Prof. Li Guoliang's Team: Management of Recurrent Type I Stenotic Lesions

DK Medtech
Vascular Interventional Balloon Product Developer

With the vigorous development of China's peripheral vascular intervention market, ordinary peripheral balloons have entered a stage of full competition. However, for the increasing number of highly resistant stenotic lesions, ordinary balloons tend to cause complications such as excessive vascular injury, flow-limiting dissections, and hematomas. On the other hand, pressure-focusing balloons utilize cutting/notching elements positioned between the inner wall of the blood vessel and the outer diameter of the balloon during expansion, enhancing localized pressure and enabling efficient directional dilation. This reduces vascular elastic recoil and represents a new direction in the evolution of vascular intervention balloons.
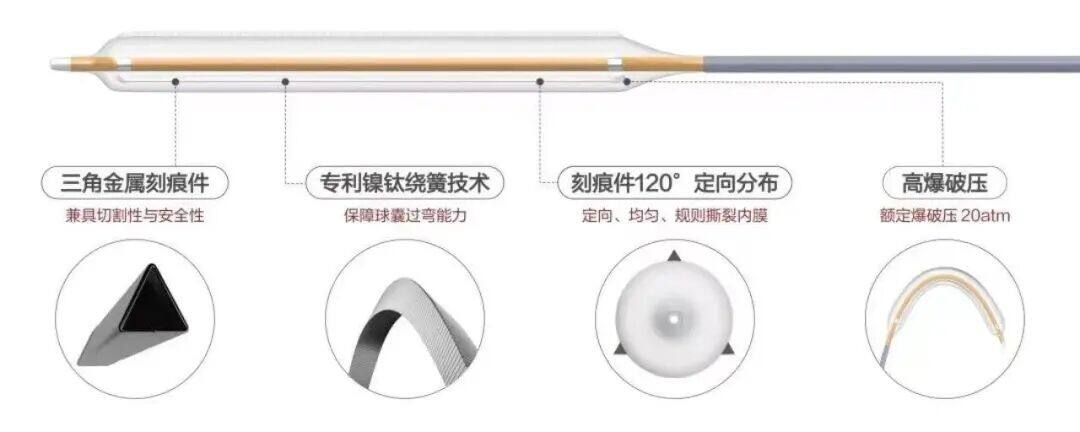
DK Medtech's independently developed DKutting™ High-Pressure Scoring Balloon, featuring an exclusive patented design (CN201810478242.X), boasts numerous advantages such as excellent deliverability, uniform expansion, and high burst pressure. In terms of overall product performance, it can be described as a "hexagonal warrior," with virtually no weaknesses. This marks a significant breakthrough for local enterprises in innovating and surpassing top-tier imported products.
DK Medtech Special Release[Professor Li Guoliang's Team: Management of Recurrent Type I Stenotic Lesions] Case Presentation, demonstrating the precise operations of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized intraoperative procedures and technical applications, complication prevention, to perioperative management, etc., the aim is to promote the standardization of diagnosis and treatment for vascular stenosis and occlusive diseases, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for future diagnosis and treatment, benefiting more clinical patients.

Management of Recurrent Type I Stenotic Lesions
Li Guoliang, Suolang QuzhenTibet Autonomous Region People's Hospital

Patient Information
Basic Information:Male patient, 67 years old.
Chief Complaint:More than 2 years of maintenance hemodialysis, poor function of the internal fistula for 3 days.
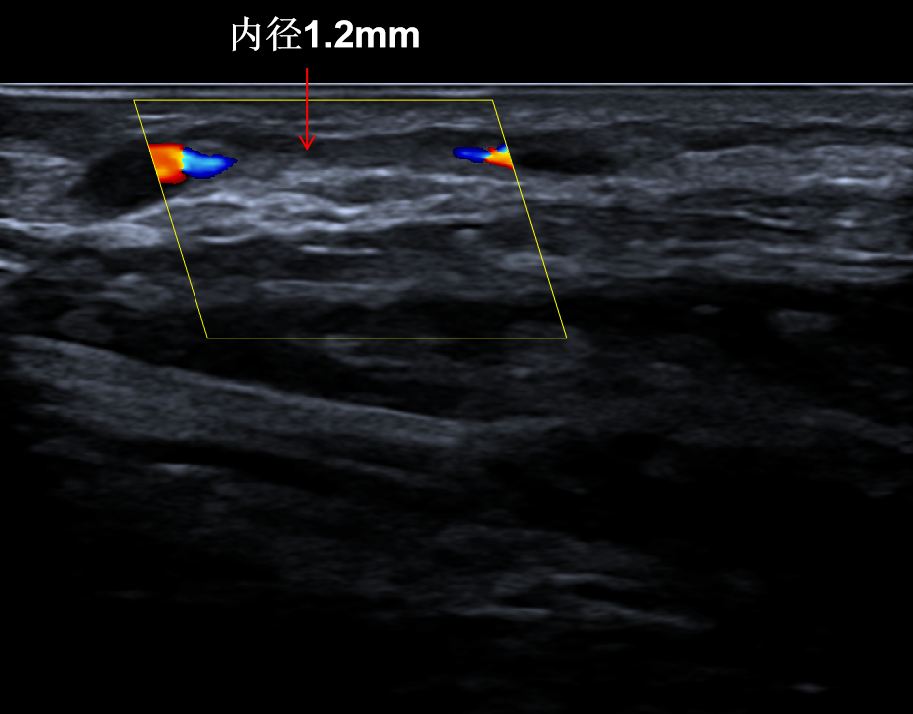
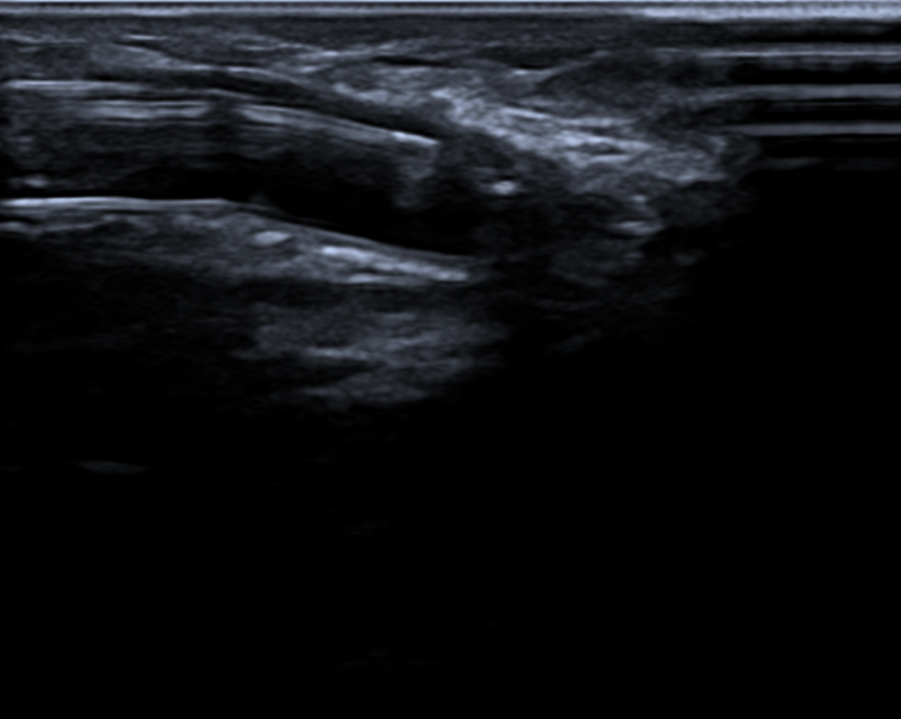
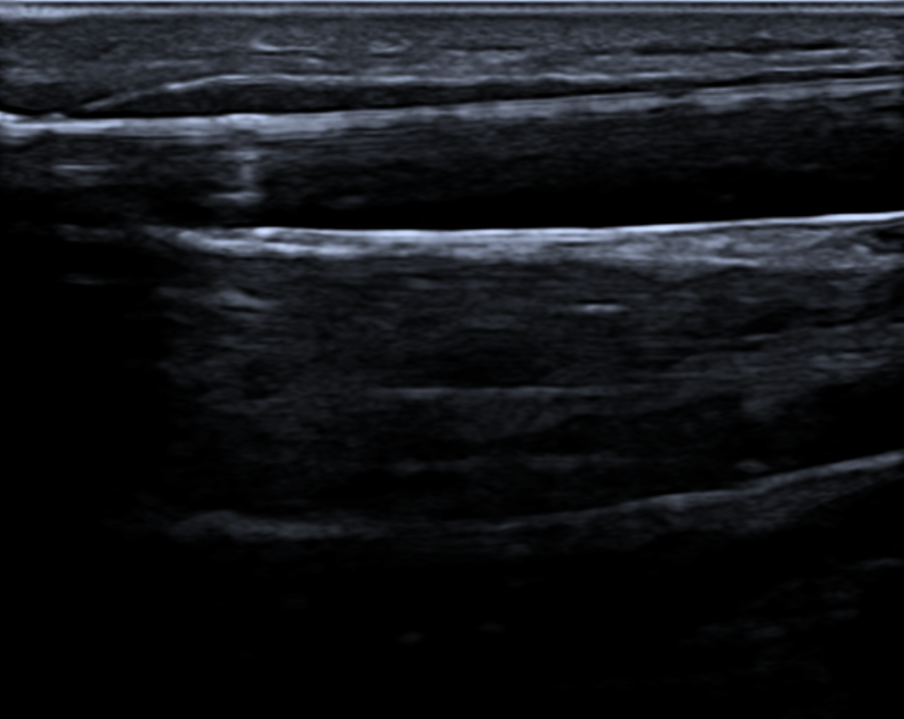
History of Present Illness:The patient visited the clinic two years ago due to fatigue and swelling, and was diagnosed with "chronic kidney disease stage 5" at that time. The primary disease was considered to be diabetic nephropathy. On March 17, 2022, a temporary catheter was placed in the right femoral vein, followed by hemodialysis treatment. On March 31, a semi-permanent catheter was inserted into the right internal jugular vein, and in April of the same year, an arteriovenous fistula surgery was performed on the left forearm. Two months later, hemodialysis treatment was continued using the fistula as the vascular access until now. Three days ago, during the patient's dialysis, there was insufficient flow upon connection, suggesting stenosis of the fistula. An outpatient ultrasound indicated Type I stenosis, and the patient was admitted for treatment due to "dysfunction of the fistula."
Past Medical History:Past medical history includes "Type 2 Diabetes" for 18 years and "Hypertension" for 6 years. Denies history of chronic diseases such as "Heart Disease" and denies history of infectious diseases.。
Physical Examination:Physical Examination of the Left Upper Limb
Visual Examination: The skin of the left upper limb is rosy, and there are two surgical scars visible on the right forearm, located approximately 3 cm and 5 cm above the wrist, each about 3 cm in length.Traces, two blunt needle puncture scars are visible on the cephalic vein of the left forearm, no aneurysmal dilation, and no skin damage.
Palpation: The skin temperature of the left upper limb is normal. Pulsation can be felt at the anastomosis of the internal fistula, and weaker thrill can be palpated at the arterial puncture site.
Auscultation: Whistling murmur at the anastomosis site, high-pitched whistling murmur at the arterial puncture site.
Admission Diagnosis:
Stenosis of Left Anterior Arm Internal Fistula (Type I);
Chronic Kidney Disease Stage 5, Maintenance Hemodialysis;
Diabetic Nephropathy;
Type 2 Diabetes;
Hypertension Grade 3, Very High Risk.
Previous interventional treatment
Time | Main Treatment Process |
March 17, 2022 | Hemodialysis treatment initiated via a temporary dialysis catheter in the right femoral vein. |
March 31, 2022 | Insertion of a semi-permanent catheter into the right internal jugular vein, removal of the temporary catheter from the right femoral vein |
April 3, 2022 | Underwent left forearm arteriovenous fistula surgery, the fistula matured two months post-operation, and the right neck semi-permanent catheter was removed. |
February 5, 2023 | Type I stenosis of left forearm arteriovenous fistula, PTA treatment |
April 16, 2023 | Type I stenosis of the left forearm arteriovenous fistula, followed by reconstruction of the proximal left forearm arteriovenous fistula after poor efficacy of PTA treatment. |
Preoperative Analysis
Preoperative Analysis:The patient had stenosis of the left forearm fistula and underwent PTA treatment twice. The stenosis recurred in a short period of time, and the patient also had diabetes, with significant intimal hyperplasia at the stenosis site. Afterward, proximal reconstruction was performed, but intimal hyperplasia still occurred within one year. The effect of ordinary balloon dilation was poor, and it might be necessary to choose a balloon that fits its characteristics. This time, the use of a scoring balloon for treatment is considered.
Surgical Objective:
Main Objectives:Resolve stenosis;
Secondary Objective:Improve the patency rate of internal fistulas and reduce the recurrence rate.
Surgical Strategy/Plan:Balloon Angioplasty of Left Forearm Arteriovenous Fistula Under B-mode Ultrasound Guidance.
Surgical Procedure
Puncture the cephalic vein of the forearm against the blood flow direction. After successful puncture, insert the needle sheath, remove the needle core, and then insert the guidewire along the needle sheath to establish support. Subsequently, insert the 6F catheter sheath.
A 0.035" standard hydrophilic guidewire was inserted along the catheter, passing retrograde through the stenotic lesion → anastomosis → proximal radial artery → brachial artery, followed by injection of 20mg of sodium heparin.
A 6mm*40mm DKutting high-pressure scoring balloon from DK Medtech was inserted along the guidewire to dilate the stenotic lesion, and a clear mark was observed when the pressure reached the working pressure.
Gradually increase the pressure to 20atm, be sure to open it significantly and maintain for 3 minutes.
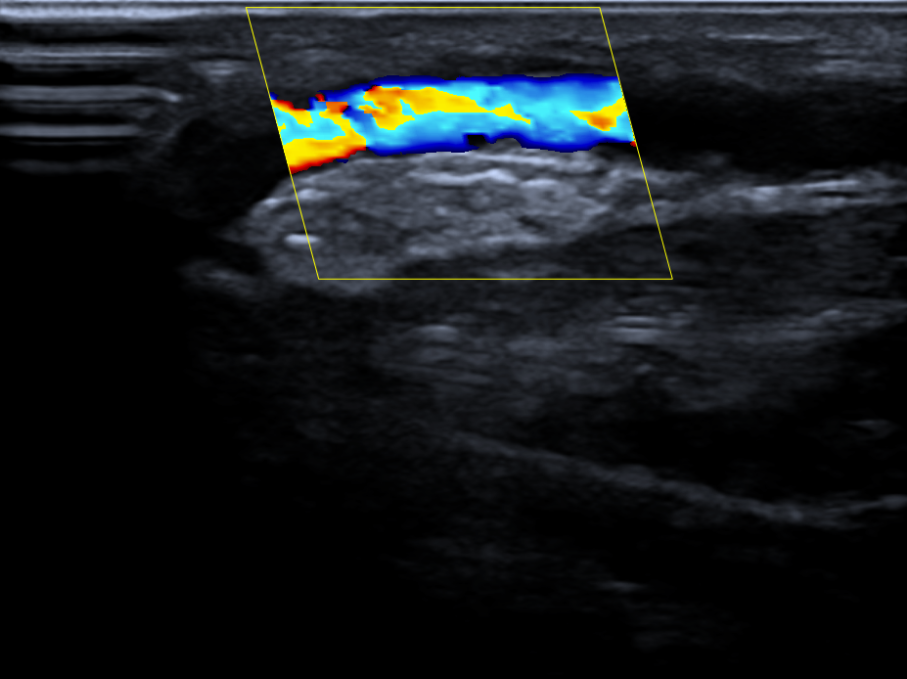
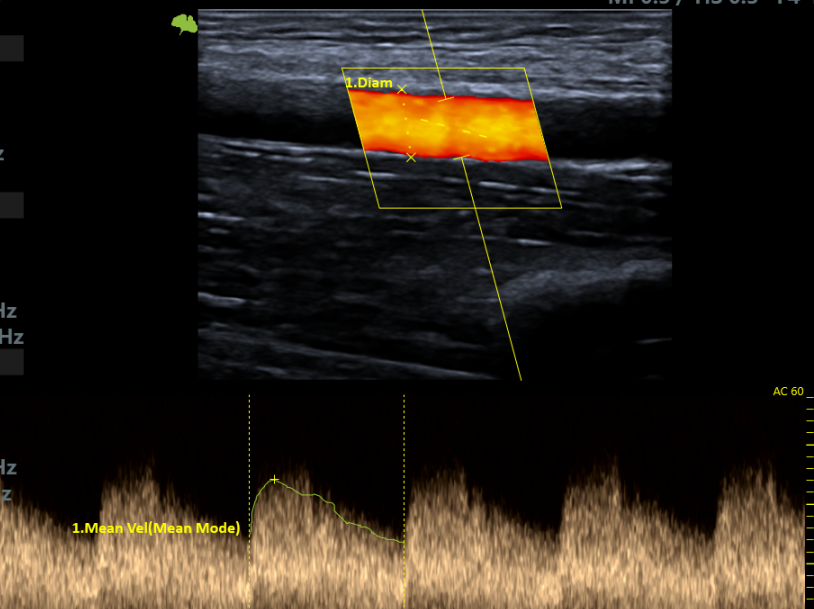
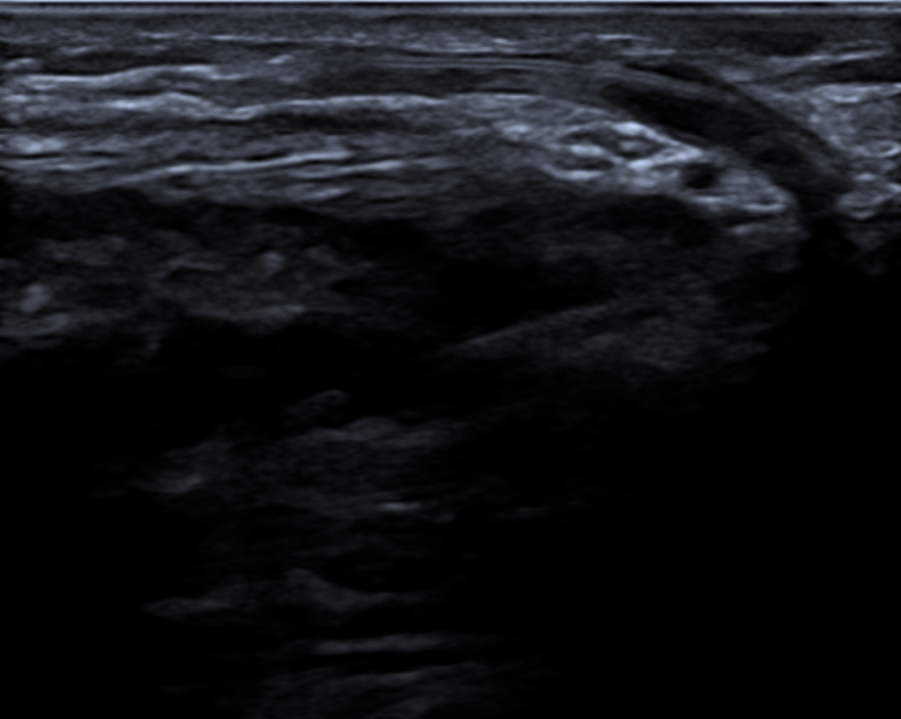
Postoperative blood flow signal is full, and postoperative VF1435.2ml/min.
Follow-up
Discharge Status:Postoperative vascular dilation was significant, and the internal fistula was used normally with a blood flow rate of 250ml/min during dialysis. On March 18, 2024, an outpatient review showed that the stenosis had resolved, and the brachial artery flow reached 870ml/min.
Case Summary
Case Characteristics:The patient's left forearm fistula has repeatedly narrowed in a short period of time, with intimal hyperplasia being the main lesion.
Preoperative Assessment Key Points:Evaluate vascular proliferation, select balloon size, and formulate a reasonable surgical plan.
Surgical Strategy/Technical Key Points:The patient has a short stenotic lesion, and it is recommended to use a pressure-focused balloon for vascular preparation. The balloon size should be 6mm, with a dilation time of 3 minutes.
Device Features/Usage Tips:Under the same balloon pressure, the small contact area generates localized high pressure, providing excellent expansion effects. The directional tearing of scoring elements can reduce injury to the vascular intima.

Expert Introduction


Dr. Guoliang Li, Associate Chief Physician
Surgeon of This Case
Group Leader of the Access Team, Department of Nephrology, People's Hospital of Tibet Autonomous Region;Member of the Vascular Access Intervention Group of the Ultrasound Intervention Committee of the Interventional Physicians Branch of the Chinese Medical Doctor Association.Hosted 1 internal scientific research project;Published multiple articles in national core journals.Secretary of the Tibet Blood Purification Quality Control Center.Proficient in the establishment, maintenance, and interventional treatment of vascular access.

Dr. Solang Quzhen, Attending Physician
Surgeon of This Case
Attending Physician, Department of Nephrology, People's Hospital of Tibet Autonomous Region;Secretary of the Tibet Medical Association Nephrology Society;Member of the Vascular Access Group, Blood Purification Branch, Tibet Medical Association.Hosted 1 scientific research project within the hospital.Advanced Study on "Endovascular Techniques for Vascular Access and Interventional Nephrology" at Haidian Hospital, Beijing, in March 2022.Expertise: Hemodialysis Technology, Dialysis Vascular Access, Renal Biopsy.

Department Introduction

Our department was established in May 2014, with a current capacity of 32 beds, 54 dialysis machines of various types, and a total of 46 medical staff members.
Our department was the first in the province to establish and maintain arteriovenous fistulas, and we began performing renal biopsies in 2017 in collaboration with Peking University People's Hospital. In 2021, we introduced treatments under B-mode ultrasound guidance for intravascular procedures and also began performing artificial blood vessel implantation surgeries. In 2023, we started conducting central venous angiography under DSA as well as PTA techniques for central venous diseases under DSA, placing us at a leading level within the province. Additionally, our department provides vascular access surgeries for dialysis centers across the Tibet region.
Copyright Statement: This platform aims to help healthcare professionals better understand the latest developments in relevant disease areas. The information published on this platform does not imply agreement with the descriptions and viewpoints therein; it is solely for providing more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will address them as soon as possible. The information is intended exclusively for healthcare professionals to stay informed, and such information cannot replace professional medical guidance in any way, nor should it be considered as medical advice. If such information is used for purposes other than staying informed, this platform and its authors shall not bear any related responsibility.Contact email for collaboration:vascular@edoctor.work。
