Dingli Xiangzhu | Professor Jiang Jinquan's Team: Restoring Blood Flow, Healing Ulcers with DKutting™ Scoring Balloon

DK Medtech
Vascular Interventional Balloon Product Developer

With the vigorous development of China's peripheral vascular intervention market, ordinary peripheral balloons have entered a stage of full competition. However, for the increasing number of highly resistant stenotic lesions, ordinary balloons tend to cause complications such as excessive vascular injury, flow-limiting dissections, and hematomas. On the other hand, pressure-focusing balloons, which utilize cutting/notching elements between the inner wall of the blood vessel and the outer diameter of the balloon during expansion, enhance localized pressure and enable efficient directional dilation. This reduces vascular elastic recoil and represents a new direction in the development of vascular intervention balloons.
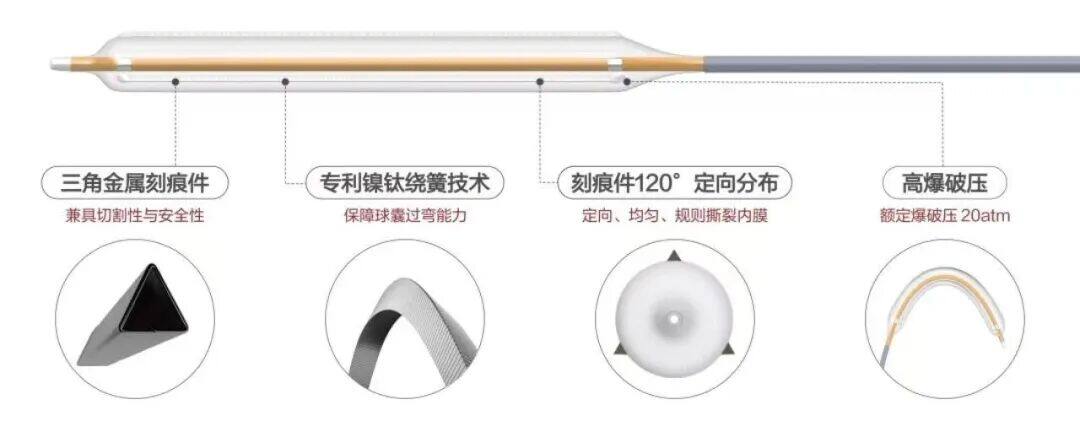
DK Medtech's independently developed DKutting™ High-Pressure Scoring Balloon, featuring an exclusive patented design (CN201810478242.X), boasts numerous advantages such as excellent deliverability, uniform expansion, and high burst pressure. In terms of overall product performance, it can be called a "hexagonal warrior" with almost no weaknesses. This marks a significant breakthrough for local enterprises in innovating and surpassing top-tier imported products.
DK Medtech Special Release[Professor Jiang Jinquan's Team: Blood Circulation Operation, Effective Treatment for Ulcers] Case Presentation, demonstrating the meticulous operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized intraoperative procedures and technical applications, complication prevention, to perioperative management, etc., the aim is to promote the standardization of diagnosis and treatment for vascular stenosis and occlusive diseases, enhance technical exchange and experience sharing among doctors, with the hope of providing new ideas and methods for future diagnosis and treatment, benefiting more clinical patients.

Promoting Blood Circulation, Healing Sores with Skill
Jiang Jinquan, First Hospital of Northwest University

Patient Information
Basic Information:Elderly female, 66 years old, from Heyang, Weinan, Shaanxi Province.
Chief Complaint:Ulcer pain in the left lower limb for more than 1 year.
History of Present Illness:Formation of Ulcer on the Left Lower Limb for Over a Year. Present Illness: The patient developed skin ulceration on the left lower limb after scratching it one year ago. There was no improvement after visiting a local clinic, and subsequently, the ulcer gradually expanded and deepened with significant pain. Obvious swelling occurred below the knee joint of the left lower limb, and the skin could not heal. One month ago, the patient visited the wound clinic of our hospital and received local dressing changes and intravenous anti-infection treatment, but the effect was not significant. Lower limb arterial occlusion was considered as a possibility. For further treatment, the patient was admitted to the hospital with a diagnosis of "Lower Extremity Arteriosclerosis Obliterans? Ulcer on the Left Lower Limb." Since the onset of the disease, the patient has been conscious, in good spirits, with normal appetite, sleep, and bowel/bladder function.
Past Medical History:History of "hypertension" for over 10 years, with the highest blood pressure reaching 180/100 mmHg. Currently taking "nifedipine sustained-release tablets and nimodipine tablets" for antihypertensive treatment; blood pressure has not been systematically monitored. Denies history of chronic diseases such as "coronary heart disease, diabetes, cerebral infarction," denies history of acute or chronic infectious diseases such as "hepatitis, tuberculosis," and denies history of surgery, trauma, or blood transfusion. Immunization history is unclear. Denies history of food or drug allergies.
Physical Examination:A large area of ulceration can be seen on the inner side of the left calf, reaching the muscular layer, with purulent coating covering the surface and a significant amount of purulent discharge. The area is approximately 10*9 cm in size. The skin temperature below both knees is low; the pulse of the left popliteal artery cannot be palpated, and the pulse of the left dorsalis pedis artery is weak.
Admission Diagnosis:
Atherosclerotic Occlusion of Both Lower Limb Arteries with Large Ulcer on Left Calf;
Hypertension.
Previous interventional treatment
Time | Main Treatment Process |
In the past year | The wound dressing was changed at multiple outpatient clinics both in other hospitals and in our hospital, but the wound did not show significant improvement, and the ulcer area continued to enlarge. |
Preoperative Analysis
Preoperative Analysis:CTA of the patient showed occlusion of the distal left superficial femoral artery and popliteal artery. The wound had long failed to heal and continued to worsen, with poor blood supply to the wound area. There were indications for recanalization of the distal left superficial femoral artery and popliteal artery to restore blood flow. The main skin ulcer was located on the calf, where the wound was primarily supplied by the peroneal artery or collateral circulation from the dominant anterior and posterior tibial arteries. Based on angiography findings, consider selectively dilating the left peroneal artery. The patient had a history of left lower limb ischemia for over a year, making recanalization potentially difficult. Atherosclerotic plaques were found in multiple vessels of both lower limbs, some with calcification. If necessary, retrograde puncture of the anterior tibial artery might be required to open the occluded segment.
Surgical Objective:
Main Objectives:Open the distal superficial femoral artery and popliteal artery of the left lower limb to restore blood supply;
Secondary Objective:Discretionary dilation of the left peroneal artery to promote wound healing.
Surgical Strategy/Plan:Angiography of the Left Lower Limb Artery + Balloon Dilatation + Thrombus Aspiration.
Preoperative CTA:Occlusion of the distal left superficial femoral artery and popliteal artery, with collateral circulation formed between the distal segment of the superficial femoral artery and the popliteal artery; multiple plaques and stenoses in bilateral femoral arteries, popliteal arteries, anterior tibial arteries, and posterior tibial arteries; proximal stenosis and partial occlusion of the left peroneal artery, with collateral circulation formed due to occlusion of the right peroneal artery and anterior tibial artery.
Surgical Procedure

Occlusion of the distal left superficial femoral artery and popliteal artery, with collateral circulation formed between the distal segment of the superficial femoral artery and the popliteal artery; multiple plaques and stenoses in the bilateral femoral arteries, popliteal arteries, anterior tibial arteries, and posterior tibial arteries; proximal stenosis and partial occlusion of the left peroneal artery, with collateral circulation formed due to occlusion of the right peroneal artery and anterior tibial artery.

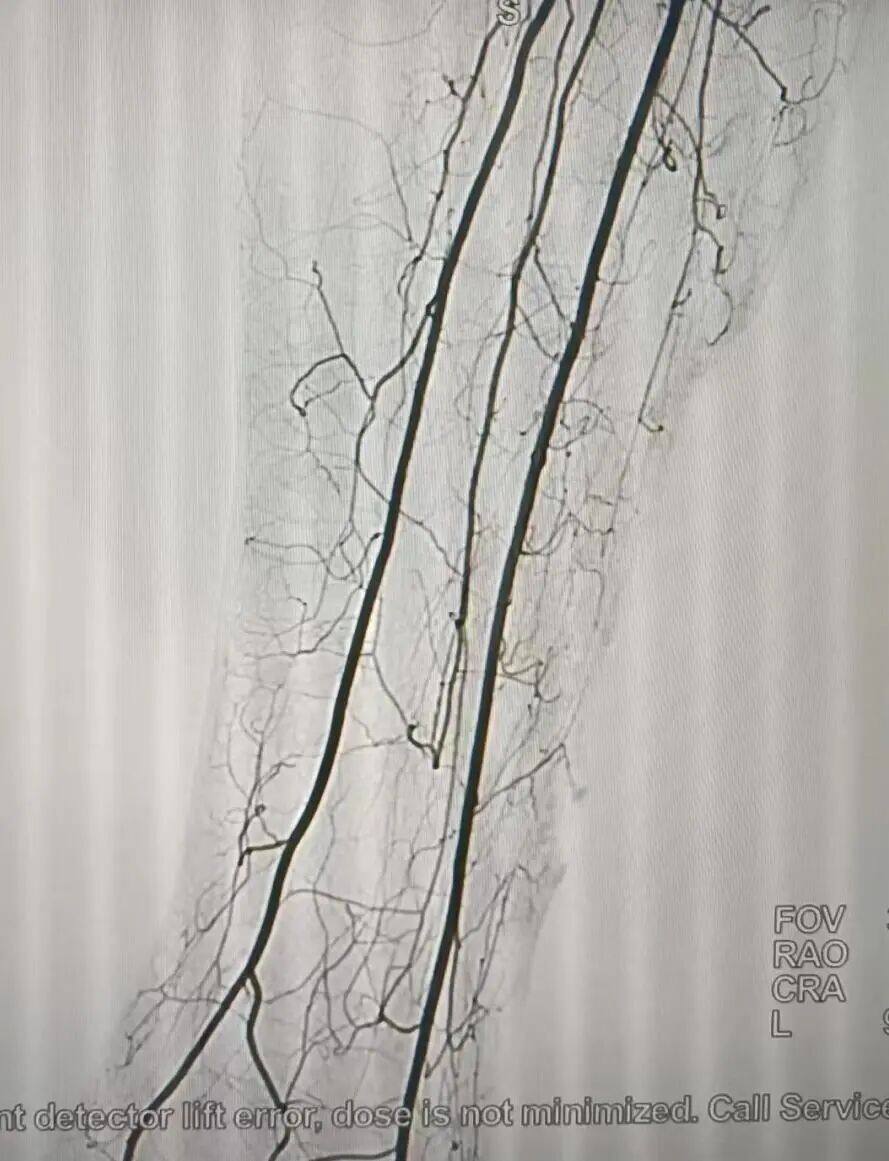
Preoperative angiography showed occlusion of the distal left superficial femoral artery and popliteal artery, multiple stenoses in the superficial femoral artery, and collateral circulation formation between the distal segment of the superficial femoral artery and the popliteal artery.

Preoperative wound condition: poor blood circulation in the wound tissue, non-healing; after months of dressing changes, no significant formation of fresh granulation tissue at the wound edges, and after debridement, there is still pus and necrotic tissue.

One week after the surgery, the blood supply of the wound had significantly improved, with new granulation tissue forming, wound edges rising, and the wound area shrinking; the purulent coating was relatively easy to clean, and obvious bleeding occurred during debridement.

The patient had vascular calcification. After using a 4mm*8cm DKutting™ high-pressure scoring balloon to dilate the distal superficial femoral artery and popliteal artery, although some of the stenotic segments were difficult to expand due to hard calcification and residual stenosis remained, the blood flow velocity was acceptable, achieving the surgical goal. If a stent were used here, although luminal gain would be achieved, stent fracture could very likely occur postoperatively due to the movement of the patient’s knee joint.
After using a 4mm*8cm DKutting™ high-pressure scoring balloon to dilate the occluded segment, no dissection was formed, and blood flow below the knee was significantly improved compared to before. Although the patient's peroneal artery is slender, both the anterior and posterior tibial arteries branch extensively in the calf; therefore, there is no need to further dilate the slender peroneal artery.
Follow-up
Discharge Status:At discharge, the patient had good pulsation of the left popliteal artery, significantly increased skin temperature of the left lower limb, and notably improved pain in the left lower limb. The wound was dressed at discharge.The blood circulation in the wound has significantly improved, with new granulation tissue forming, the wound edges are raised, and the wound area has decreased; the pus coating is relatively easy to clean, and there is noticeable bleeding during debridement.
Discharge Instructions:
Continue to change the dressing at our hospital's wound clinic.
Continue oral administration of aspirin 100mg/day; atorvastatin calcium tablets 20mg/day; rivaroxaban 15mg/day.
Follow-up after discharge:Two weeks after discharge, the patient underwent VSD negative pressure wound therapy at our hospital's wound clinic. The purulent coating on the wound had further decreased compared to before, and new granulation tissue had further increased. Due to the large size of the wound, the subsequent healing process will require a longer time. Skin grafting can be considered once the wound shows further improvement.
Case Summary
Case Characteristics:The patient has had long-term occlusion of the left lower limb artery, with the occluded segment occurring at the distal end of the superficial femoral artery and the popliteal artery. Due to ischemia of the tissue below the knee, the wound has been expanding over the past year and has not healed for a long time despite active dressing changes.
Preoperative Assessment Key Points:The patient's left lower limb artery has been occluded for a long time, which may make it difficult to open or result in poor vascular bed conditions after opening, with severe calcification, and may become occluded again after opening; moreover, it is best not to implant a stent at the popliteal artery.。
Surgical Strategy/Technical Key Points:Use the V18 guidewire to achieve true lumen opening as much as possible; use the DKutting™ high-pressure scoring balloon to dilate the occluded segment, restore the lumen, and avoid dissection formation; if there is secondary thrombosis, handle the thrombus properly to prevent thrombus detachment and embolization of distal vessels.
Characteristics/Usage Tips of the Device:The scored balloon effectively dilated the occluded segment, restoring the lumen; no dissection formed throughout the procedure, especially in the popliteal artery segment, avoiding the dilemma of whether to use stent implantation.

Introduction of Experts


Jiang Jinquan, Attending Physician
Surgeon of This Case
Attending Physician of the Interventional Radiology Department at the First Hospital of Northwest University;Member of the Intervention Committee of the Shaanxi Medical Communication Association;Member of the Liver Cancer Group, Shaanxi Anti-Cancer Association;Bachelor of Clinical Medicine and Master of Surgery from Xiangya School of Medicine, Central South University; Ph.D. candidate in Medicine at Xi'an Jiaotong University.
曾于西京医院、唐都医院介入手术中心学习血管介入技术;Published 1 SCI article and 4 articles in domestic core journals.

Department Introduction

The current interventional radiology team consists of 2 doctors, 1 technician, and 2 nurses, including 2 members with intermediate professional titles. The team possesses strong technical expertise and has appointed Professor Zhonghua Luo, the standing committee member and secretary-general of the Interventional Branch of the Shaanxi Medical Association and Director of the Interventional Department at Tangdu Hospital, as a guest professor. Additionally, the department has introduced advanced equipment from both domestic and international sources to meet the full range of interventional treatment needs for patients.
Currently, we have one GE Optima IGS 330 Digital Subtraction Angiography (DSA) machine and one GE Voluson E8 Color Ultrasound Diagnostic System.
Copyright Statement: This platform aims to help healthcare professionals better understand the latest developments in relevant disease areas. The information published on this platform does not imply agreement with its descriptions or viewpoints, but is merely intended to provide more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will address them as soon as possible. This information is solely for healthcare professionals to stay informed, and such information cannot replace professional medical guidance in any way, nor should it be considered as medical advice. If such information is used for purposes other than staying informed, this platform and its authors shall not bear any related responsibilities.Contact Email for Cooperation:vascular@edoctor.work。
