Hu Shanlian: Feasibility Assessment of Outcome-Based Payment Models for New Drugs

Fosun Kairos
Developer of Tumor Immune Cell Therapy Technologies and Products

Medi Cover
Innovative Commercial Insurance Solution Provider
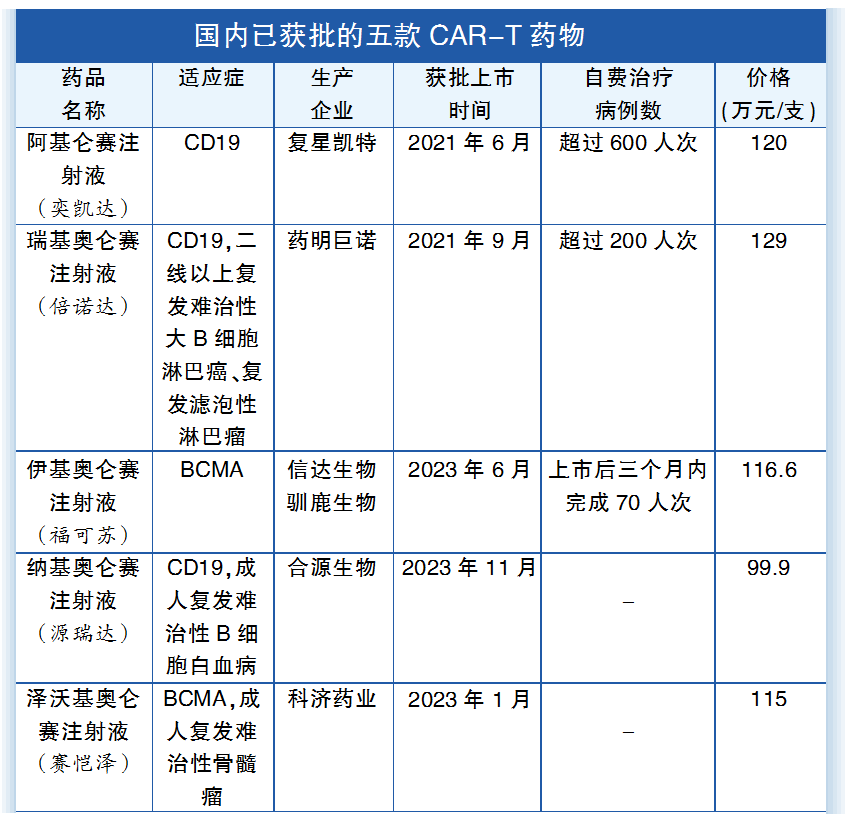
At the beginning of this year, Fosun Kite Biotechnology Co., Ltd. announced that it would join hands with Medi Cover, a subsidiary of Sinopharm Holding, to launch the first CAR-T cell therapy (Axicabtagene Ciloleucel Injection).Innovative Payment Plan Based on Efficacy Value for Lymphoma Patients Treated with Injection: For those who fail to achieve complete remission (CR) after treatment, a refund of up to 600,000 RMB can be obtained at the price of 1.2 million RMB per injection. Data shows that in the past two years, both Axicabtagene Ciloleucel Injection and Relmacabtagene Autoleucel Injection have passed the medical insurance form review, but ultimately failed to enter the medical insurance negotiation due to the high cost of treatment, as too few patients can afford this therapy.
From the perspective of the five CAR-T drugs currently approved in China, their prices are around 1 million yuan. In order to make them more affordable for patients, companies are actively helping patients obtain support from惠民保 (mutual aid insurance) and commercial insurance. In addition to exploring diverse funding methods, how to provide certain medical insurance compensation for innovative drugs according to China's national conditions has become a focal topic of discussion within the industry. Currently, outcome-based risk-sharing payment models are considered a worthwhile path to explore.
Payment based on outcomes has various names in different contexts. In foreign literature, it is commonly reported as Pay-for-Performance (P4P), Outcome-Based Contracts (OBA), Risk-Sharing Agreements (RSA), etc. This type of payment method involves a form of risk-sharing between pharmaceutical companies and health insurance payers, where payment depends on the final therapeutic effect of the drug. If the treatment effect is significant, the health insurance department pays in full; if patients do not achieve the expected therapeutic effect, the pharmaceutical company needs to fully or partially refund the cost of the medication.
This payment method is often applied to anti-tumor drugs, Alzheimer's disease, gene therapy or chronic disease medications, as well as drugs with uncertain clinical treatment effects or that patients cannot afford for long-term treatment. These drugs are often new drugs that have not completed Phase III clinical trials, lack long-term effect observation data, and are from single-arm clinical trials without a control group.
The advantages of this payment method are: First, it promotes the early market entry of innovative drugs, followed by obtaining real-world evidence through prospective observational studies after practical use; Second, it reduces the financial burden risk on health insurance payers and patients caused by treatment failure; Third, it encourages pharmaceutical companies to engage in sustainable research, development, and production; Fourth, it enhances the financial stability of the health insurance fund; Fifth, it stimulates the enthusiasm of doctors and health insurance departments in utilizing innovative drugs.
Although outcome-based payment methods play a crucial role in enhancing the value of pharmaceuticals and accessing significant medical technologies, they also face substantial challenges in terms of feasibility, including: 1. How to select clinical endpoints or surrogate indicators to accurately reflect clinical efficacy; 2. The complexity of designing protocols and collecting data requires the establishment of a database with accurate information; 3. Cost and efficacy data need to be more precise and transparent for timely sharing among healthcare providers, health insurance payers, and pharmaceutical companies; 4. Specialized technical research teams need to be established, involving considerable administrative costs; 5. Reimbursement of drug costs cannot be made promptly.
A British scholar once summarized twelve steps for outcome-based payment of innovative drugs in a report on breast cancer programs: 1. Establish inclusion criteria for measuring the relevant patient population; 2. Identify outcomes related to treatments in the data; 3. Convert raw data into measurable outcomes; 4. Stratify risks and identify risk factors for relevant subgroups; 5. Set outcome benchmarks to establish a baseline for efficacy evaluation; 6. Define efficacy metrics relative to the benchmark; 7. Aggregate results across different risk levels; 8. Determine contract structure based on the payment process from provider to payer; 9. Calculate outcome-based payment schemes during the contract period; 10. Determine the level of risk-sharing or the proportion of contract payments affected by OBA results (preset efficacy thresholds or linear compensation percentages based on efficacy); 11. Establish a payment formula that converts efficacy metrics into financial payments (with upper/lower limits); 12. Revise terms regarding updates to contract parameters/design during the contract period. These steps can serve as a reference for relevant departments when designing risk-sharing payment models in the future.
How feasible is it to implement risk-sharing payment methods in China to promote innovative drugs entering medical insurance reimbursement? The industry generally reflects that this idea is excellent, but there are still many difficulties at the execution level.
First, what are the criteria for selection or approval? For instance, which innovative drugs are suitable for试行 (pilot implementation) of outcome-based payment? How can fairness of opportunity be ensured? Based on the current total market sales of some innovative drugs as a proportion of total medical insurance drug expenditure, the share is very small and the impact is also minimal. Whether these drugs are worth promoting this payment method is still open to debate.
Secondly, this payment method requires a significant investment of human and material resources, with high management costs. The design of the plan and the collection of information demand even higher standards, and there are still considerable challenges in terms of human resource allocation. Currently, only dozens of innovative drugs in a few countries have implemented outcome-based payment methods. For instance, between 2017 and 2020 in Spain, 25 drugs adopted payment based on patient treatment outcomes. Some were implemented nationwide, while others were regional or limited to specific hospitals. The primary clinical endpoint for anti-tumor drugs is OS (Overall Survival). Follow-up periods range from 3 to 18 months, depending on survival time post-treatment and drug response time. In Saudi Arabia, 22 drug programs have been carried out under a pay-for-performance model over six years, updated every three years. Algeria, learning from Saudi Arabia’s experience, has actively promoted payment methods based on patient outcomes.
South Korea Introduced Risk-Sharing Contracts in 2013 as a Measure to Strengthen the Technology of New Drugs and Manage Drug Costs
Again, how this payment method adapts to China's existing fiscal and medical insurance systems in terms of the form and timeliness of cost reimbursement remains to be studied.
In summary, risk-sharing payment models based on either financial or therapeutic outcomes provide a valuable reference for promoting the development of innovative drugs in the future. These models seek to strike a balance between meeting patient needs, improving the accessibility of new drugs, and managing basic medical insurance funds. This is particularly relevant for certain oncology or rare disease treatments, such as cell therapy, gene therapy, and other high-cost immune and biologic agents, driving the coordinated and high-quality development of China’s medical insurance, healthcare, and pharmaceutical industries.




www.yyjjb.com.cn
Insight into Industry Trends

"Pharmaceutical Economy News"
Academic Official Account
Focus on the Frontiers of Oncology Academia

Terminal Official Account