Boston Scientific Acquires Silk Road Medical for $1.16B to Lead the TCAR Market

Silk Road Medical
Minimally Invasive Medical Device Developer

Boston Scientific
Medical Device Manufacturer
Recently, Boston Scientific announced that$1.16 Billion AcquisitionU.S. Publicly Listed CompanySilk Road Medical. MessagePublishAfter,Silk Road Medical's stock price surged by 23.8%.It is reported that,Silk Road MedicalMainly developed forTranscarotid Artery RevascularizationSurgical Procedure (TCAR)Innovative devices to treat carotid artery stenosis and prevent stroke.
Data shows that carotid artery stenosis is a type of hemodynamic disorder in the neck vessels and an important cause of ischemic stroke. Stroke has an extremely high disability and mortality rate, with at least 1 out of every 5 deaths in China being attributed to stroke. Clinical evidence indicates that most strokes caused by carotid artery stenosis can be prevented through appropriate diagnosis and treatment.
Previously, the surgical treatment options for carotid artery stenosis included carotid endarterectomy (CEA) and carotid artery stenting (CAS). Among them, carotid endarterectomy (CEA) is the "gold standard" procedure for removing atherosclerotic plaques and reconstructing normal lumen and blood flow; carotid artery stenting (CAS) is a minimally invasive interventional treatment with less trauma and faster recovery.
For many years, the medical community has been discussing which surgical method is more advantageous for treating carotid artery stenosis, and there have been numerous clinical comparative studies on carotid endarterectomy (CEA) versus carotid artery stenting (CAS). However, each method has its own advantages and disadvantages, and neither has shown an overwhelming superiority.
In 2015, Silk Road Medical began promoting the TransCarotid Artery Revascularization (TCAR) procedure in the U.S. market. This marked the introduction of a third treatment option for carotid artery stenosis. To date, Silk Road Medical has collaborated with clinical experts to publish research findings in multiple journals, demonstrating the safety and efficacy of the TCAR procedure. As a result, the medical community and industry are increasingly recognizing the value of TCAR.
Boston Scientific's Premium Acquisition of Silk Road Medical This Time May Be Due to Their Belief That the TCAR Procedure Will Become the Standard Treatment for Carotid Artery Stenosis. By Acquiring Silk Road Medical, the Only Company with an Approved Product for the TCAR Procedure, Boston Scientific Hopes to Dominate the Entire Carotid Artery Stenosis Market.
However, some clinical experts said that it is too early to evaluate the pros and cons of the three surgical methods. The competition among the three major surgical methods has just begun.
In the market competition of medical devices, innovative techniques are often the sharpest weapons.
For example, in the market for coronary artery stenosis, the initially common interventional treatment was coronary stent implantation, with the corresponding product being cardiac stents. For a long time, cardiac stents dominated the market, and the revenue of related companies surged. Later, some companies collaborated with clinical experts to innovate coronary balloon angioplasty. The corresponding product, drug-coated balloons, immediately began to compete with cardiac stents for market share and achieved significant success.
In the carotid artery stenosis market, there are signs that the current market competition is evolving into a competition of surgical methods.
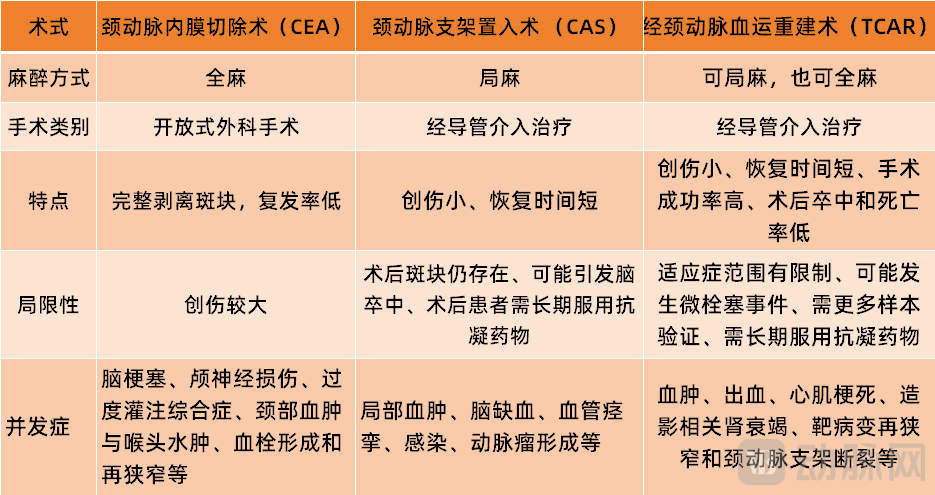
(Comparison of the Three Surgical Procedures)
Regarding the treatment of carotid artery stenosis, the first surgical procedure to appear was carotid endarterectomy (CEA). In the 1950s, after Michael Ellis DeBakey completed the first CEA surgery, an increasing number of clinicians began to explore and apply CEA.
According to the early clinical trial results of CEA, compared with drug therapy, CEA treatment did not show sufficient safety and efficacy. In an early study with a sample size of only 20 cases: 7 deaths occurred in the surgical group (3 died during the postoperative perioperative period), and 10 deaths occurred in the non-surgical group. Although the treatment effect was unsatisfactory, the medical community did not stop researching this surgical procedure.
After 40 years of development, doctors began to stratify the risks for patients with carotid artery stenosis and standardized the surgical procedures, which significantly improved the safety and effectiveness of CEA. Currently,CEA has become the gold standard for carotid artery surgical treatment., Clinically, a treatment approach for carotid artery stenosis has been formed, where moderate to severe stenosis is mainly treated with surgery, and mild stenosis is primarily managed with medication.
In terms of specific procedures, the CEA technique involves making a horizontal or oblique incision at the base of the patient's neck near the collarbone. The length of the incision is typically 6-8 centimeters, though some patients may require an incision of 8-10 centimeters. After exposing the carotid artery through the incision, the surgeon can use an aortic clamp to stop blood flow. The vessel is then cut open, plaque is removed, and the artery is flushed and sutured before the incision is closed layer by layer.
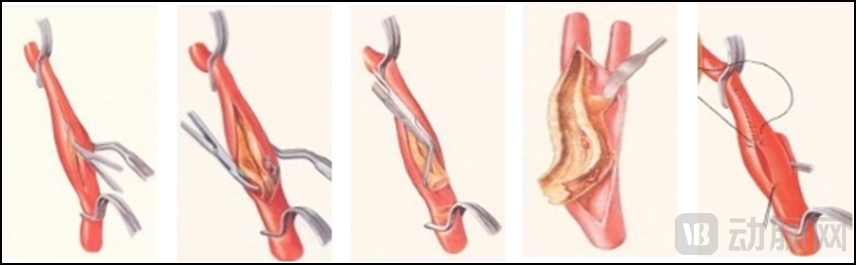
(Carotid Endarterectomy (CEA) Surgical Diagram)
Obviously, the CEA procedure can completely strip plaque with a low recurrence rate, but it involves significant trauma. During the decades when the CEA procedure was being perfected, interventional concepts and treatments were also quietly emerging, and some doctors attempted to explore interventional treatment methods for carotid artery stenosis.
In 1993, the clinically more mature carotid artery stenting (CAS) emerged.The doctor performs a puncture at the femoral artery in the patient's groin, guiding the guidewire and catheter through the blood vessels to the site of carotid artery stenosis, and then delivers the carotid artery stent to the lesion site. Afterwards, the stent expands the plaque, increasing the vascular lumen at the stenosis and restoring blood flow to the brain.
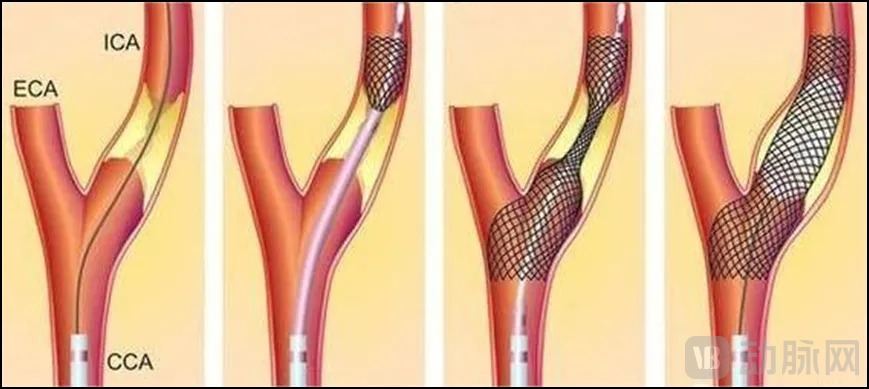
(Schematic Diagram of Carotid Artery Stent Placement (CAS) Surgery)
Compared with carotid endarterectomy (CEA), carotid artery stenting (CAS) is characterized by minimal invasiveness, shorter recovery time, no need for general anesthesia, and a reduction in some CEA-related adverse events. However, carotid artery stenting (CAS) also has its limitations, such as the continued presence of plaque post-procedure, which may lead to stroke, and the need for patients to take anticoagulant medications long-term after the procedure.
It is worth mentioning that the safety of CAS in its early stages was also at a relatively low level. However, with the surgical procedures becoming increasingly standardized, clinicians gaining more experience, and the selection of surgical indications becoming more scientific, the safety of CAS has continuously improved. According to publicly published clinical trial data, the rate of 30-day mortality and stroke associated with CAS surgeries dropped from 2.9% in 2000 to 0.6% in 2008.
When carotid endarterectomy (CEA) became the gold standard procedure and carotid artery stenting (CAS) also matured, the debate between the two began.。
In 2004, a comparative study (SAPPHIRE) on CEA and CAS in high-risk patients with CEA was completed, showing that CAS was superior to CEA for high-risk patients. However, three large-sample, multicenter randomized trials conducted between 2006 and 2010 all showed that CEA was superior to CAS.
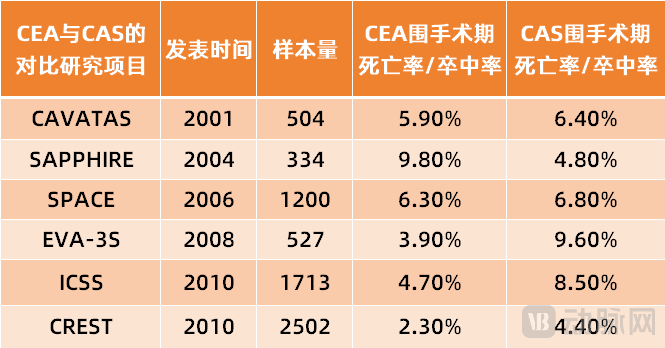
(2001-2010 Partial Comparative Study Projects on CEA and CAS Procedures)
In 2010, a larger-scale multicenter randomized controlled trial was completed. This study enrolled 2,502 patients with symptomatic and asymptomatic carotid artery stenosis. The trial results showed: no significant difference between the CEA and CAS groups, but the intraoperative stroke rate was higher in the CAS group, while the perioperative myocardial infarction rate was higher in the CEA group.
So far, comparative studies between CEA and CAS are still ongoing, and neither has shown overwhelming superiority. The associated products for CEA include surgical instruments such as scissors, hemostatic clips, micro tweezers, aortic clamps, and periosteal elevators; the associated products for CAS include catheters, guidewires, carotid artery stents, and carotid balloon dilation catheters, which are more expensive, have larger market potential, and come with higher marketing budgets from manufacturers.
Driven by the active promotion of manufacturers and the concept of intervention, CAS has been more widely applied in China. According to statistics from the Stroke Prevention Committee: In 2019, stroke center hospitals across China completed 6,280 CEA and 19,688 CAS procedures, with CAS being approximately three times the number of CEA. However, in the United States, the situation is reversed, with the number of CEA surgeries being about seven times that of CAS.
Against the backdrop of CAS and CEA competing for market share, Silk Road Medical has identified a new market opportunity. It found that multiple clinical trials have shown that the 30-day postoperative mortality or stroke rate in the CAS group is significantly higher than in the CEA group. Targeting this clinical pain point,Silk Road Medical, Inc. jointly created with clinical experts in 2012TransCarotid Artery Revascularization (TCAR) Technique。
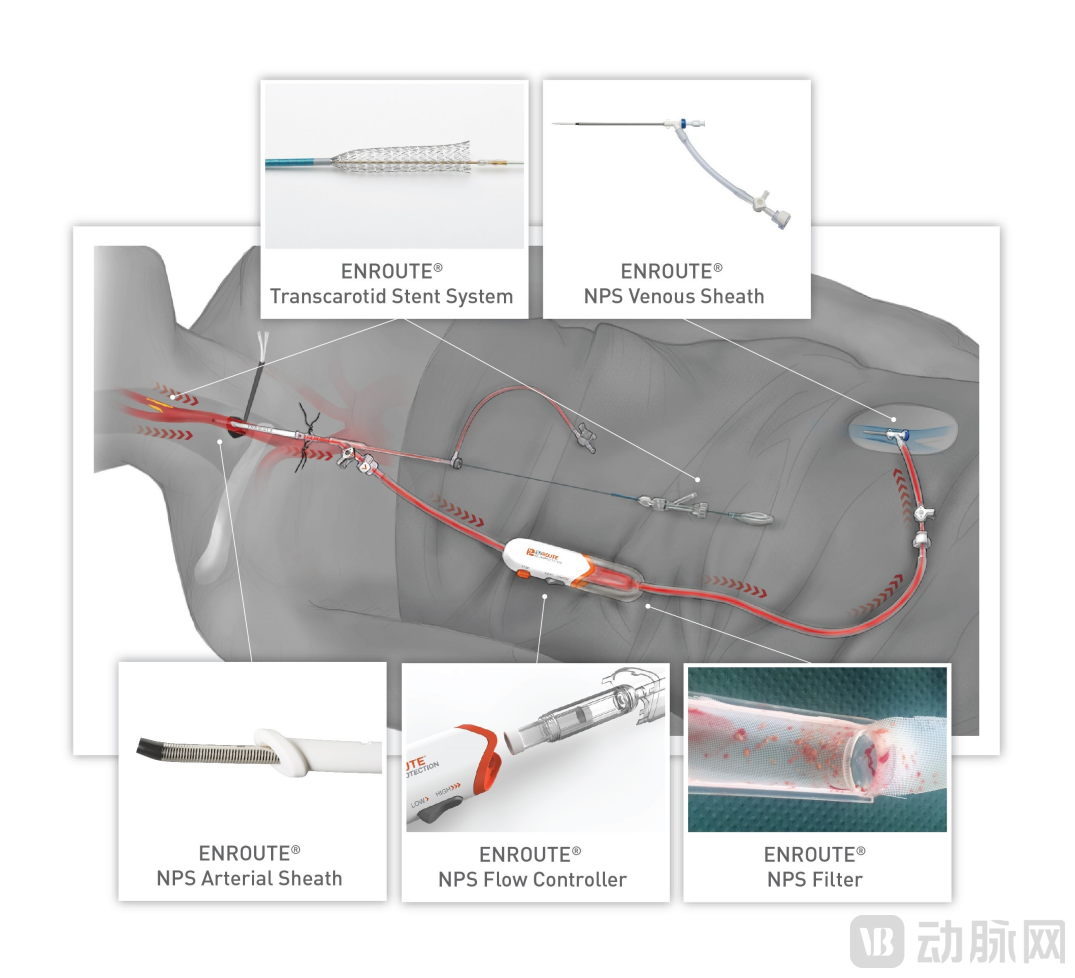
(TCAR Product Portfolio)
Data shows that TCAR surgery, innovatively introduced by Silk Road Medical, combines the techniques of CAS and CEA. It includes both the direct visualization of common carotid artery clamping in carotid endarterectomy (CEA) and the local anesthesia and stent placement involved in carotid artery stenting (CAS). With the combination of these two approaches, TCAR surgery not only features the characteristics of minimally invasive procedures but also significantly reduces the risk of stroke, death, and myocardial infarction within 30 days post-operation.
As of now, only Silk Road Medical has been approved for the core complementary products of TCAR surgery in the global market: the ENROUTE Reverse Flow Thrombus Protection Device and the ENROUTE Carotid Stent System. The ENROUTE Reverse Flow Thrombus Protection Device is used to directly access the common carotid artery and initiate temporary blood flow reversal; the ENROUTE Carotid Stent System is a self-expanding, self-tapering stent that can enter the lesion through the carotid artery, improving accuracy.
A comparative study between TCAR and the gold standard procedure CEA for carotid artery stenosis showed that: despite higher medical risks in patients undergoing TCAR, the in-hospital stroke/mortality rates were similar for both TCAR and CEA. The study analyzed 1,182 TCAR and 10,797 CEA cases from the VQI database of the American Venous and Lymphatic Society between January 2016 and March 2018.
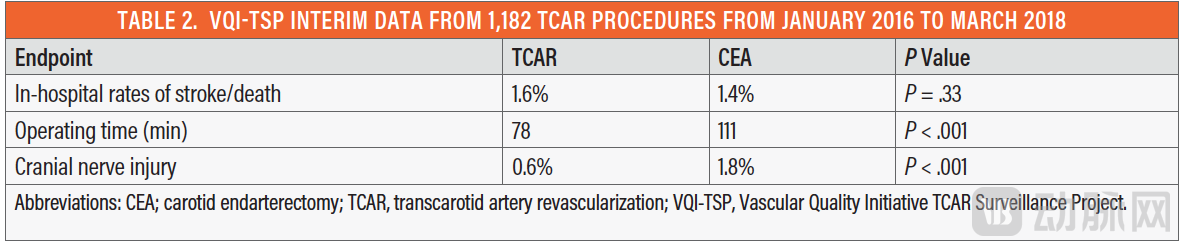
(Image courtesy of Endovascular Today)
In another study, compared with carotid artery stenting (CAS), TCAR had lower rates of stroke, perioperative mortality, and cranial nerve injury; there was no difference between the two in terms of stroke and mortality at 30 days and 1 year postoperatively.
Based on this series of clinical research data, TCAR has shown the potential to replace carotid artery stenting (CAS).The U.S. market also validates this point: In the VQI database of the American Venous Forum, from 2016 to 2018, the number of TCAR procedures grew exponentially; CAS showed a declining trend.
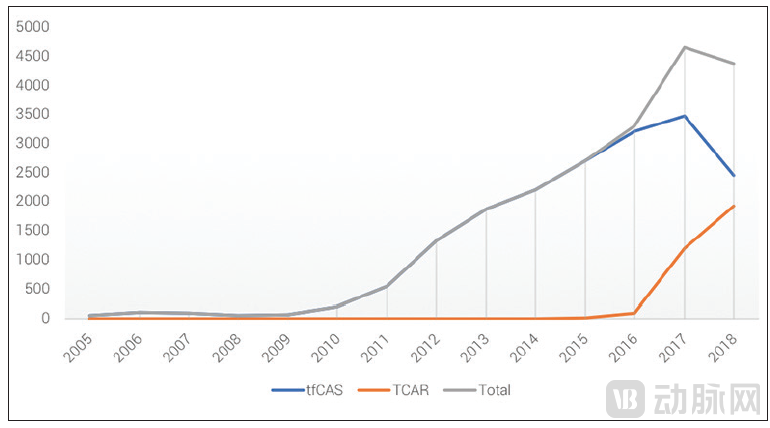
(Trends in the Use of TCAR and CAS in VQI, Image from Endovascular Today)
From the existing data, compared with the gold-standard surgical procedure CEA, TCAR has a similar mortality/stroke rate and offers advantages such as minimally invasive intervention; compared with the minimally invasive interventional procedure CAS, TCAR shares the same minimally invasive benefits while demonstrating superior clinical data. It seems that TCAR could already claim victory and dominate the carotid artery stenosis treatment market.
However, on the one hand, TCAR still has certain limitations; on the other hand, CAS continues to enhance safety and clinical outcomes through innovative products and refined indications for specific patient populations, with ongoing improvements in procedural safety and efficacy. In December 2019, Professor Brajesh Lal's team published the latest results of the CREST-2 registry study in JACC: The perioperative stroke/mortality rate of CAS was lower than in previous randomized trials and comparable to the outcomes observed with new revascularization techniques such as TCAR. Professor Brajesh Lal stated:The latest CAS technology efficacy may surpass the data results from previous studies.。
Therefore, it is still too early to evaluate the pros and cons of the three surgical methods, and we will have to wait and see which one becomes mainstream in the future.
CAS has advanced alongside the progress of medical devices. From the first-generation self-expanding stents to the current dual-layer stents, and from not using embolic protection devices to utilizing various types of embolic protection devices, the supporting equipment for carotid artery stenting (CAS) has continued to evolve, enhancing its safety and efficacy.
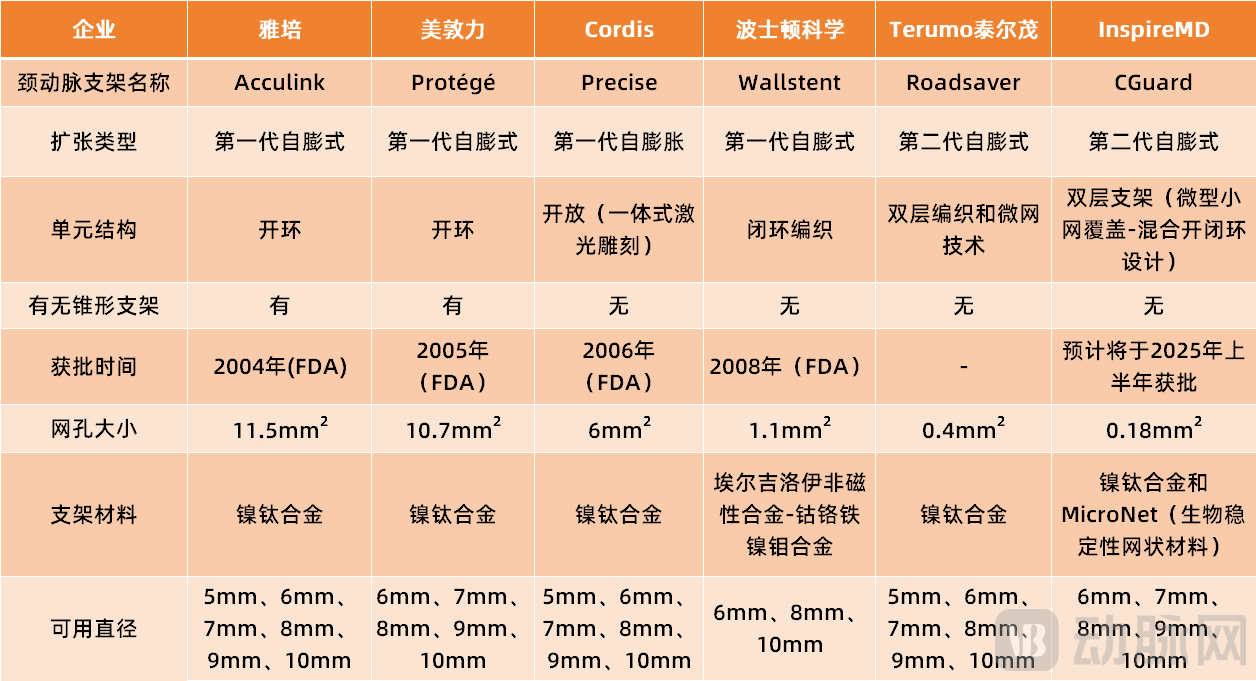
As of now, there are approximately 10 commonly used carotid artery stents globally. Among them, the first-generation products such as Abbott's Acculink, Medtronic's Protege, Cordis' Precise, and Boston Scientific's Wallstent were all developed nearly 20 years ago, and these products currently hold a significant market share.
Taking Medtronic's Protege as an example, the product received FDA approval in 2005 and entered the Chinese market in 2006, achieving a relatively high market share in China. Protege adopts an open-loop design (the smallest mesh is connected to other meshes), offering advantages such as good conformability, better wall apposition for tortuous vessels, strong radial support, and minimal risk of displacement after deployment.
After years of practical application, clinical findings have revealed that the first-generation carotid artery stents, due to their single-layer structure, often lead to plaque prolapse and detachment within the stent. Additionally, these stents are prone to issues such as strut embedding, fibrous cap rupture, and plaque prolapse, increasing the risk of postoperative embolic events.
In response to this pain point, innovative companies have begun collaborating with clinicians to improve stent design and increase plaque coverage.In recent years, a new generation of dual-layer mesh carotid artery stent systems has finally emerged., such as the Roadsaver stent developed by Terumo and the CGuard stent developed by InspireMD.
Taking the CGuard stent as an example, its inner layer is a nitinol stent, and the outer layer is covered by a MicroNet mesh. This design not only provides the stent with stronger anti-embolic force but also allows it to better encase lesions within the blood vessel, preventing further deterioration of the lesion structure. The MicroNet is a mesh woven from "polyethylene terephthalate (a bio-stable reticulated material)" with pore sizes typically ranging between 150–180 micrometers. It is used to capture and seal thrombi and plaques on the blood vessel wall, preventing embolism, and offers protection for up to 48 months.
At the same time, the CGuard stent utilizes the memory properties of nitinol, allowing the stent to change shape at different temperatures. Without requiring a specific tapered design, it achieves more precise adherence to the vessel wall while reducing surgical complexity.
InspireMD executives stated: If all goes well, the company will submit the final report to the FDA in the second half of 2024, and the CGuard stent is expected to receive FDA PMA approval in the first half of 2025.
China's innovative medical device company, Zhongtian Medical, believes that: although the second-generation carotid artery stent reduces the mesh size of the stent, the deliverability of the double-layer stent is relatively poor, requiring the use of a larger diameter delivery catheter, which increases vascular irritation during the procedure. Therefore, in collaboration with Professor Liqun Jiao's team from Xuanwu Hospital, Capital Medical University, they independently developedZhongtian Tianmi Carotid Artery Stent. Currently, the product has recently been approved by the National Medical Products Administration (NMPA) and has entered the "Green Channel" for special review of innovative medical devices.
According to the introduction, the Zhongtian Tianmi carotid artery stent adopts the world's first single-layer micro-pore hybrid weaving technology. The mesh area is only 1/30 of that of traditional cut-type stent mesh, increasing plaque coverage and effectively avoiding the delamination risk associated with double-layer stents. The product also utilizes the superelastic strain hysteresis energy storage characteristics of nickel-titanium alloy to ensure effective dilation of the narrowed area while avoiding excessive stimulation to blood vessels. Additionally, the product uses a protective film on the stent surface, significantly reducing nickel ion release and enhancing corrosion resistance and biocompatibility.
Compared with traditional braided stents, the Zhongtian Tianmi carotid artery stent has stronger radial support; compared with laser-carved stents, it has lower chronic outward force.
In addition to stent products, innovative companies have also developed more complementary devices for carotid artery stenting (CAS), such as distal occlusion devices, distal filtration devices, and proximal occlusion devices. These devices all help to reduce the risks associated with CAS procedures and minimize the possibility of plaque detachment flowing to the brain.
Currently, the clinical efficacy of embolic protection devices such as distal occlusion devices, distal filtration devices, and proximal occlusion devices has been confirmed by various clinical studies. The use of embolic protection devices during carotid artery stenting (CAS) has also become a consensus among most experts. With innovative stents and improved supporting devices, the safety and efficacy data of CAS have significantly improved.
Overall, neither CAS nor TCAR has been developed for more than 30 years, and both are still in the development stage. Therefore, the competition between the two is bound to be a protracted battle. It may take a long time to clearly see the future of the carotid artery stenosis market.