Case Report by Professor Liao Dan's Team: Combined Mechanical and Pharmacological Approach for Refractory Intimal Hyperplasia in AVF Stenosis

DK Medtech
Vascular Interventional Balloon Product Developer


Stenosis of autologous/artificial arteriovenous fistula (AVF/AVG) is the most common complication in hemodialysis patients. Percutaneous transluminal angioplasty (PTA) has become the primary method for maintaining dialysis access. However, the blunt and irregular tearing of the intima and part of the media by traditional balloons during PTA excessively damages the endothelial vessels, causing intense proliferation of vascular smooth muscle cells and macrophages, which rapidly leads to restenosis.
In recent years, there has been continuous international exploration and clinical research on drug-coated balloons for PTA treatment of dialysis access. DK Medtech has developed the Dissolve™ AV Scoring Drug Balloon, which integrates three features: "scoring," "high-pressure," and "drug-coating," as the world's first third-generation drug balloon:
Directional Scoring: Uniform and regular tearing of the intima to reduce damage from blunt splitting.
High Burst Pressure: For high-resistance lesions, improving technical success rate.
Paclitaxel Coating: Effectively Inhibits Excessive Proliferation of Smooth Muscle Cells.
DK MedtechSpecially launched[Mianyang Central Hospital - Professor Liao Dan's Team: A Case of AVF Refractory Intimal Hyperplasia and Stenosis - Soft and Hard Combined] Case Presentation, demonstrating the meticulous operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized intraoperative procedures and technical applications, complication prevention, perioperative management, and other aspects, the aim is to promote the standardization of diagnosis and treatment for hemodialysis access stenosis, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for the future diagnosis and treatment of hemodialysis access, benefiting more clinical patients.

Combination of Soft and Hard
A Case of Refractory Intimal Hyperplasia and Stenosis in AVF
Liao Dan, Mianyang Central Hospital

Patient Information
Basic Information:Male, 57 years old.
Chief Complaint:More than 5 years of maintenance hemodialysis, poor fistula function for over 10 days.
History of Present Illness:More than 5 years ago, the patient was diagnosed with "uremia" at another hospital and underwent the creation of an autologous arteriovenous fistula in the left forearm. After the fistula matured, maintenance hemodialysis treatment was initiated and has continued to the present. During this period, poor blood flow in the fistula was noted, and the patient underwent multiple "fistula balloon dilation procedures." About 10+ days ago, during dialysis, the patient noticed reduced blood flow and reported a weakened thrill upon palpation, with only slight pulsation and thrill detectable. For further diagnosis and treatment, the patient visited our hospital and was admitted to the department with a diagnosis of "arteriovenous fistula stenosis."
Past Medical History:A history of "hypertension" and "diabetes" for over 10 years, regular dialysis treatment (multiple instances of poor blood flow were found during weeks 1, 3, and 5, underwent "fistula balloon dilation"). Denies history of trauma, blood transfusion, and drug/food allergies.
Physical Examination:Visual Examination: A longitudinal surgical scar approximately 2.5 cm in length is visible 2 cm above the transverse wrist crease on the left upper limb. Two puncture scars with pigmentation are visible on the forearm, without obvious tumor-like dilation or skin lesions. Palpation: Normal skin temperature on both upper limbs; a distinct pulse and weak thrill can be felt at the arteriovenous fistula anastomosis site and 3 cm above it. Auscultation: A unidirectional blowing murmur can be heard at the arteriovenous fistula anastomosis site, and a high-pitched blowing murmur can be heard approximately 3 cm above the anastomosis.
Admission Diagnosis:
Stenosis of Arteriovenous Fistula;
Chronic Kidney Disease Stage 5;
Type 2 Diabetes;
Hypertension Grade 3, Very High Risk.
Previous interventional treatment
Time | Main Treatment Process |
2019.6 | Left Upper Limb Autologous Arteriovenous Fistula |
2020.4 | Stenosis of arteriovenous fistula in the left upper limb, underwent PTA treatment (specific balloon usage unknown) at another hospital. |
2021.6 | Stenosis of arteriovenous fistula in the left upper limb, underwent PTA treatment (specific balloon usage unknown) at another hospital. |
2022.6 | Thrombosis of arteriovenous fistula in the left upper limb, underwent PTA treatment (specific balloon usage unknown) at another hospital. |
2022.12 | Stenosis of arteriovenous fistula in the left upper limb, underwent PTA treatment (specific balloon usage unknown) at another hospital. |
2023.4 | Stenosis of arteriovenous fistula in the left upper limb, underwent PTA treatment (specific balloon usage unknown) at another hospital. |
2023.7 | Thrombosis of arteriovenous fistula in the left upper limb with Type I stenosis, treated with PTA (high-pressure balloon 5*40mm + 6*40mm). |
2023.10 | Left Upper Limb Arteriovenous Fistula with Type I Stenosis, Treated with PTA (High-Pressure Balloons 4*40mm + 6*40mm) |
Preoperative Analysis
Preoperative Analysis:The patient has a lesion in the arteriovenous fistula of the left upper limb, with intimal hyperplasia and stenosis, and has undergone PTA treatment seven times in the past. The last PTA treatment only lasted for three months, and changing the treatment method is required to improve the therapeutic effect for further expansion. This time, the use of a scoring drug-coated balloon is considered.
Surgical Objective:
Main Objectives:Addressing the issue of insufficient patient flow by increasing vascular diameter through PTA treatment with a scored drug-coated balloon.
Secondary Objective:Extend the interventional interval for patients, reduce the number of interventions, suppress intimal hyperplasia, and improve the patency rate of fistulas.
Surgical Strategy/Plan:
Percutaneous Transluminal Angioplasty of Left Upper Limb Arteriovenous Fistula Under B-mode Ultrasound Guidance (Dissolve™ AV).
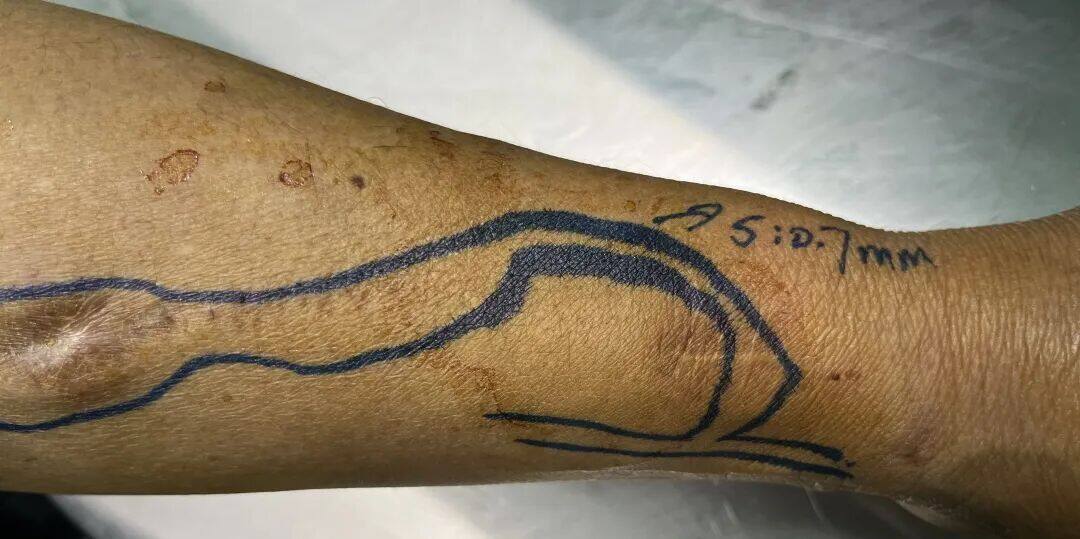
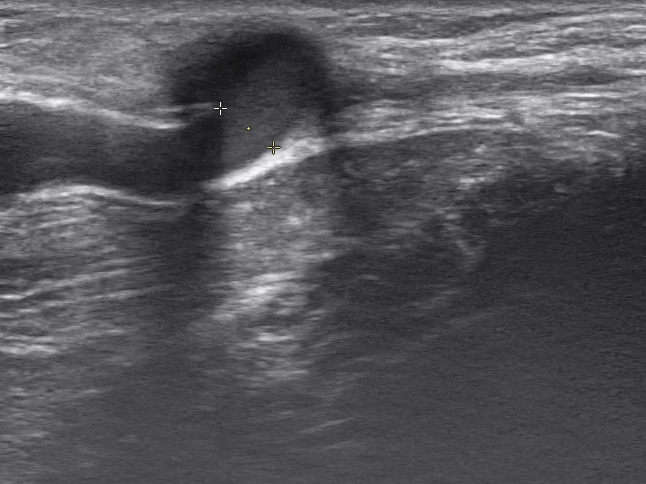
S:0.7mm
S: 0.7mm; Length 29mm
Proximal A Diameter 3.2mm
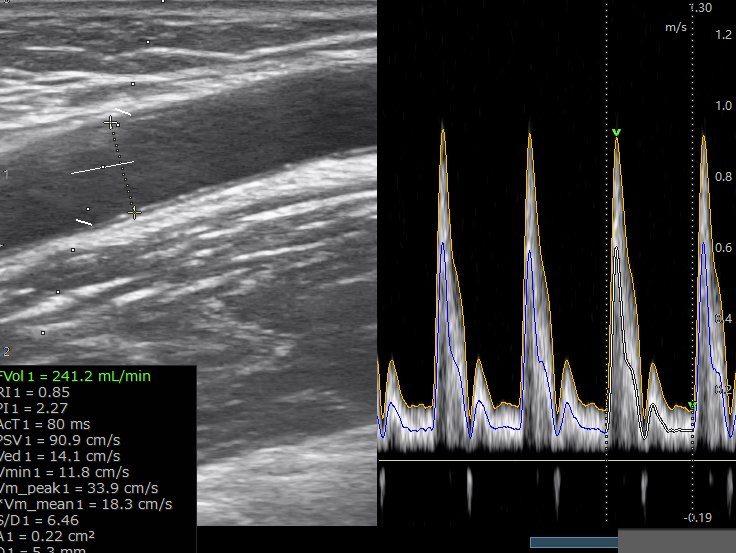
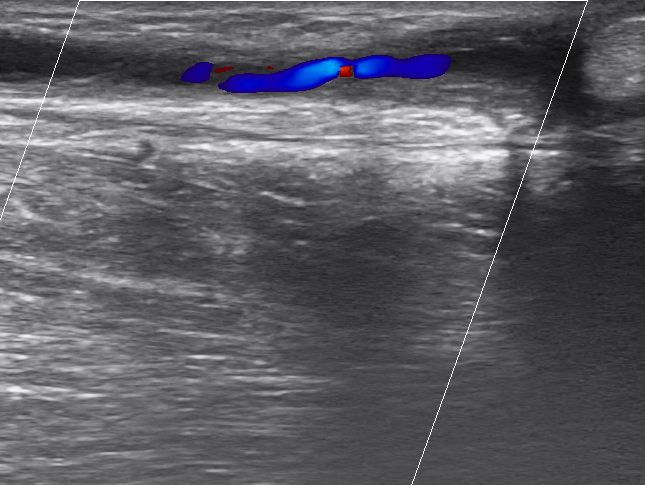
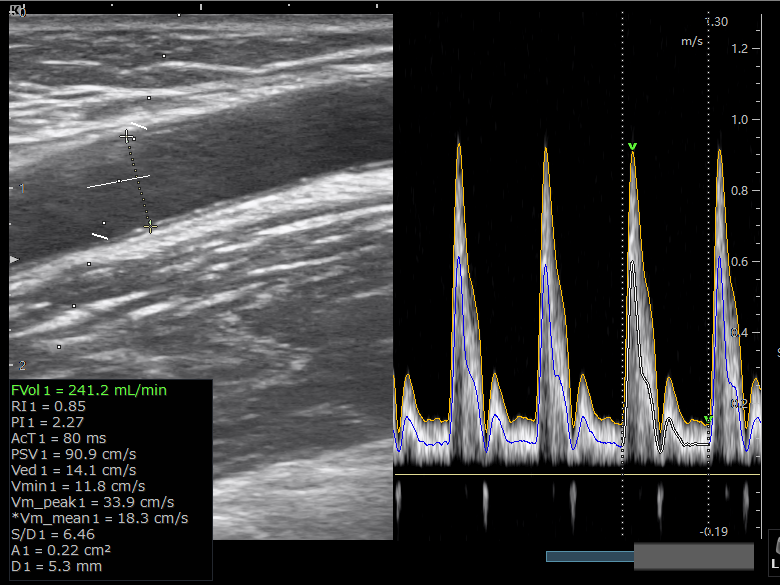
Preoperative brachial artery flow: 241.2 ml/min, RI: 0.85
Surgical Procedure

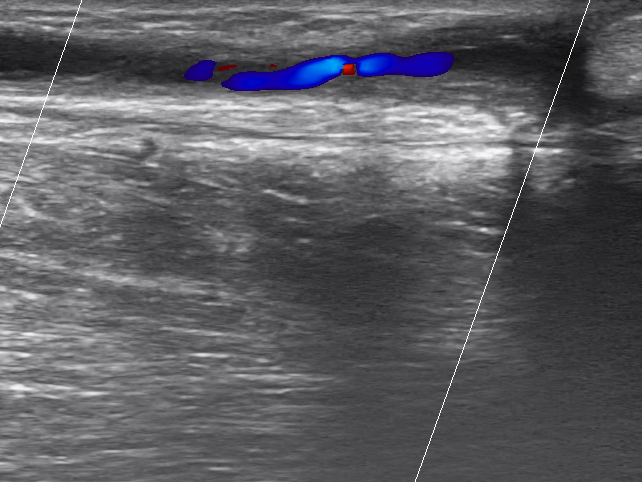
Under color Doppler ultrasound guidance, the antecubital vein was punctured against the blood flow to establish access. After successful puncture, a 7F vascular sheath was inserted.
The guidewire passes through the stenotic segment of the vessel and enters the proximal radial artery.

Prepare a 6mm×6cm scored drug-coated balloon (DK Medtech Dissolve™ AV) with heparin saline flush.
A scoring drug balloon (DK Medtech Dissolve™ AV) was inserted through the vascular sheath, and the balloon was expanded at the stenotic site for 3 minutes. After the balloon was withdrawn, the effect of lesion vessel dilation was evaluated.
Postoperative Effect

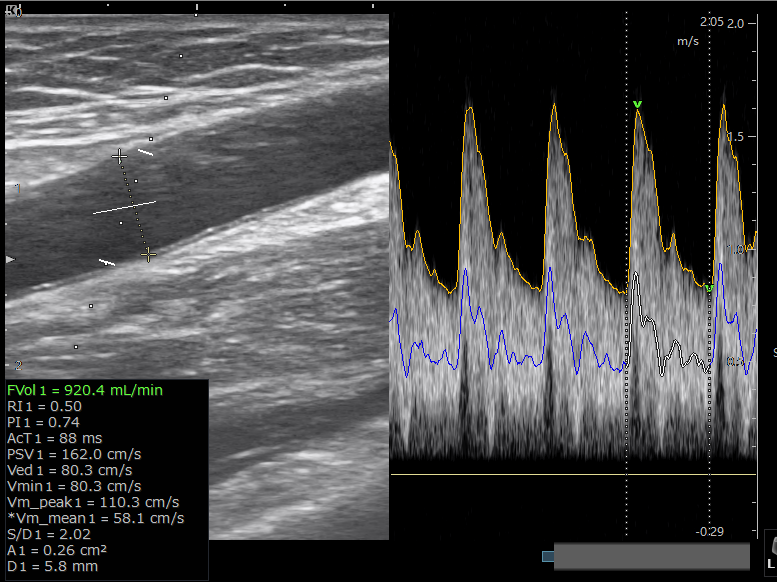
After treatment with the scored drug-coated balloon (DK Medtech Dissolve™ AV), the patient's stenosis site expanded from 0.7mm to 4.1mm; brachial artery flow increased from preoperative: 241.2ml/min, RI: 0.85, to 920.4ml/min, RI: 0.5.
Follow-up
Discharge Status:Postoperative arteriovenous fistula showed good thrill, no abnormal pulsation was palpated. After discharge, the patient returned to the local area for dialysis with a flow rate of 240 ml/min. No pain or inadequate flow at the fistula site was reported during dialysis. The patient was instructed to return to the hospital for reexamination one month after the surgery.
Case Summary
Case Characteristics:The patient has Type I stenosis of the arteriovenous fistula in the left upper limb, accompanied by intimal hyperplasia. The patient has previously undergone PTA treatment seven times, with the last dilation lasting for 3 months.
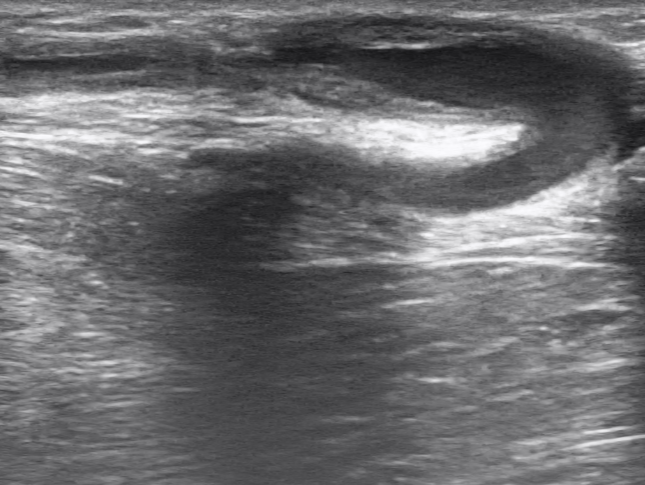
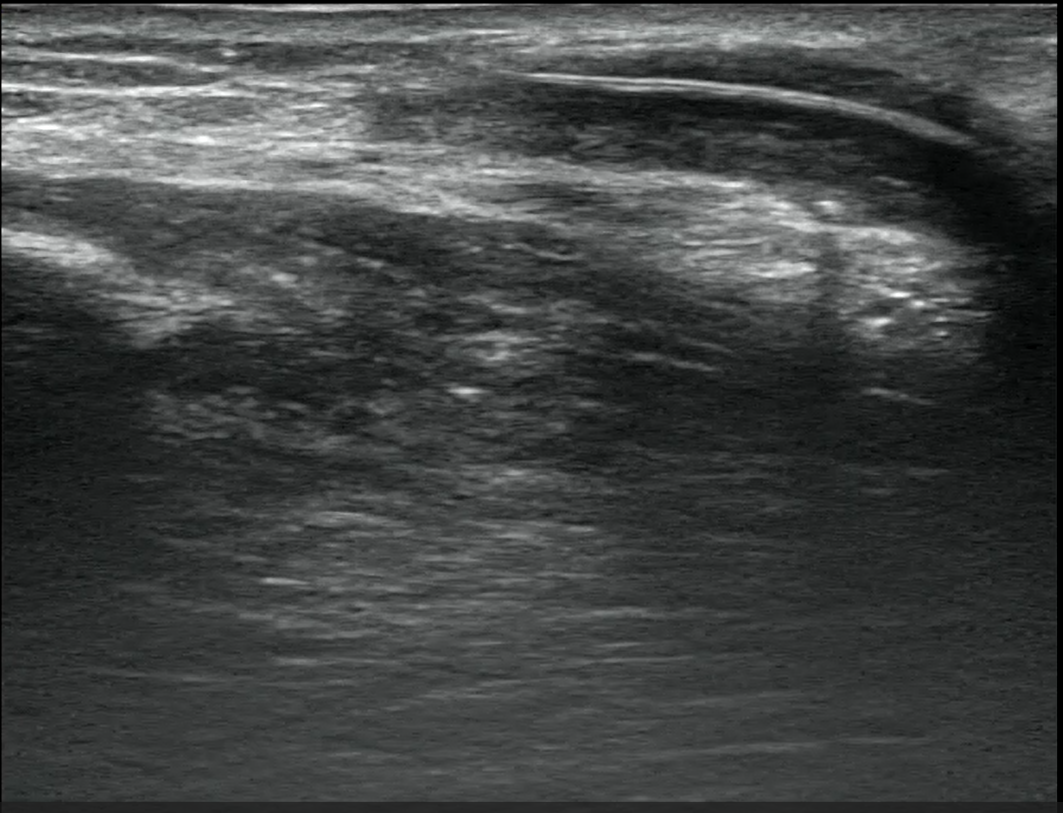
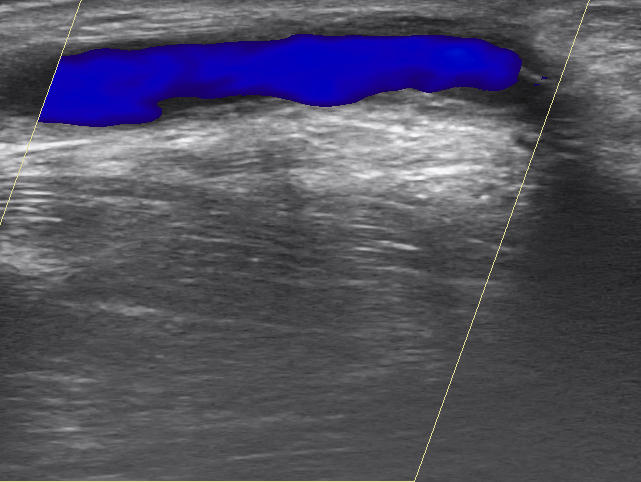
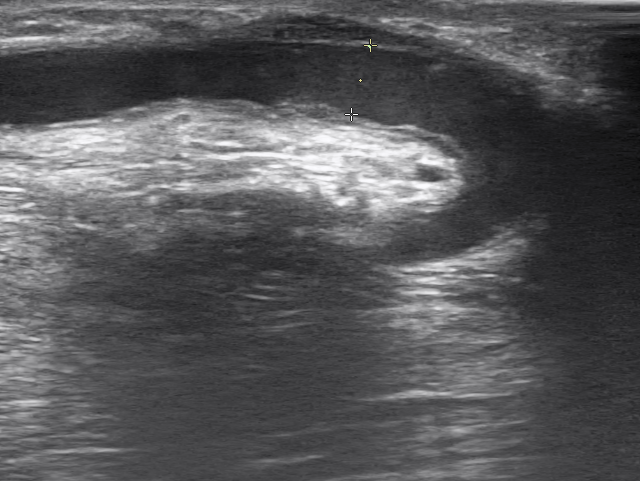
Preoperative Assessment Key Points:Preoperative Assessment and Reasonable Surgical Planning for Intimal Hyperplasia of the Patient's Fistula Vessel. Preoperative ultrasound evaluation: proximal artery inflow diameter 3.2mm, anastomosis diameter 4.7mm, normal outflow tract diameter 5.1mm, brachial artery blood flow.241ml/min. Color Doppler ultrasound showed that the left upper limb was narrowed 3 cm away from the anastomosis, with the narrowest inner diameter of about 0.7 mm and intima thickness of 2.1 mm.
Surgical Strategy/Technical Key Points:
To fully dilate the hyperplastic intima, inhibit postoperative intimal hyperplasia, and address calcified stenotic lesions, the Dissolve™ AV scoring drug-coated balloon is the optimal choice due to its high-pressure, scoring, and drug-coated advantages.
In April 2020, this patient underwent balloon angioplasty for arteriovenous fistula stenosis. The effect was not ideal after high-pressure balloon dilation, and multiple restenosis recurred shortly after the surgery.
The AV Peripheral Scoring Balloon Dilation Catheter, in addition to having high-pressure characteristics, features scoring elements on its surface that provide a pressure-focusing scoring effect. This enables effective and precise incision of the intima and fibrous ring, enhancing dilation efficiency and increasing lumen gain. The balloon surface is coated with paclitaxel, which effectively inhibits intimal hyperplasia at the lesion site, improving long-term patency rates.
In this case, it can be seen that the lesion was fully opened when pressurized to 19atm.
Characteristics/Usage Tips of the Device:
Preoperative balloon needs only to be flushed with saline in the balloon catheter lumen, avoiding soaking the balloon end to prevent drug loss.
Without removing the coating protective sleeve, advance the balloon along the guidewire to the sheath opening until it is locked at the sheath opening;
The AV Peripheral Scoring Balloon Dilation Catheter is equipped with three nickel-titanium alloy triangular scoring elements on its surface and features a paclitaxel drug coating on the balloon surface. After achieving adequate dilation of the lesion, paclitaxel is utilized to inhibit the proliferation of the intima. In this case, after using the balloon once, the balloon was rotated approximately 60 degrees and then used again to dilate the lesion, allowing for more comprehensive expansion treatment of the stenotic lesion.
This case adopts a 3-minute pressure retention this time, allowing for better drug adherence.

Expert Introduction


Dr. Liao Dan, Associate Chief Physician
Surgeon of This Case
Mianyang Central Hospital,M.D., Associate Chief Physician, Master's Supervisor,Secretary of the Party Branch and Director of the Nephrology Department;The 14th batch of reserve candidates for academic and technical leaders in Sichuan Province;Reserve Candidate for Academic and Technical Leader of Sichuan Provincial Health Commission;Member of the Vascular Access Group, Blood Purification Branch, China Hospital Management Association;Member of the Vascular Access Intervention Group of the Ultrasound Intervention Professional Committee of the Interventional Physicians Branch of the Chinese Medical Doctor Association;Youth Committee Member of the Nephrology Professional Committee of the China Association of Traditional Chinese Medicine;Vice Chairman of the Nephrology Professional Committee of the Sichuan Provincial Association of Rehabilitation Medicine;Standing Committee Member of the Nephrology Specialty Committee of the Sichuan Medical Association;Member of the Vascular Access Group, Sichuan Province Medical Doctor Association;Deputy Group Leader of the Vascular Access Group, Sichuan Medical Promotion Association;Chairman of the Nephrology Professional Committee of the Mianyang Medical Association.
Successively at Haidian Hospital in Beijing, China, St. Martin's Hospital in Taiwan, China, and Hammersmith Hospital affiliated with Imperial College London, UKSmith Hospital Internship,Awarded the Third Prize of Sichuan Medical Science and Technology Award for 2 items, and the First Prize of Mianyang Medical Technology Best Promotion Award.Third Prize of Mianyang Medical Science and Technology, Outstanding Physician of Mianyang;First author or corresponding author published 13 SCI papers and 8 Chinese core journal articles;Associate Editor, contributed to "Internal Medicine Diagnosis"; holds 2 utility model patents.
Zhang Fenglian, Attending Physician
Surgeon of This Case
Mianyang Central Hospital, Master's Degree,Attending Physician in Nephrology.
Graduated from Luzhou Medical College;Once studied at Beijing Haidian Hospital for half a year.
Proficient in the establishment and maintenance of vascular access for uremic patients, such as autologous arteriovenous fistula surgery and balloon dilation; management of blood purification complications; diagnosis and treatment of various chronic glomerulonephritis, nephrotic syndrome, diabetic nephropathy, etc.
Vascular Access Committee Member of the 2nd Nephrology Specialized Committee, Chengdu High-Tech Medical Association.
First author or corresponding author published 1 SCI paper and several Chinese journal articles.

Department Introduction


The Department of Nephrology at Mianyang Central Hospital was established in 1994. It is a professional department integrating clinical practice, teaching, and research. The department currently has 80 beds, 61 hemodialysis machines, 10 hemofiltration machines, 5 CRRT machines, and 2 automated peritoneal dialysis machines. The department has 97 medical staff members, including 18 doctors (5 chief physicians, 2 deputy chief physicians, 7 attending physicians, 3 resident physicians, 3 doctors with a Ph.D., and 9 with a master's degree) and 79 nurses (30 in the nephrology ward and 49 in the hemodialysis center).
Medical Technology: Capable of treating refractory nephrotic syndrome, various glomerular diseases, tubulointerstitial lesions, acute renal failure, chronic renal failure, and various toxic diseases. Regularly conducts hemodialysis, hemodiafiltration, hemoperfusion, plasma exchange, continuous bedside blood purification, CRRT endotoxin adsorption technology, arteriovenous fistula surgery, ultrasound-guided balloon dilation, artificial blood vessels, giant aneurysm resection, peritoneal dialysis, renal pathological biopsy, thrombolysis, blunt needle buttonhole puncture technology, etc. Accumulated successful experience in complex and difficult vascular access. The department emphasizes discipline construction, talent cultivation, and internal development. It is a key specialty construction unit of Sichuan Province (Grade A), a construction unit of the Sichuan Kidney Disease Diagnosis Clinical Medical Research Center, a network member unit of the National Kidney Disease Clinical Medical Research Center, a key discipline of Mianyang City (Grade A), the director unit of the Mianyang Nephrology Committee, the Standardized Dialysis Construction Center of the Zhongguancun Nephropathy and Blood Purification Innovation Alliance, the Ingenuity Skills Studio, established the Northwest Sichuan Nephropathy Specialty Alliance consisting of 36 units, the group leader unit of the Mianyang Kidney Disease Quality Control Center, and the supporting unit of the Blood Purification Nursing Specialty Committee of the Mianyang Nursing Association. It has been awarded the Outstanding Sub-center of the Sichuan Kidney Disease Quality Control for five consecutive years and ranks among the top in terms of academic influence in Sichuan Province.
Copyright Statement: This platform aims to help healthcare professionals better understand the latest developments in relevant disease areas. The information published on this platform does not imply agreement with its descriptions or viewpoints, but is merely intended to provide more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will address them as soon as possible. The information is solely for healthcare professionals to stay informed, and such information cannot replace professional medical guidance in any way, nor should it be regarded as medical advice. If such information is used for purposes other than staying informed, this platform and the author shall not bear any related responsibilities.Contact Email for Cooperation:vascular@edoctor.work。
