Johnson & Johnson recently announced the submission of a supplemental Biologics License Application (sBLA) and a New Drug Application (NDA) to the U.S. FDA, as well as a Marketing Authorization Application for this indication to the European Medicines Agency (EMA), seeking approval for Rybrevant (amivantamab) in combination with the third-generation epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor (TKI) oral medication lazertinib for the first-line treatment of adult patients with locally advanced or metastatic non-small cell lung cancer (NSCLC) harboring EGFR exon 19 deletions (ex19del) or L858R substitution mutations.
Osimertinib, as the world's first third-generation EGFR inhibitor, was approved for marketing in 2015. According to AstraZeneca's annual report, its global sales reached $5.444 billion in 2022, and $2.92 billion in the first half of 2023, with the potential to exceed $6 billion for the full year. The success of Amivantamab/Lazertinib in head-to-head first-line treatment for NSCLC against Osimertinib speaks volumes about its market potential. However, as the defending champion, AstraZeneca has not been idle. It has been continuously enhancing the efficacy of Osimertinib while going head-to-head with Johnson & Johnson, developing a new generation of bispecific antibody EGFR/cMET-ADC.
First, let's take a look at the clinical data for Johnson & Johnson's new indication: The application for this new indication is based on a Phase III, multicenter, randomized clinical study called MARIPOSA (NCT04487080). This study primarily explores the efficacy and safety of the combination therapy of amivantamab and lazertinib (ami+laz) as a first-line treatment for EGFR-mutated non-small cell lung cancer, with osimertinib (osi) and lazertinib monotherapy (laz) serving as control groups. At a recent ESMO conference, Johnson & Johnson presented the clinical efficacy of this therapy.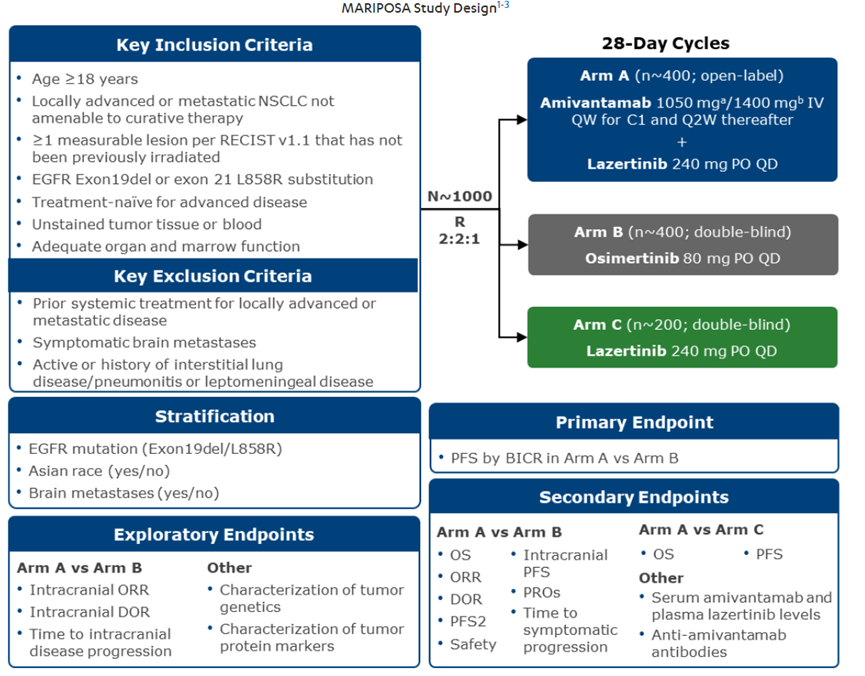 This clinical trial enrolled a total of 1074 patients, who were randomized in a 2:2:1 ratio to receive ami+laz, osi, and laz (429, 429, and 216), respectively. After an average follow-up of 22 months, compared with osimertinib (osi) treatment, ami+laz reduced the risk of death and disease progression by 30% (HR, 0.70; 95% CI, 0.58-0.85; P<0.001). The mPFS for the two treatments (ami+laz vs osi) was 23.7 months (95% CI, 19.1-27.7) vs 16.6 months (95% CI, 14.8-18.5). However, there was almost no difference in ORR between the two treatments: 86% (95% CI, 83-89) for ami+laz vs 85% (95% CI, 81-88) for osi. In terms of mDoR, the ami+laz treatment group showed a significant improvement: 25.8 months (95% CI, 20.1-N.E.) vs 16.8 months (95% CI, 14.8-18.5) for the osi group. For median OS, ami+laz treatment demonstrated a favorable trend (HR, 0.80; 95% CI, 0.61-1.05; P=0.1).
This clinical trial enrolled a total of 1074 patients, who were randomized in a 2:2:1 ratio to receive ami+laz, osi, and laz (429, 429, and 216), respectively. After an average follow-up of 22 months, compared with osimertinib (osi) treatment, ami+laz reduced the risk of death and disease progression by 30% (HR, 0.70; 95% CI, 0.58-0.85; P<0.001). The mPFS for the two treatments (ami+laz vs osi) was 23.7 months (95% CI, 19.1-27.7) vs 16.6 months (95% CI, 14.8-18.5). However, there was almost no difference in ORR between the two treatments: 86% (95% CI, 83-89) for ami+laz vs 85% (95% CI, 81-88) for osi. In terms of mDoR, the ami+laz treatment group showed a significant improvement: 25.8 months (95% CI, 20.1-N.E.) vs 16.8 months (95% CI, 14.8-18.5) for the osi group. For median OS, ami+laz treatment demonstrated a favorable trend (HR, 0.80; 95% CI, 0.61-1.05; P=0.1).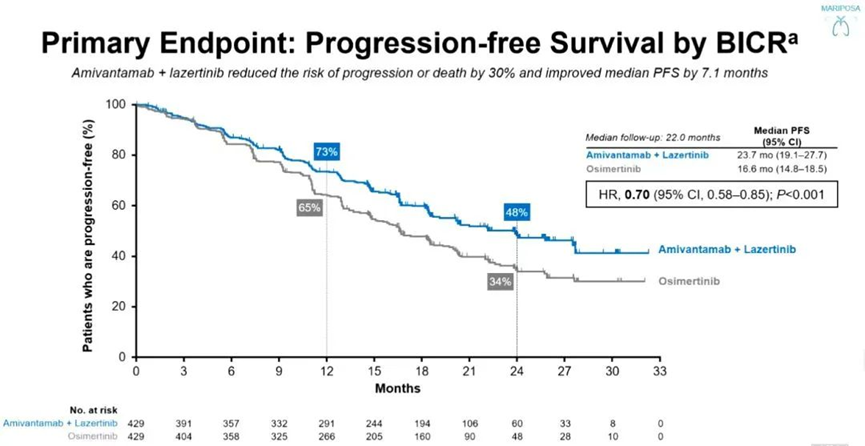
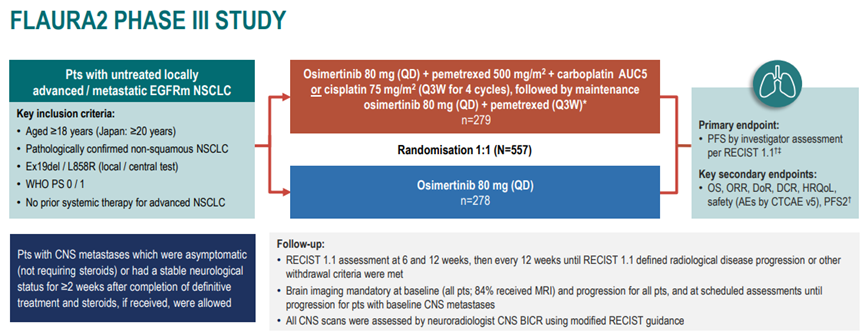
To defeat magic, one must rely on magic. While Johnson & Johnson was launching its attack, AstraZeneca did not stand still either. It also adopted combination therapy, but with a different approach: combining Osimertinib and chemotherapy. At this year's ESMO conference, AstraZeneca and its researchers announced the FLAURA2 clinical study data. This clinical trial is an international, multicenter, open-label, randomized controlled Phase III study designed to evaluate the efficacy and safety of Osimertinib combined with pemetrexed and platinum-based chemotherapy compared to Osimertinib monotherapy as a first-line treatment for patients with advanced non-small cell lung cancer (NSCLC) carrying EGFR-sensitive mutations (exon 19 deletion mutations or exon 21 L858R point mutations).
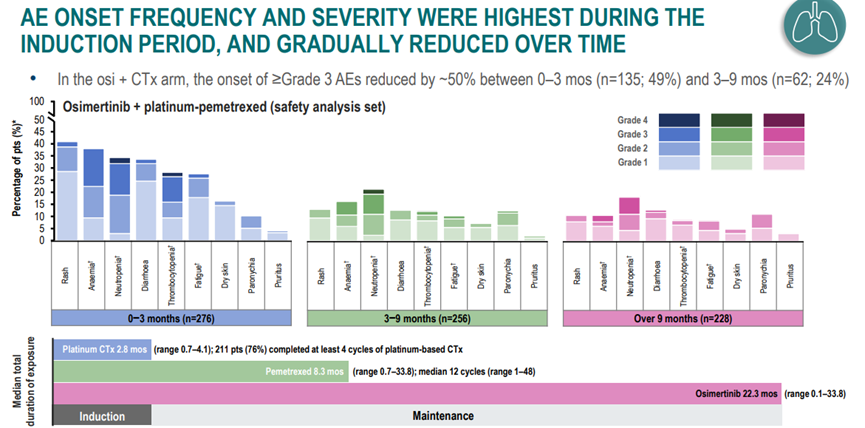
The clinical study design is shown in the figure below: 557 treatment-naïve patients with locally advanced/metastatic NSCLC carrying EGFR sensitizing mutations were randomized 1:1 to receive either osimertinib combined with chemotherapy (N = 279, patients initially received osimertinib + pemetrexed + carboplatin or cisplatin, followed by maintenance therapy with osimertinib + pemetrexed on a Q3W regimen) or osimertinib monotherapy control group (N = 278, Q3W), until disease progression or intolerable toxicity occurred.
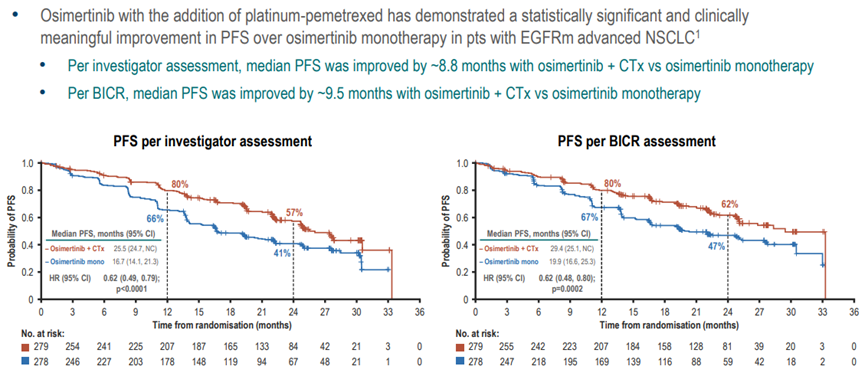
As of April 3, 2023, the median PFS in the osimertinib plus chemotherapy group was extended by 8.8 months compared to the osimertinib monotherapy group (25.5 months vs 16.7 months; HR = 0.62, p<0.0001). The mPFS assessed by BICR in the osimertinib plus chemotherapy group also showed a significant extension of 9.5 months compared to the osimertinib monotherapy group (29.4 months vs 19.9 months; HR = 0.62, p = 0.0002).
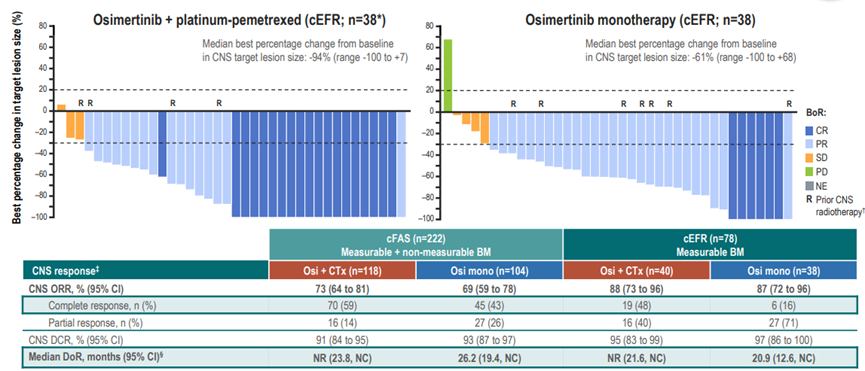
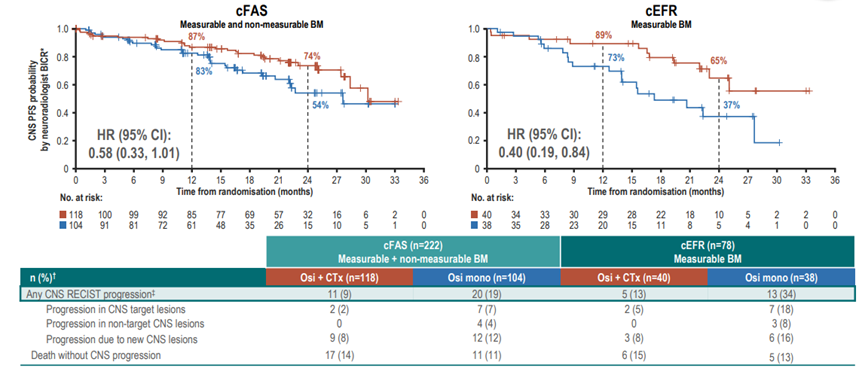
In relevant subgroup analyses, osimertinib combined with chemotherapy showed better efficacy compared to osimertinib monotherapy, such as in patients with CNS metastases. In this subgroup, the ORR for the osimertinib plus chemotherapy group and the control group (osimertinib monotherapy) was 88% and 87%, respectively, while the CR was 48% and 16%, respectively. However, for PFS, whether at 12 months or 24 months, the combination therapy showed improvement over monotherapy.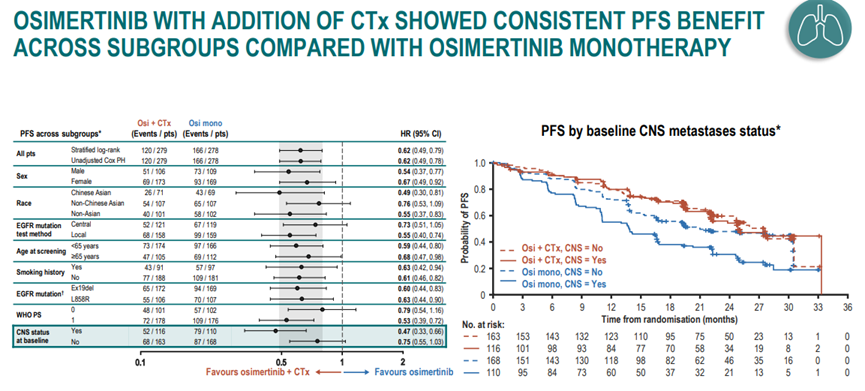
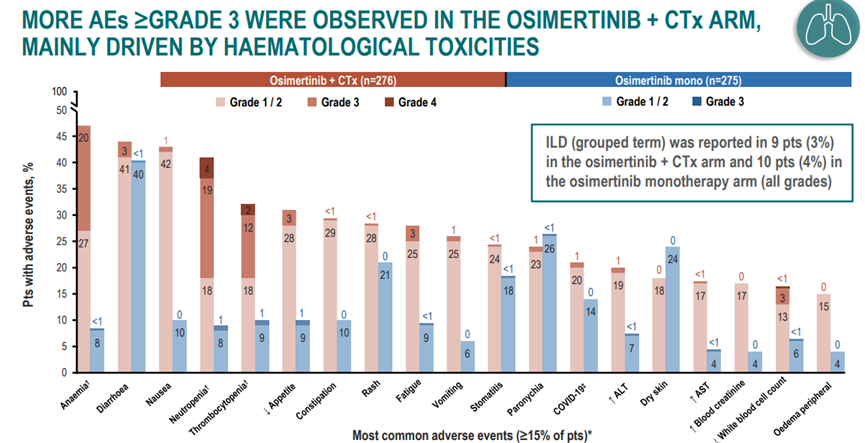
 In terms of safetyIn the combination therapy and osimertinib monotherapy groups, the incidence rates of grade ≥3 adverse events (AEs) were 64% and 27%, respectively. The incidence rates of AEs leading to osimertinib discontinuation were 11% and 6%, respectively. In both regimens, the overall incidence rates of treatment-related adverse events (TRAEs) were 97% and 88%, respectively, with the majority being mild or moderate. Additionally, the incidence rates of interstitial lung disease (ILD) in the combination therapy and monotherapy groups were 3% and 4%, respectively.
In terms of safetyIn the combination therapy and osimertinib monotherapy groups, the incidence rates of grade ≥3 adverse events (AEs) were 64% and 27%, respectively. The incidence rates of AEs leading to osimertinib discontinuation were 11% and 6%, respectively. In both regimens, the overall incidence rates of treatment-related adverse events (TRAEs) were 97% and 88%, respectively, with the majority being mild or moderate. Additionally, the incidence rates of interstitial lung disease (ILD) in the combination therapy and monotherapy groups were 3% and 4%, respectively.
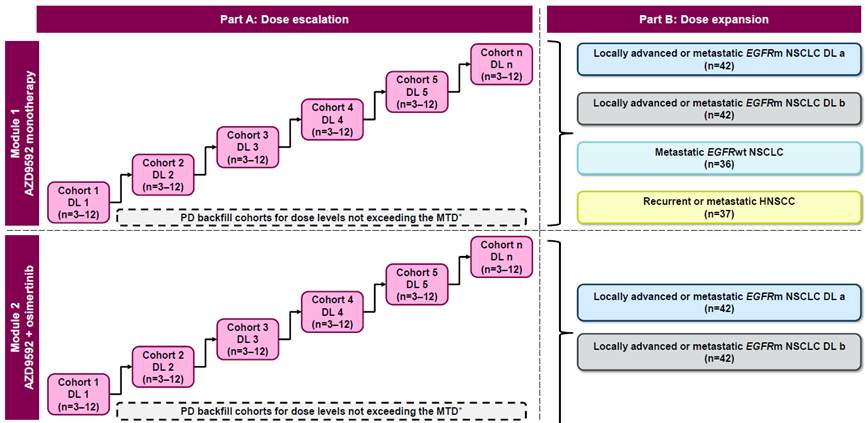
Of course, in addition to combination with chemotherapy, AstraZeneca has also developed a bispecific antibody targeting EGFR/cMET, which has been further upgraded into a bispecific antibody-drug conjugate (ADC), AZD9592. This bispecific antibody entered clinical research in 2022 (NCT05647122) to investigate the efficacy of this bispecific ADC in EGFR-mutated NSCLC. The clinical trial is divided into two parts: evaluating the safety and efficacy of AZD9592 as monotherapy, and the safety and efficacy of AZD9592 in combination with osimertinib. Additionally, based on initial dose escalation, a dose expansion study will be conducted to further evaluate the efficacy of this bispecific ADC.
Summary
On May 21, 2021, based on the CHRYSALIS study, Amivantamab received FDA approval for marketing to treat patients with metastatic non-small cell lung cancer (NSCLC) carrying EGFR exon 20 insertion mutations whose disease has progressed after platinum-based chemotherapy. This is the first targeted drug for treating EGFR exon 20 insertion mutations. However, Johnson & Johnson has not stopped there. It has not only targeted the market for osimertinib resistance but has also advanced to the front line, directly competing with osimertinib for a market that is now approaching $6 billion.
In an era of fierce competition, standing still means falling behind. Therefore, as the defending champion, AstraZeneca has not been idle. While exploring the combination of Osimertinib and chemotherapy, it is also investigating new drug modalities and has developed a bispecific antibody-drug conjugate (ADC) targeting the same point as Johnson & Johnson. Moreover, relying on its current platforms such as ADCs and immune bispecific antibodies, AstraZeneca still has many strategic combinations to explore.
Scan the WeChat QR code, add the editor of the Antibody Circle, and those who meet the requirements can join the Antibody Circle WeChat group!
Please indicate: Name + Research Direction!All reproduced articles in this official account are intended to convey more information, with the source and author clearly stated. Media or individuals who do not wish to be reproduced can contact us (cbplib@163.com), and we will immediately proceed with deletion. All articles represent the views of the author and do not represent the position of this site.