Medtronic's TurboHawk™ Plus Peripheral Directional Atherectomy System Receives NMPA Approval in Mainland China

Medtronic
Chronic Disease Medical Device and Therapy Developer


With the introduction of the "Leave Nothing Behind" concept, a new era has dawned in the field of lower extremity arterial occlusive disease. Percutaneous Transluminal Directional Atherectomy (DA), as an effective debulking method, offers a new treatment option for moderate to severe calcified lesions while laying the foundation for Drug-Coated Balloon (DCB) application, contributing to improved long-term patency rates. Whether in core lab evaluations or real-world studies,Plaque debulking reduces plaque burden, significantly decreases the occurrence of flow-limiting dissections, and achieves greater lumen volume during follow-up.Benefiting numerous patients with lower limb arterial diseases.
Medtronic is committed to the continuous innovation and introduction of medical devices, with the latest third-generation Hawk product launched globally this time.TurboHawk™ Plus Peripheral Directional Atherectomy System Officially Approved in China (Registration No.: 20233010606), also marks the emergence of a new treatment option for peripheral vascular intervention.
Indications
Suitable for plaque removal in the peripheral vascular system. When used with Spider FX™When used in conjunction with the series of embolic protection devices, it can be used to treat severely calcified vascular lesions (not applicable to coronary, carotid, iliac, or renal arteries).
Product Features
Significant improvements over the second-generation Turbohawk™ Peripheral Plaque Excision System include:
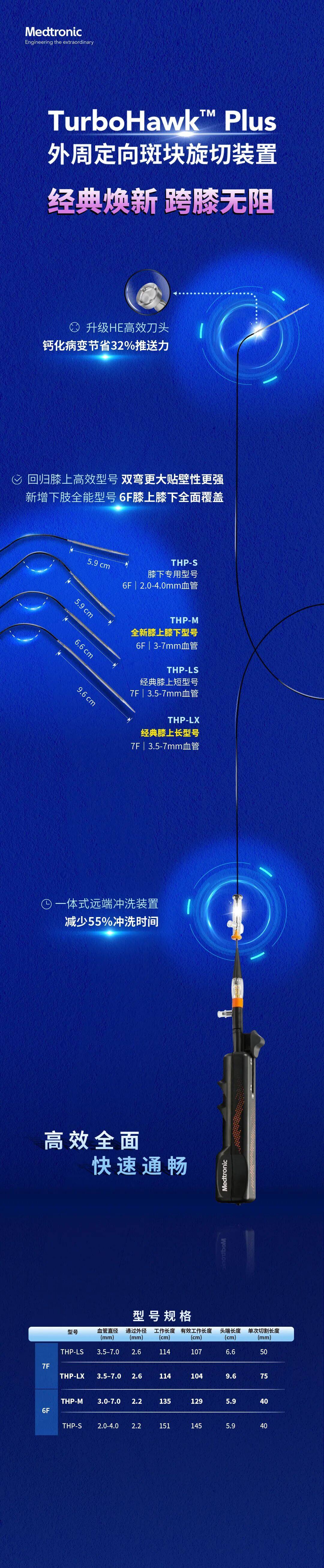
Upgraded High-Efficiency Blade:Reduce the pushing force of calcified lesions and improve cutting efficiency.
Enhanced double-bend for improved wall apposition, modified pusher catheter design:Enriched the selection of above-knee and below-knee models, improving cutting precision and controllability.
Integrated Distal Flush Device:Reduce flushing time by 55% and double the flushing efficiency.
Full visibility of the distal end:Improves positioning accuracy when used in conjunction with a distal protection device.
Technical Highlights
Among the highlights worth mentioning are:
9.6cm Tip, High-Efficiency Blade: The Classic Above-Knee Model Returns,And improve the double-bend design to 90°, providing stronger large-lumen wall apposition capability, effectively enhancing the handling capacity for moderate to severe calcified plaques.
Simultaneously launch a brand-new 6F large dual-bend cutting catheter.,Fully covers from the superficial femoral artery to the tibiofibular trunk, addressing the clinical pain point of varying vessel diameters above and below the knee that require model changes, effectively targeting cross-joint lesions and tandem lesions above and below the knee.
Evidence-based Evidence
DA as a monotherapy for treating lesions above and below the knee.DEFINITIVE LE Study[1]YesCurrently the clinical study with the largest number of follow-up cases for peripheral atherectomy. The 12-month follow-up results showed that the stent rescue rate after the application of DA was 3.2%, the primary patency rate at 12 months for patients with claudication was 78%, and the major unplanned amputation-free rate of the target limb at 12 months for CLI patients was 95%. This indicates that DA is a safe and effective treatment method for both claudication and CLI patients.
DA as a pre-DCB lumen preparation therapy.To further evaluate the role of DA application prior to DCB,DEFINITIVE AR Study[2]A total of 102 patients with claudication or rest pain were randomly divided into the DA+DCB group (n=48) or the DCB alone group (n=54), including 19 patients with severe calcified lesions treated with DA+DCB. The study results showed a higher technical success rate in the DA+DCB group (89.6% vs. 64.2%), a lower dissection rate in the DA+DCB group, an overall stent implantation rate of 3.7%, and at 12-month follow-up, the DA+DCB group demonstrated better patency rates and lumen diameter gain compared to the DCB alone group.
REALITYResearch[3]Evaluation of Directional Atherectomy Combined with DCB Angioplasty for Symptomatic Severe Calcification in Femoropopliteal Arteries: The success rate of DCB+DA surgery was 57.6%, the rate of bailout stenting was 8.8%, and follow-up at 395 days showed a primary patency rate of 76.7%, with a CD-TLR-free rate of 92.6%. The results were satisfactory. In terms of complications, TLR was 7%, the major amputation rate was 1%, and MAE was 22%. These findings confirm that DA combined with DCB is safe and effective in complex lesions.
The introduction of TurboHawk™ Plus can better enhance the clinical application experience of debulking devices, especially for some lesions that are traditionally difficult to manage, such asCross-joint lesions, moderate to severe calcified lesions, eccentric lesions, effectively avoiding dissection, reducing unnecessary stent placement, and restoring the natural lumen shape.,It is a true reduction in volume, one of the most ideal vessel preparation methods before DCB, preserving future treatment options for patients.
A new chapter has begun, and we look forward to more clinical feedback and research data to witness the continuous progress in the diagnosis and treatment of lower extremity arterial diseases.
References:
[1]James F. McKinsey, Thomas Zeller, Krishna J. Rocha-Singh, et al. Lower Extremity Revascularization Using Directional Atherectomy: 12-Month Prospective Results of the DEFINITIVE LE Study. JACC: CARDIOVASCULAR INTERVENTIONS. 2014;7(8):923-3.
[2]Thomas Zeller, Ralf Langhoff, Krishna J. Rocha-Singh, et al. Directional Atherectomy Followed by a Paclitaxel-Coated Balloon to Inhibit Restenosis and Maintain Vessel Patency: Twelve-Month Results of the DEFINITIVE AR Study. Circ Cardiovasc Interv. 2017;10:e004848.
[3]Krishna J. Rocha-Singh, Ravish Sachar, Brian G. DeRubertis, et al. Directional atherectomy before paclitaxel coated balloon angioplasty in complex femoropopliteal disease: The VIVA REALITY study. Catheter Cardiovasc Interv. 2021;1-10.
Copyright Statement: This platform aims to help healthcare professionals better understand the latest developments in related disease areas. The information published on this platform does not imply agreement with its descriptions or viewpoints; it is only intended to provide more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will address them as soon as possible. This information is solely for healthcare professionals to stay informed and should not replace professional medical guidance in any way, nor should it be regarded as medical advice. If such information is used for purposes other than staying informed, this platform and its authors assume no responsibility.Contact email for cooperation:vascular@edoctor.cn。

