New Drug Approvals Bring Hope—But Is It Real Progress in the Battle Against 'King of Cancers'?

Ipsen
Biopharmaceutical Manufacturer

NeoImmuneTech
Developer of Novel Immunotherapies
On February 13, French listed company Ipsen announced that the FDA had approved the liposomal irinotecan injection Onivyde for use in the NALIRIFOX regimen, which combines fluorouracil, oxaliplatin, and leucovorin, as a first-line treatment for metastatic pancreatic cancer (mPDAC). This marks the first approved first-line mPDAC drug in over a decade. Notably, in China, two liposomal irinotecan injections have been approved for marketing by domestic companies Shijie and Hengrui, both of which are used in combination with fluorouracil and leucovorin for mPDAC.
In addition, in early February, the FDA also granted NeoImmuneTech’s NT-17 Orphan Drug Designation (ODD) status as a potential treatment option for patients with pancreatic cancer.
Pancreatic cancer has long been referred to as the "king of cancers" in academic circles due to its insidious clinical symptoms, high malignancy, rapid progression, and poor prognosis. The incidence and mortality rates are almost identical, with over 80% of patients already progressed to advanced stages at the time of diagnosis, and the median overall survival is less than one year. Conventional treatment methods have shown limited efficacy, resulting in numerous unmet clinical needs within the field of pancreatic cancer.
With the continuous approval of new drugs, it seems that the high barriers of pancreatic cancer are showing signs of loosening. However, reviewing the clinical trial records over the years, perhaps we have only just taken the first step.
Precision medicine that varies according to the same disease, individual differences, and stages of the disease has become a developmental trend in pancreatic cancer treatment.
In September 2023, the European Society for Medical Oncology (ESMO) Guidelines Committee updated the pancreatic cancer diagnosis and treatment guidelines. This marks the first update to the ESMO pancreatic cancer guidelines in eight years. The new edition significantly expands on the previous version, reflecting recent advancements in the field of pancreatic cancer diagnosis and treatment, as well as indicating future trends in this area.
In the previous version of the ESMO guidelines, there were no recommended targeted therapies for pancreatic cancer. In the new edition of the ESMO pancreatic cancer guidelines, three targeted drugs are now available, although the proportion of patients who are suitable for these treatments remains low. This indicates that precision medicine is the future direction for overcoming pancreatic cancer.
For patients with germline BRCA gene mutations (accounting for 5%-7%), chemotherapy regimens based on platinum drugs are recommended; for pancreatic cancer patients with high microsatellite instability/mismatch repair deficiency (accounting for about 0.8%), pembrolizumab is recommended; for pancreatic cancer patients with NTRK gene fusion (seen in KRAS wild-type pancreatic cancer, total proportion >1%), larotrectinib or entrectinib is recommended.
The indications for these three drugs are all advanced pancreatic cancer. In the future, they will gradually expand to the adjuvant treatment stage. Meanwhile, the combination treatment regimens of these drugs with different chemotherapy protocols and cycles still need further exploration.
Surgical resection remains an effective method for pancreatic cancer patients to achieve a chance of cure and long-term survival; however, over 80% of pancreatic cancer patients lose the opportunity for surgery due to advanced stages of the disease. Currently, commonly used chemotherapy drugs for treating unresectable locally advanced or metastatic pancreatic cancer include gemcitabine, albumin-bound paclitaxel, fluorouracil, cisplatin, oxaliplatin, and irinotecan. Targeted drugs include erlotinib, larotrectinib, and olaparib. However, reviewing the clinical trials of these drugs seems to reveal a sense of old wine in new bottles.
At first glance, there is a glimmer of hope for drug development targeting pancreatic cancer, but clinical research data shows that the field has remained almost stagnant for many years.
The world's first randomized controlled trial targeting advanced pancreatic cancer was published in 1997. The study, led by Professor Brurris and his team, evaluated the efficacy of gemcitabine compared to fluorouracil (5-FU) and busulfan in untreated patients with metastatic pancreatic adenocarcinoma. Notably, this study has been cited over 7,000 times and is the most-cited article in the 40-year history of the Journal of Clinical Oncology.
The primary outcome of the study was a composite assessment of three quality-of-life indicators, including pain, dosage of anesthetic analgesics, and net weight gain. Overall, gemcitabine not only improved quality of life but also increased the median overall survival (OS) by 1 month.
This study not only prompted the FDA to approve gemcitabine for the treatment of metastatic pancreatic cancer but also triggered a wave of participation in pancreatic cancer research from both academia and pharmaceutical companies. More importantly, the study was a pioneer in many aspects, such as establishing dual primary endpoints that include quality of life and survival time. It is important to note that while overall survival (OS) remains the gold standard for evaluating tumor drugs, indicators such as quality of life (QoL) and patient-reported outcomes (PRO) have only gained attention in recent years.
Notably, although researchers at the time believed that a four-week increase in median overall survival was not a significant breakthrough and, at most, considered it a modest benefit, subsequent clinical studies have highlighted even a 10-day survival benefit.
From 2000 to the end of October 2023, according to ClinicalTrials data, there were 485 Phase I, 614 Phase II, and 85 Phase III clinical trial registrations for pancreatic cancer drugs. In 2007, the results of a Phase III randomized controlled clinical trial comparing gemcitabine plus erlotinib with gemcitabine plus placebo for the treatment of advanced pancreatic cancer patients were published, showing that the primary endpoint was reached. Although the median improvement in overall survival was only 10 days, it achieved statistical significance and was therefore heavily promoted; the FDA also approved this therapy.
By 2011, a clinical trial named FOLFIRINOX (leucovorin, fluorouracil, irinotecan, and oxaliplatin) versus gemcitabine brought about a gain of approximately 4 months in overall survival and an improvement in quality of life. However, since these drugs had already been approved for other cancer therapies, no new drug approval was granted. In 2013, another study showed that nab-paclitaxel combined with gemcitabine provided less than 2 months of overall survival benefit compared to gemcitabine alone.
The intriguing part is that the price of albumin-bound paclitaxel is nearly 50 times that of conventional paclitaxel. Although some studies suggest that albumin-bound paclitaxel has fewer neurological and infusion-related reactions, whether these minor differences in side effects justify the substantial price difference remains a topic of debate within the industry. However, the reality is that albumin-bound paclitaxel has been successfully approved for use in pancreatic cancer, whereas paclitaxel has never received approval.
Following the precedent set by albumin-bound paclitaxel, some subsequent studies began to "follow suit."
In 2016, the NAPOLI-1 study tested the efficacy of fluorouracil combined with liposomal irinotecan in patients who had been treated with gemcitabine but were intolerant to irinotecan. Although the overall survival was extended by less than two months, the study did achieve statistical significance, leading to the drug's approval by the FDA.
Following the success of the 2011 FOLFIRINOX study, it is reasonable to conclude that irinotecan is effective against pancreatic cancer. However, the new study did not test the combination of fluorouracil and irinotecan but instead opted for the more expensive liposomal irinotecan. Consequently, some in the industry argue that research on drugs like albumin-bound paclitaxel and liposomal irinotecan represents innovation for the sake of innovation.
If the aforementioned studies were only slightly controversial, the POLO study published in 2019 sparked significant debate.
The study recruited patients who responded effectively to chemotherapy and then randomly assigned them to either the olaparib group or the placebo group four months after chemotherapy. Regardless of the ethical concerns regarding assigning chemotherapy-responsive patients to the control group after halting treatment, the controversial aspect of the POLO study lies in the choice of the primary endpoint. This is the first pancreatic cancer drug trial to use progression-free survival (PFS) rather than overall survival as the primary endpoint.
Although it did improve progression-free survival, on one hand, the control group did not receive active therapy, and on the other hand, overall survival and quality of life were not improved. The conclusion of the trial was that, while no statistically significant overall survival benefit was observed, the hazard ratio numerically favored Olaparib. Ultimately, the FDA still approved the indication.
At the 2023 ASCO American Society of Clinical Oncology, the results of the NAPOLI-3 clinical trial were published, continuing the previous pattern of selecting high-priced drugs.
This randomized controlled trial assigned patients with advanced pancreatic cancer to receive either NALIRIFoX (liposomal irinotecan, fluorouracil, leucovorin, and oxaliplatin) or gemcitabine plus nab-paclitaxel. In comparison, the NALIRIFoX regimen extended overall survival (OS) by 17%.
Compared with the FOLFIRINOX trial, NALIRIFoX also uses the more expensive liposomal irinotecan instead of the conventional version. Therefore, some in the academic community believe that the trial should compare NALIRIFoX with FOLFIRINOX. This viewpoint is also supported by data. In the NALIRIFoX trial, the median overall survival was 11.1 months, while the corresponding data from the 2011 FOLFIRINOX trial was also 11.1 months, showing no significant improvement between the two.
A review of clinical trials on pancreatic cancer treatment over the past 25 years reveals a frustrating fact: despite the approval of several new drugs, such as gemcitabine, erlotinib, nab-paclitaxel, liposomal irinotecan, and olaparib, which have also been recommended for first-line or second-line treatment regimens, the median survival time for patients in multiple clinical trials remains less than one year. Among them, the best survival period for the older drug combination therapy FOLFIRINOX is 11 months.
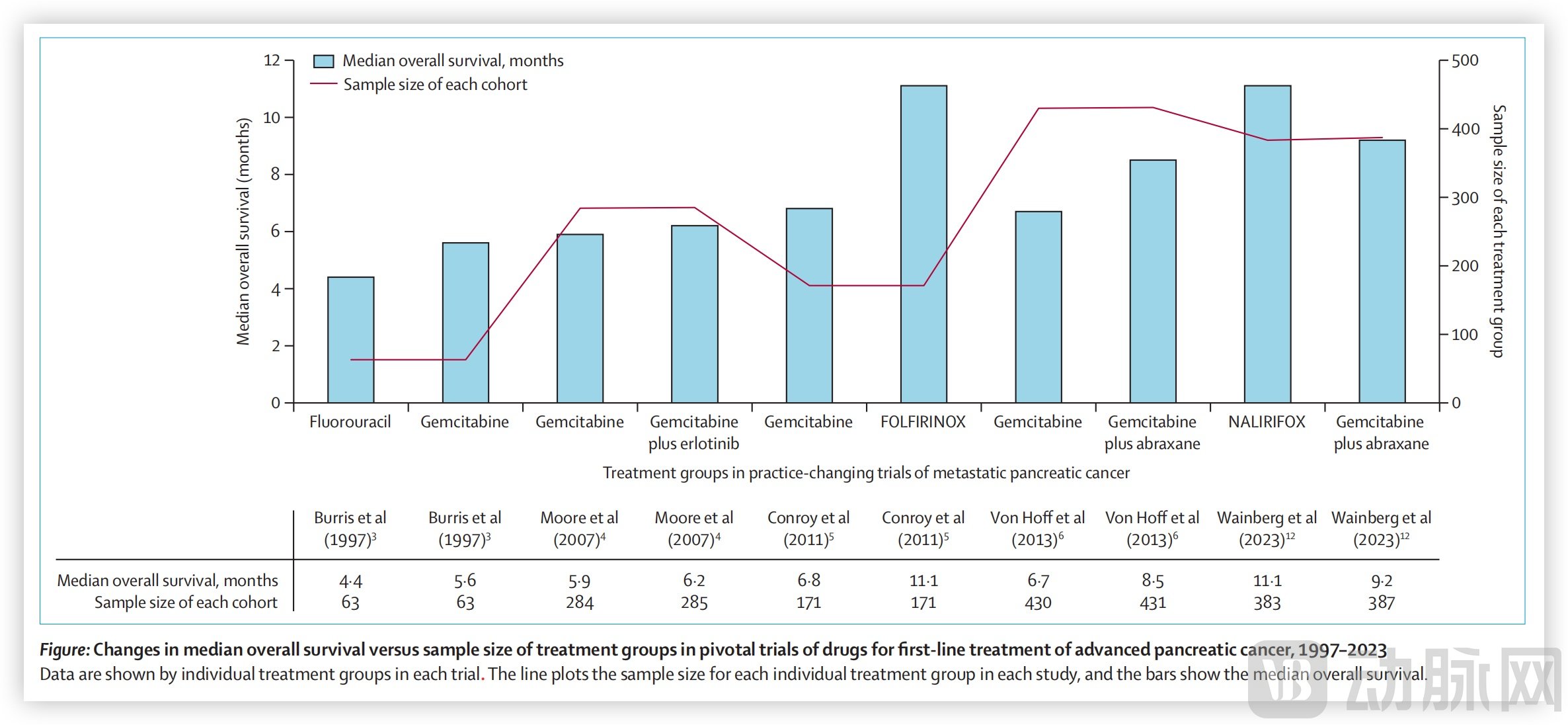
Changes in Median Overall Survival and Sample Size in Pancreatic Cancer Drug Clinical Trials; Image Source: PMID: 38301687
These randomized controlled trials have shown two distinct trends over time.
First, perhaps to detect smaller differences, the sample sizes of clinical trials have gradually increased. The gemcitabine trial in 1997 had only 126 patients; the gemcitabine plus erlotinib trial in 2007 recruited 569 patients; the FOLFIRINOX trial recruited 342 patients; the gemcitabine plus nab-paclitaxel trial in 2013 recruited 861 patients, and the NALIRIFOX trial in 2023 recruited 770 patients.
Secondly, many clinical trials have shifted to using progression-free survival (PFS) as the primary endpoint. Moreover, over the years, there has been no significant improvement in overall survival (OS). However, trial conclusions have been framed in an optimistic light around marginal benefits.
Real-world research data from the Netherlands shows that, compared to the period between 1989 and 1993, the 5-year survival rate for newly diagnosed metastatic pancreatic cancer patients in 2014–2018 improved by only 1%. These figures indicate that over the past 20-plus years, our effective efforts for pancreatic cancer patients have been too few.
"Innovation should not be pursued for its own sake; rather, commercial benefits should be gained on the basis of truly helping patients."
Conducting more clinical trials and accumulating more clinical evidence in order to identify the benefiting populations from different regimens is a lengthy phase, which will inevitably involve a process of trial and error.
First is the combination of immunotherapy. Due to the dense immunosuppressive microenvironment of pancreatic cancer, the efficacy of single-agent immunotherapy is limited, requiring combination therapy. The industry's exploration in this area has never stopped.
At the 2023 American Society of Clinical Oncology (ASCO), the European Association for Gastroenterology and Oncology (AGEO) presented research on the use of immune checkpoint inhibitors (ICIs) in patients with advanced pancreatic cancer, as well as a study on the combination therapy of Surufatinib + Camrelizumab + Nab-paclitaxel + S-1 (NASCA), both showing promising results. Although these were small-sample retrospective studies, they provided some clinical evidence for combination therapies and laid a solid foundation for future large-scale research.
Next is targeted therapy. Although the research progress of targeted therapy for pancreatic cancer has been slow, there have been recent breakthroughs. At the end of February, a new drug for pancreatic ductal adenocarcinoma patients, IMM-1-104, received Fast Track designation from the FDA, which will accelerate the drug's development and market approval process.
IMM-1-104 is a highly selective small-molecule MEK inhibitor that stands out among anticancer drugs due to its unique mechanism of action, which deprives tumor cells of growth signals while protecting healthy cells. Currently, clinical trials of IMM-1-104 are underway, targeting not only pancreatic cancer but also malignant cutaneous melanoma and non-small cell lung cancer (NSCLC), among others.
In addition, good progress has been made in the targeted treatment of KRAS G12C mutations in pancreatic cancer, with drugs already available overseas. In China, Jacobio Pharmaceuticals presented clinical data of its KRAS G12C inhibitor JAB-21822 for the treatment of pancreatic cancer and other solid tumors at the 2024 American Society of Clinical Oncology (ASCO) Gastrointestinal Cancers Symposium, achieving positive results.
The proportion of KRAS G12C mutations in pancreatic cancer accounts for only 1% to 2%. Drugs targeting KRAS G12D, which has a higher mutation rate (approximately 41%), are currently still in Phase 1 clinical trials. Only when there is a breakthrough in targeted therapies for KRAS G12D or even pan-KRAS mutations, will it likely be the time when targeted therapy for pancreatic cancer truly gains momentum.
At the end of 2023, Yoson Genehealth announced a global exclusive licensing agreement with AstraZeneca for the UA022 project, a small molecule candidate drug targeting the KRAS G12D mutation at the preclinical stage. Just before this deal was announced, Hengrui Pharma presented research data on its KRAS G12D inhibitor HRS-4642 at the European Society for Medical Oncology (ESMO) conference, also showing promising results.
Finally, there are ADC drugs, which have been developing rapidly in the past two years. Previously, HER2 ADC drugs have achieved good efficacy in fields such as breast cancer, gastric cancer, and biliary tract cancer. However, in pancreatic cancer, the proportion of HER2-positive patients is low, making it difficult for pancreatic cancer to benefit from ADC drugs targeting this site. Recently, clinical research on ADC drugs targeting Claudin 18.2 and TROP2 has been widely carried out.
By the end of 2023, Boan Biotech announced that its innovative ADC drug BA1301 targeting Claudin18.2 received orphan drug designation from the FDA for the treatment of pancreatic cancer. Research has found that Claudin18.2 is expressed in 70% of gastric cancer patients, 50% of pancreatic cancer patients, and 30% of esophageal cancer patients, making it a molecular target with significant potential for anti-tumor drugs. Currently, the drug is in Phase 1 clinical trials in China.
On February 19, AstraZeneca and Daiichi Sankyo announced that the FDA had accepted the marketing application for their new Trop2 ADC drug Datopotamab Deruxtecan, with a PDUFA date set for December 20, 2024. Kelun-Biotech's SKB264 (MK-2870) is also in the NMPA marketing application stage. Additionally, companies including Duality Biologics, Hengrui Medicine, Alkyn Biologics, EpimAb Biotherapeutics, Bio-Thera Solutions, DAC Biotech, Junshi Biosciences, and Baili Pharmaceutical have Trop-2-targeted ADC products in clinical stages.
Although pancreatic cancer is not currently included in the indications for Trop-2 ADC drugs, the Trop-2 protein is also highly expressed in pancreatic cancer. Perhaps in the future, ADC drugs based on these targets will carve out a niche in the field of pancreatic cancer.
From Basic Research to Clinical Trials, the Development of Pancreatic Cancer Drugs is Rapid, Entering an Era of Flourishing Diversity. Building upon past first- and second-line treatments as well as maintenance therapies, continuous advancements in molecular biology technology and new drug development have deepened the industry's understanding of the genetic regulation and microenvironment involved in the onset and progression of pancreatic cancer. Immunotherapy and targeted treatments are gradually entering the field of pancreatic cancer, bringing new hope.
References:
DOI:10.1016/S1470-2045(23)00516-8
DOI:10.1200/JCO.23.01895
DOI:10.1200/JCO.21.02514
G12C–Mutated Advanced Pancreatic Cancer[J]. New England Journal of Medicine, 2023
Pancreatic cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up[J].Ann Oncol,2023,2023,34(11):987-1002.