New Advances in Cancer Therapy Targeting TGF-β Signaling Pathways

Tessa Therapeutics
Solid Tumor T Cell Immunotherapy Developer
Transforming Growth Factor-β(TGF-β) Secretion is a hallmark of cancer development and a significant pathway for suppressing anti-tumor immunity. EliminationTGF-βThe research findings have profound positive implications for the future of immunotherapy.
Recently, researchers from Singapore's Tessa Therapeutics published a research paper titled "A novel GPI-anchored dominant-negative TGF-β receptor II renders T cells unresponsive to TGF-β signaling" in the Cell subsidiary journal, Molecular Therapy Oncology:

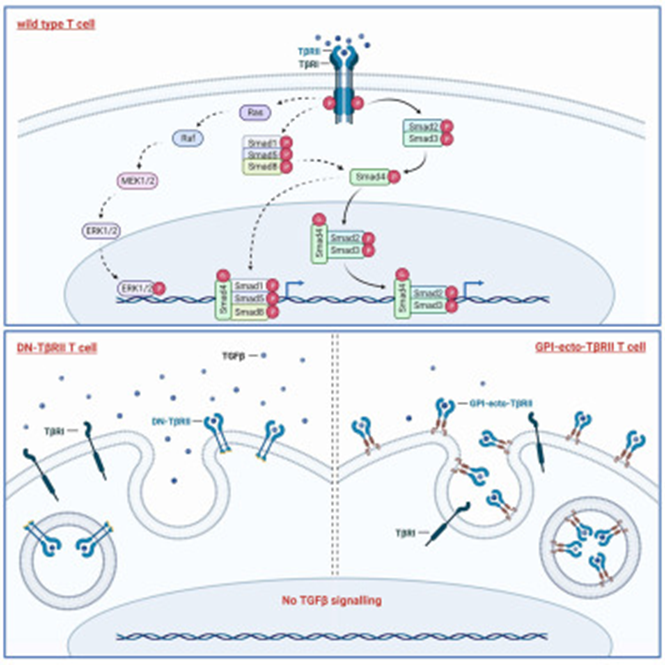
Design of Hemagglutinin (HA)-tagged decoy receptors, consisting of the extracellular domain of TGF-βRII (TβRII-ecto) linked to a glycosylphosphatidylinositol (GPI) anchor, was found to deeply inhibit TGF-β-induced SMAD phosphorylation. T cells transduced with lentiviruses expressing the GPI-ecto-TβRII construct continue to express high levels of cytokines such as interferon-γ (IFNγ) and granulocyte-macrophage colony-stimulating factor (GM-CSF), effectively capturing and inactivating TGF-β from their environment.In addition, studies have shown that cytotoxic T cells (CTL) expressing GPI-ecto-TβRII are regulators of tumor immune suppression and can reduce the detrimental effects of TGF-β in cancer immunotherapy.
Recently, researchers from Nanjing Medical University published a research commentary titled "New advances in cancer therapy targeting TGF-β signaling pathways" in the Cell subsidiary journal Molecular Therapy Oncology, discussing and reviewing new advances in cancer therapy targeting the TGF-β signaling pathway.

TGF-β Mediates Immunosuppression
Immunosuppression remains a major barrier to the efficacy of therapeutic interventions, which can be mediated through various mechanisms, such as immunomodulatory cytokines. TGF-β released by various cells in the tumor microenvironment (TME) suppresses the anti-tumor activity of immune cells, creating an immunosuppressive environment that impedes or diminishes the effectiveness of cancer immunotherapy.
Many clinical studies have linked high TGF-β levels to poor prognosis in various types of cancer. However, the development of TGF-β-targeted therapies has been slow, possibly due to: (1) the dual role mechanism of TGF-β in cancer; (2) severe toxicity, such as neurological disorders and cytokine release syndrome (CRS), which may also occur due to blocking TGF-β activity in normal cells outside the tumor microenvironment (TME); and (3) downstream mechanisms of the TGF-β signaling pathway, as well as biomarkers suitable for patients receiving TGF-β-targeted therapy and optimal dosing regimens, are still in the early stages of research. Although T cells expressing the GPI-ecto-TβRII construct do not affect the proliferation or phenotype of transduced T cells under standard culture conditions, further in vivo experimental data and preclinical models are still needed to validate the safety of this construct.
Therapeutic Strategies for Inhibiting the TGF-β Signaling Pathway
Currently, a series of treatment methods targeting the TGF-β/SMAD signaling pathway and cell-targeting approaches to inhibit the TGF-β signaling pathway are under development, some of which are in clinical trials. Methods to inhibit TGF-β signaling are divided into five major categories.
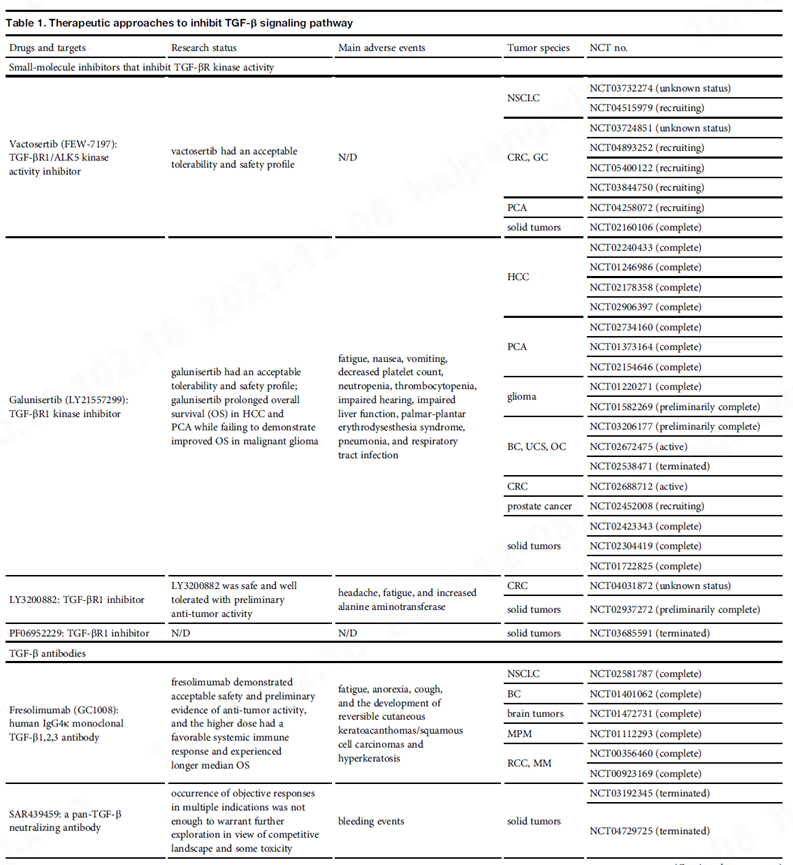
One class consists of small molecule inhibitors of TGF-β receptor kinase.These block the binding of ATP to the ATP-binding pocket of the TGF-β receptor (mainly TβRI), thereby blocking the activation of SMAD2 and SMAD3. However, despite the simplicity of oral administration, these inhibitors have poor pharmacokinetics and pharmacodynamics. Additionally, they are equally effective in inhibiting several other TGF-β-related proteins and kinase receptors.
Another class of therapies includes monoclonal antibodies that block TGF-β receptor binding ligands.Although neutralizing TGF-β antibodies exhibit good ligand specificity, they need to effectively interfere with the very high binding affinity between TGF-β and the cell surface receptor complex. However, the production cost of antibodies is high, and their intratumoral distribution is inefficient. Therefore, some other inhibitors have been designed as soluble, high-affinity ligand traps to prevent TGF-β from binding to its receptors. These include Fc-stabilized dimers of the TβRII extracellular domain, which are designed to chelate TGF-β1 and TGF-β3, but not TGF-β2, thereby blocking their binding to the transmembrane TβRII receptor.
In addition, some antibodies and small molecules target the TGF-β activation process,Thereby providing selective cell or tissue type inhibition of TGF-β signaling.
Finally, antisense oligonucleotides (ASOs)Single-stranded DNA or RNA sequences composed of 15-25 nucleotides that directly inhibit the synthesis of TGF-β by targeting and interfering with transcription or translation processes. ASOs possess high specificity, high efficiency, safety, and low toxicity, showing broad application prospects in gene therapy. However, clinical practice development faces many limitations, such as instability of ASO molecules and insufficient cellular uptake.
Combination of TGF-β Blockade with Anticancer Therapy
Since inhibiting TGF-β signaling can suppress immunosuppressive activity, angiogenic responses, and the activation of cancer-associated fibroblast (CAF) populations in the tumor microenvironment (TME), inhibiting TGF-β signaling can enhance the efficacy of other treatments. Moreover, TGF-β signaling-driven epithelial-mesenchymal transition (EMT) in cancer cells also promotes cancer drug resistance and cancer stem cell properties. Therefore, targeting the inhibition of TGF-β signaling and/or EMT in cancer cells, combined with cytotoxic or radiation therapy, holds promise for suppressing cancer progression. Due to the emphasis on immunotherapy, the combination of anti-TGF-β and checkpoint inhibitors is receiving close attention.
Increased TGF-β signaling in the TME has been associated with poorer overall survival and resistance to immune checkpoint blockade of PD-L1 or its receptor PD-1. Considering TGF-β, CTLA-4, and PD-L1/PD-1 signaling as parallel immunosuppressive pathways that inhibit cytotoxic T lymphocytes (CTLs), natural killer (NK) cells, and macrophage activity through distinct mechanisms, blocking TGF-β signaling should suppress immunosuppressive activity and enhance the success rate of immune checkpoint inhibitors (ICIs) or other immunotherapy approaches.Several combination therapies have been clinically pre-evaluated in mouse cancer models. Thus, the novel GPI-anchored dominant-negative TβRII can be further combined with ICIs to assess efficacy and adverse reactions in preclinical models, thereby further translating to clinical applications.
Since TGF-β inhibits the activation of cytotoxic T lymphocytes, research has focused on suppressing TGF-β to enhance the efficacy of CAR-T cell therapy. The TβRI inhibitor SM16A enhances T cell transfer and antitumor efficacy in mice with mesothelioma. Further modifications of CAR-T cells generate engineered T cells expressing an extracellular single-chain variable fragment that neutralizes TGF-β antibodies. These CAR-T cells respond to TGF-β through dimerized TGF-β-binding CARs, leading to T cell activation. Thus, instead of exerting its normal immunosuppressive effects, TGF-β acts as a potent immunostimulant for these CAR-T cells. This design enables CAR-T cells to target areas within the tumor microenvironment (TME) with high levels of TGF-β. Other studies have also shown that adoptive T cells (ATCs) co-expressing CAR and GPI-TβRII can significantly and effectively kill cancer cell spheroids that secrete antigens.
Overall, the GPI-ecto-TβRII construct designed by Singapore's Tessa Therapeutics represents a promising therapeutic strategy.Because it establishes higher affinity than before, T cell activation, TGF-β depletion in the TME, thereby antagonizing tumor immunosuppression.However, the efficacy of this construct has not been compared or combined with ICIs or CAR-T therapy, and thus cannot reflect its advantages in clinical applications. Most importantly, although the TME has a significant impact on tumor treatment outcomes, there is a lack of in vivo study results. Additionally, drugs that inhibit the TGF-β signaling pathway have shown various adverse effects in the past, so the safety of this therapeutic intervention needs further exploration. Finally, even with promising results in preclinical models, the failure of multiple drugs that inhibit the TGF-β signaling pathway suggests that higher-level evidence is still needed in the future.
Reference:New advances in cancer therapy targeting TGF-β signaling pathways. Mol Ther Oncolytics. https://doi.org/10.1016/j.omto.2023.100755