

Figure 7. Pfizer Official Website Pipeline
Timely adjustment of pipelines is also a great wisdom. Moreover, the efficacy of Danuglipron is not bad. If its safety can be improved through formulation optimization, it will also have a place in the future market.
Hope this oral small-molecule weight-loss drug from Pfizer proceeds smoothly.
[1] Biospace.
[2]Pfizer Official Website
[3] Pu Gongying Ouryao: Over $2 Billion! AstraZeneca and Chengyi Bio Reach Exclusive Collaboration on GLP-1 Drug
[4] Peptide Research Society: Express | Pfizer Terminates Lotiglipron, What's the Impact on Small Molecule GLP-1RA Landscape?
[5] Empty Guest: [Listening to the Tide in the Sea of Medicine] Marginal Benefit is King: Pfizer's Oral GLP-1 Suffers Another Setback
- END -

Flagship Report
Column Recommendation




Peptide Research Society

Biopharmaceuticals · Beauty & Personal Care · Functional Foods
Animal Health · Green Agriculture · Biomaterials
Professional Focus | Achieving Customer Success | Growing Together