Case Report by Prof. Chen Zhiyong & Prof. Zha Binshan: Treating No-Stenting Zone Lesions with DKutting™ Scoring Balloon

DK Medtech
Vascular Interventional Balloon Product Developer

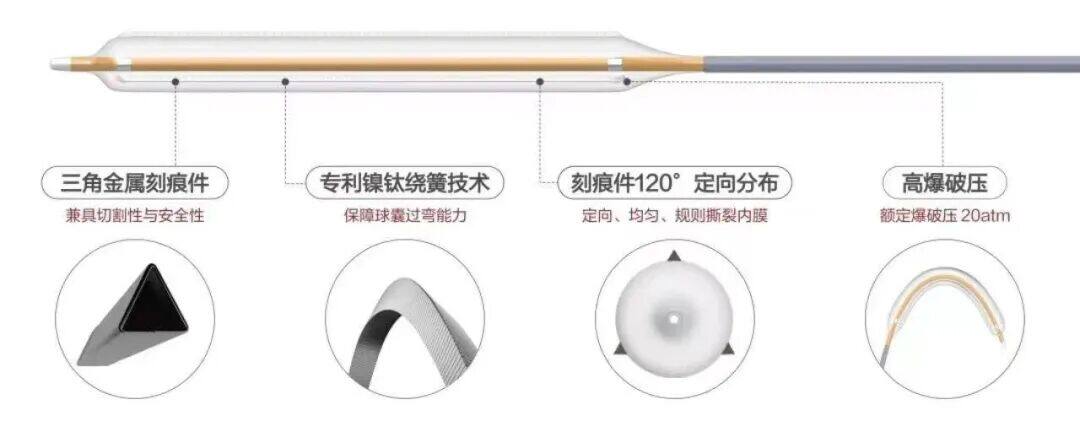
With the vigorous development of China's peripheral vascular intervention market, ordinary peripheral balloons have entered a stage of full competition. However, for the increasing number of highly resistant stenotic lesions, ordinary balloons tend to cause complications such as excessive vascular injury, flow-limiting dissections, and hematomas. On the other hand, pressure-focusing balloons utilize cutting/notching elements positioned between the inner wall of the blood vessel and the outer diameter of the balloon during expansion. These elements enhance localized pressure, enabling efficient directional expansion, thereby reducing vascular elastic recoil and representing a new direction in the development of vascular intervention balloons.。
DK Medtech Special Release【Professor Chen Zhiyong & Professor Cha Binshan's Team: A Case of Scoring Balloon Treatment for No Stenting Zone Lesions】Case Presentation, demonstrating the meticulous operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized intraoperative procedures and technical applications, complication prevention, to perioperative management, etc., the aim is to promote the standardization of diagnosis and treatment for vascular stenosis and occlusive diseases, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for future diagnosis and treatment, benefiting more clinical patients.

A Case of No Stenting Zone Lesion Treated with a Scoring Balloon
The First Affiliated Hospital of Anhui Medical University, Department of Vascular Surgery

Patient Information
Basic Information:The patient is a 79-year-old female.
Chief Complaint:Intermittent claudication of the right lower limb for half a year, worsened in the past 10 days.
History of Present Illness:The patient developed intermittent claudication six months ago, with a claudication distance of approximately 500 meters. Two months ago, due to acute pain in the left lower limb, the patient underwent left lower limb arteriography + catheter thrombectomy of the left femoral-popliteal artery + PTA of the popliteal artery, anterior tibial artery, peroneal artery, and tibiofibular trunk. In the past 10 days, the claudication distance has decreased and the pain has worsened. The patient came to the hospital for further treatment.
Past Medical History:Hypertension, Cerebral Infarction, Atrial Fibrillation.
Physical Examination:No edema in both lower limbs, gastrocnemius muscles are soft, no ulcers or pigmentation, the pulse of the right femoral artery is palpable, but the pulse of the right dorsalis pedis artery is not palpable, skin temperature is lower than the opposite side, and the movement of the right foot is mildly restricted.
Admission Diagnosis:Arteriosclerosis Obliterans of the Right Lower Limb.
Preoperative Analysis
Preoperative Analysis:The patient is an elderly male, mainly presenting with intermittent claudication in the lower limbs. With a long history of illness, lower limb arterial CTA suggests diffuse lesions in the right femoral-popliteal artery and infrapopliteal arteries, consistent with the medical history. The diagnosis of lower extremity atherosclerotic occlusive disease is clear, and endovascular treatment is planned.
Surgical Objective:
Main Objectives:Open Occluded Vessels, Relieve Symptoms;
Secondary Objective:Reduce stent implantation.
Surgical Strategy/Plan:Antegrade puncture and catheterization of the right common femoral artery were performed to clarify the lesion condition by angiography. Appropriate guidewires and catheters were selected based on the lesion condition for endovascular treatment through the lesion segment. Balloon dilation was initially performed, and if sufficient pre-treatment was achieved without flow-limiting dissection and residual stenosis, drug-coated balloon dilation therapy was planned.
Surgical Procedure
Occlusion of the distal superficial femoral artery to the popliteal artery, with poor visualization of the infrapopliteal arteries. An 18-gauge guidewire was used in conjunction with a balloon to pass through the femoropopliteal lesion segment. Angiography simultaneously revealed segmental stenosis and occlusion of the anterior tibial artery and peroneal artery, while the posterior tibial artery showed relatively good visualization.
The anterior tibial artery was dilated with 2.5mm and 3mm balloon catheters, and the lesion segment of the peroneal artery was dilated with a 2.5mm balloon.
No obvious dissection was observed without angiography after 3mm balloon dilation. Then, a 4mm*80mm scored balloon was used for segmental dilation of the popliteal artery and superficial femoral artery. Repeat angiography showed satisfactory luminal gain in the femoral and popliteal arteries, with no obvious dissection or residual stenosis.
A 4mm*150mm Cercor drug-coated balloon was used to dilate the femoral-popliteal artery lesion segment. Post-dilation angiography showed no distal embolism, fast blood flow, satisfactory luminal gain of the femoral-popliteal artery, and no flow-limiting dissection, residual stenosis, or elastic recoil.
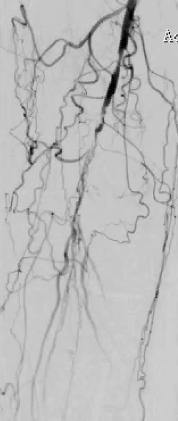
Preoperative Angiography

Postoperative Angiography
Follow-up
Discharge Status:
The next day, the patient got out of bed and walked without lower limb pain or weakness. After 2 days of observation, the patient was discharged and instructed to regularly take oral antiplatelet and statin medications (Aspirin 100mg qd + Rivaroxaban 10mg qd + Atorvastatin 10mg qd).
Repeat CTA after 3 months.
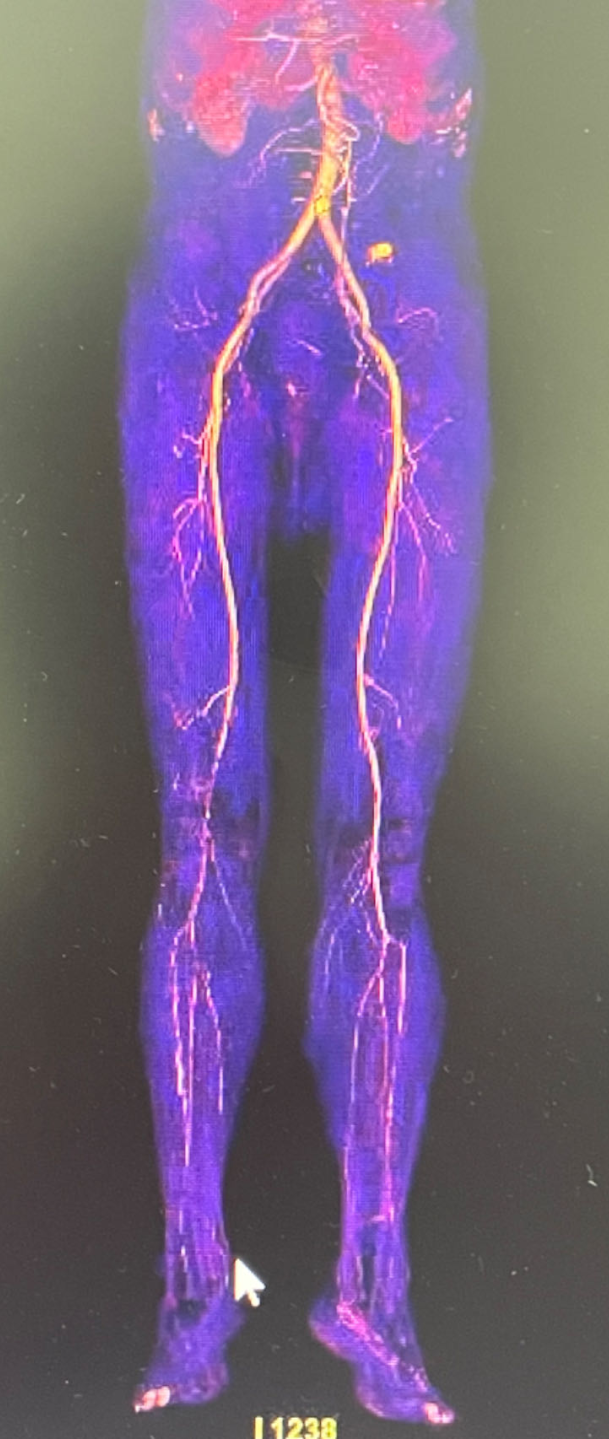
Preoperative

3 Months Post-Operation
Case Summary
Case Characteristics:Diffuse lesions in the femoral-popliteal and infrapopliteal arteries, combined with mild to moderate calcification. The scoring balloon can perfectly achieve expansion in the "No stenting zone," avoiding dissection and elastic recoil. It better modifies the lumen plaque, resulting in satisfactory lumen gain and avoiding stent implantation.
Preoperative Assessment Key Points:Nature and length of the lesion.
Surgical Strategy/Technical Key Points:
The 18-guide wire cooperates with the balloon catheter to pass through the lesion segment in the true lumen as much as possible;
First, select a balloon with a diameter smaller than the target lesion to pre-dilate the lesion segment.
Select a 1:1 balloon for the diseased vessel, with a length that fully covers the lesion;
Low-pressure slow expansion.
Device Features/Usage Tips:The scored balloon was slowly inflated with pressure increasing gradually at 2, 4, 6, and 8 atmospheres, each pressure level maintained for 15 seconds to avoid intimal tearing. The dilation time was over 3 minutes, followed by a careful assessment of the lesion after expansion.

Expert Introduction


Professor Chen Zhiyong
Director of Department Administration
Director of the Vascular Surgery Department at the First Affiliated Hospital of Anhui Medical University, PhD, Associate Chief Physician, Master's Supervisor. Vice Chairman of the Vascular Committee of the Anhui Province Medical Association, Member of the Endovascular Committee of the Chinese Medical Doctor Association, Member of the Abdominal Aortic Specialized Committee of the International Union of Angiology, Standing Committee Member of the Vascular Surgery Committee of the Anhui Medical Association, and Vice Chairman of the VTE Alliance of the Anhui Hospital Association. Specializes in open and endovascular minimally invasive treatments for aortic and peripheral vascular diseases. Has led and participated in four provincial natural science foundation projects, published over 10 papers, and co-authored four monographs.

Professor Binshan Zha
The Surgeon of This Case
Associate Professor, Deputy Chief Physician, Doctor of Surgery, and Master's Supervisor in the Department of Vascular Surgery at the First Affiliated Hospital of Anhui Medical University. Visiting scholar in the Department of Vascular Surgery and Endovascular Surgery at Agaplesion Diakonieklinikum (Rotenburg Wümme), affiliated with the University of Hamburg, Germany, in 2015. Currently serving as the Deputy Chairman of the Youth Committee of the Second Committee of the Anhui Branch of the Asia-Pacific Vascular Academic Alliance, committee member of the Vascular Surgery Branch of the Anhui Medical Association, committee member of the Vascular Surgery Branch of the Anhui Physician Association, committee member of the Aortic Dissection Specialty Committee of the Endovascular Society of the Chinese Physician Association, youth committee member of the International Union of Angiology China Branch, committee member of the Intravascular Treatment Committee for Lower Limb Veins of the Microcirculation Society, and committee member of the Anhui Minimally Invasive Medical Association.
Currently engaged in vascular surgery clinical work for over 10 years, specializing in minimally invasive diagnosis and treatment of common vascular surgical diseases. Professional expertise: Endovascular minimally invasive treatment of aortic and peripheral diseases, local anesthesia minimally invasive treatment for varicose veins of the great saphenous vein. The new technology and project "Individualized minimally invasive treatment for varicose veins of the lower extremity great saphenous vein" has been rated as leading in China. In the past five years, has led and participated in three provincial-level research projects, published over 10 SCI papers including in JVS and EJVES, and six papers in the Chinese Journal series. Co-authored one monograph and granted two patents.
Copyright Statement: This platform aims to help medical and health professionals better understand the latest developments in relevant disease areas. The information content published on this platform does not imply agreement with its descriptions or viewpoints, but is only for providing more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will handle it as soon as possible. This information is solely for medical and health professionals to stay informed, and such information cannot replace professional medical guidance in any way, nor should it be regarded as diagnostic or treatment advice. If such information is used for purposes other than staying informed, this platform and the author shall not bear any related responsibilities.Contact email for cooperation:vascular@edoctor.work。
