Five-Year Follow-Up Results of Hengrunda's BCMA CAR-T (HDS269B) in Relapsed/Refractory Multiple Myeloma Highlight Durable Efficacy and Safety

Hrain Biotechnology
Developer of Tumor Immunotherapy Technology R&D


June 24, 2024
eMedClub News
Research Results
eMedClub
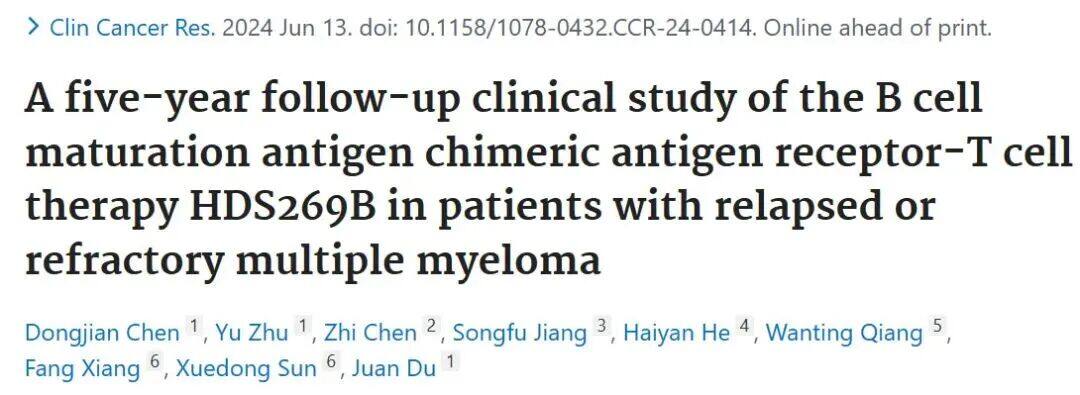
This study is an open-label, multi-center, single-arm, non-randomized Phase I/II trial, enrolling a total of 49 RRMM patients who have received ≥3 prior lines of therapy (including proteasome inhibitors and immunomodulatory agents), administering the BCMA CAR-T cell product HDS269B.The clear infusion regimen is cyclophosphamide + fludarabine, with an infusion dose of 9×10.6CAR-positive live T cells/kg (±15%).
Patient Characteristics
A total of 49 patients with RRMM received lymphodepletion and CAR-T cell infusion, of which 20 (40.82%) had poor physical status (ECOG 3-4) at enrollment. 42.86% had high-risk cytogenetic features, 63.27% had received ≥4 lines of therapy, and 79.59% showed disease progression at the time of infusion. Among patients with poor physical status, 30% had extramedullary disease (EMD), 45% had high-risk cytogenetics, 70% had received ≥4 lines of therapy, and 80% progressed after the last line of treatment.
IMWG Remission
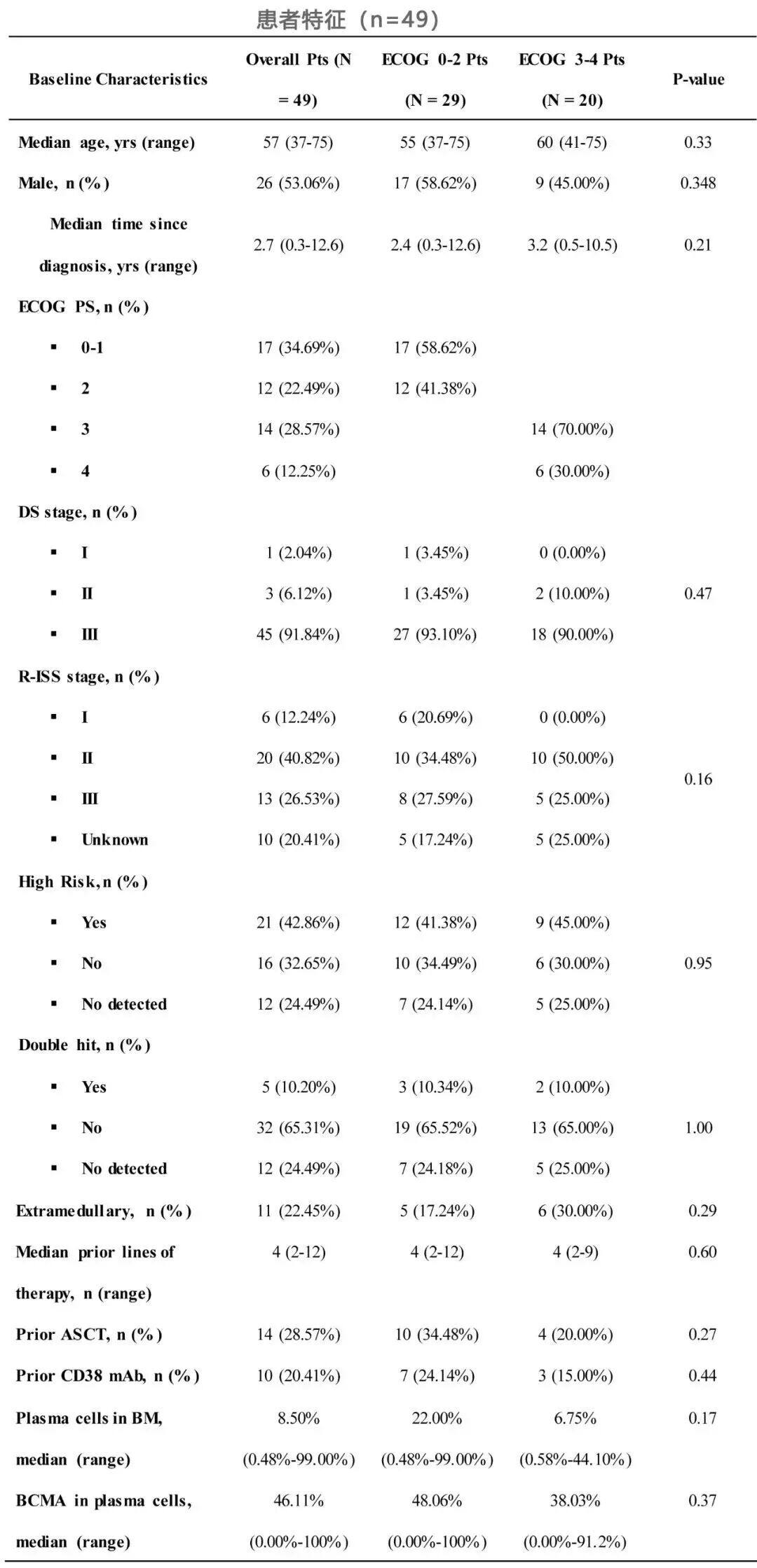
Median follow-up of 59.0 months,ORR was 77.55%, the rate of stringent complete response (sCR) was 24.49%, complete response (CR) rate was 24.49%, very good partial response (VGPR) rate was 16.33%, and partial response (PR) rate was 12.24% (Table 1). The overall response rate (ORR) was similar among patients with different ECOG scores, with 79.31% for ECOG 0–2 and 75% for ECOG 3–4 (P=0.72).
Treatment Outcome
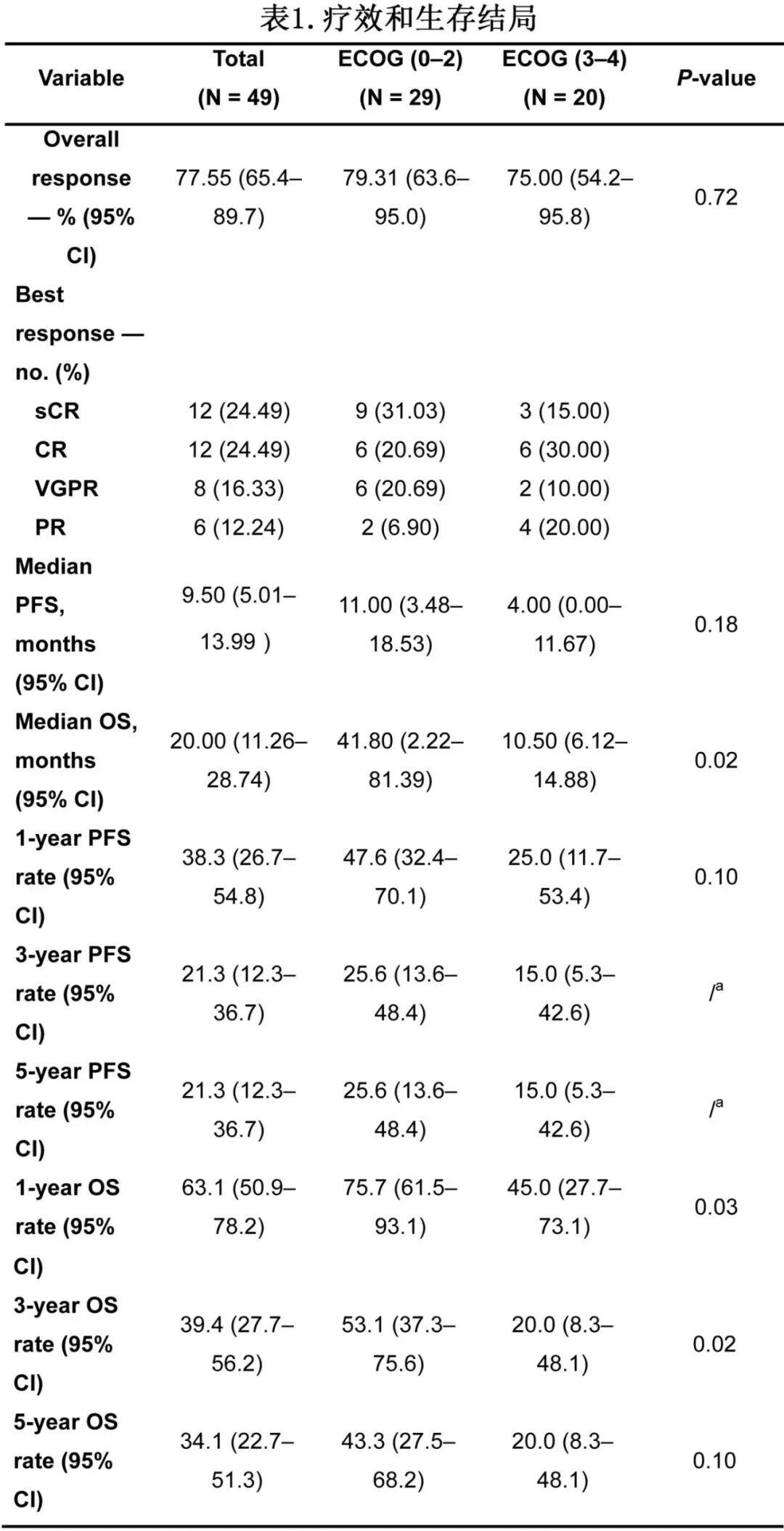
The median progression-free survival (PFS) and overall survival (OS) were 9.5 months and 20.0 months, respectively (Fig. 1A,B), with 5-year PFS and OS rates of 21.3% and 31.4%, respectively (Table 1). The median PFS for patients with ECOG scores of 0–2 and 3–4 were 11.0 months and 4.0 months, respectively (P=0.18, Fig. 1C), and the median OS was 41.8 months versus 10.5 months (P=0.015, Fig. 1D).
Patients with ≥4 prior lines of therapy had shorter PFS and OS compared to those with <4 lines of therapy (PFS: P=0.012; OS: P=0.0049; Figure 2A-B).
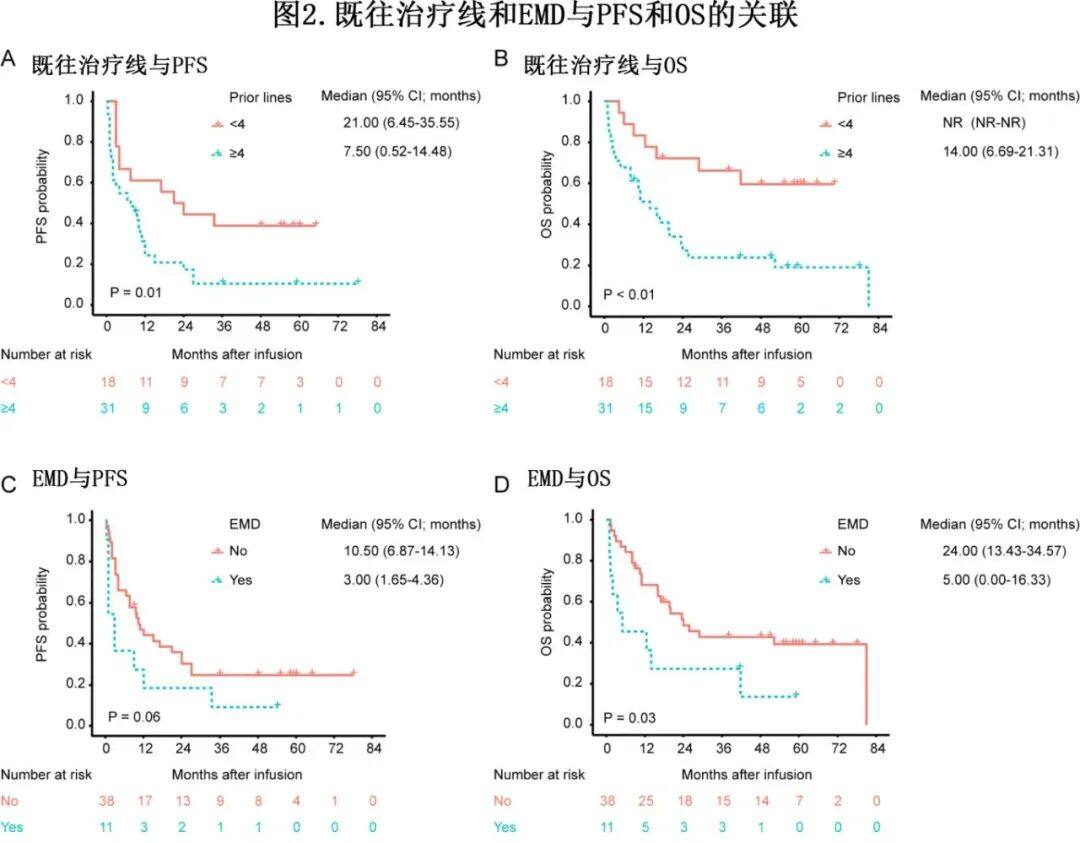
EMD is highly aggressive, and in this study, 11 patients had EMD at enrollment. Although the ORR for patients with and without EMD was 64% and 82%, respectively, the median PFS and OS of patients with EMD were significantly shorter than those without EMD (PFS: 3.0 months vs 10.5 months, P=0.06; OS: 5.0 months vs 24.0 months, P=0.03; Figure 2C-D).
At the 6-month comparison after infusion, the PFS and OS of patients who achieved CR/sCR were significantly longer than those who did not reach CR (PFS: P=0.04; OS: P=0.02), with a similar trend observed at 3 months and 12 months.
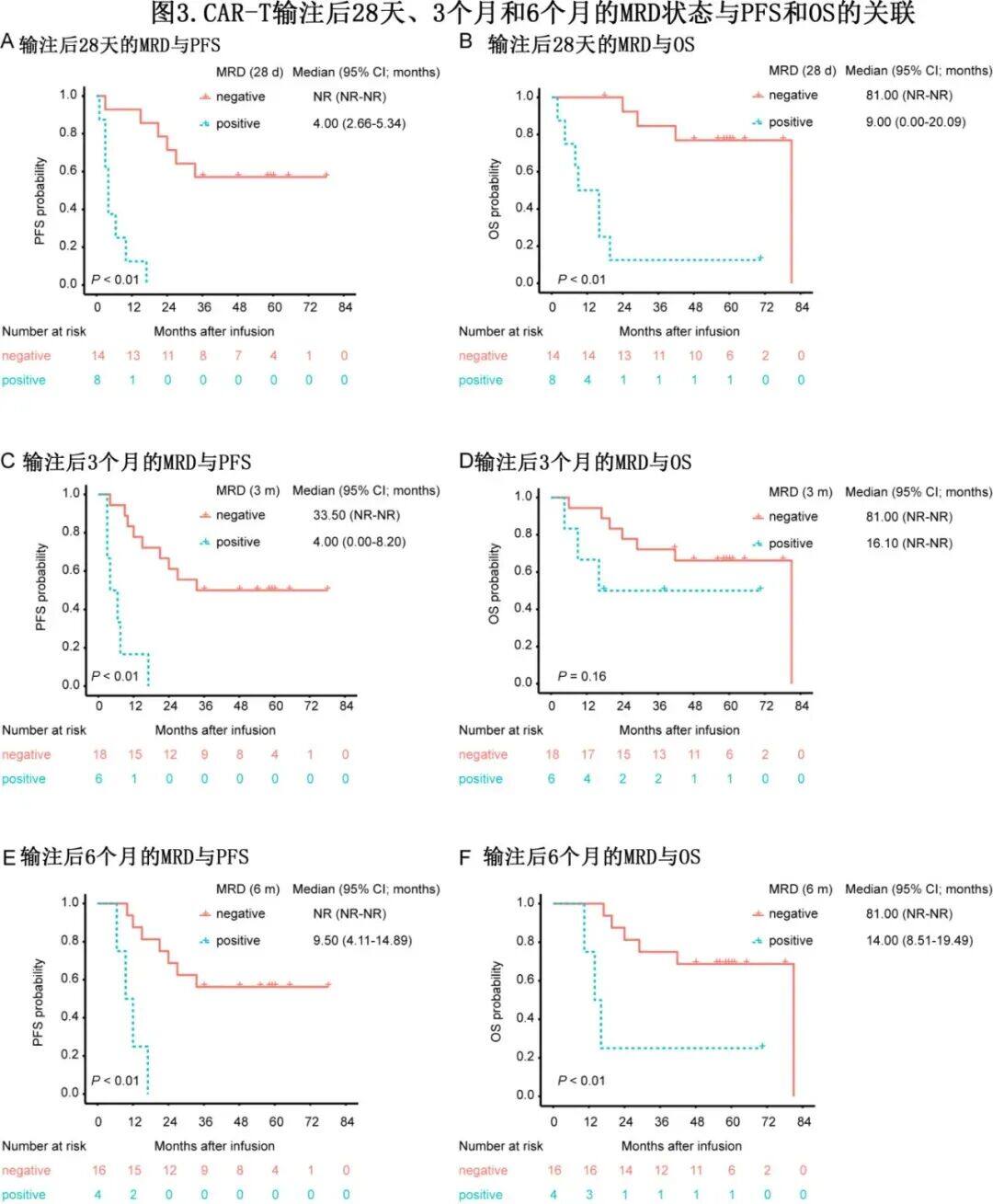
MRD has a good correlation with PFS and OS, and can reasonably predict the prognosis and clinical benefits of MM. Based on this, MRD is expected to gain FDA approval as a new surrogate endpoint for the accelerated approval and market launch of new therapies in the MM field. In this study, 22 patients had MRD data at D+28 after infusion, of which 14 achieved MRD negativity (10-4), including 1 case of sCR, 2 cases of CR, 3 cases of VGPR, and 8 cases of PR.PFS and OS were significantly longer in patients who were MRD-negative at D+28 than in those who were MRD-positive.(Figure 3A, B), confirming that the early MRD status plays a crucial role in predicting disease progression and survival outcomes. Additionally, detecting the MRD status at 3 months and 6 months also has a similar effect (Figure 3C-F).
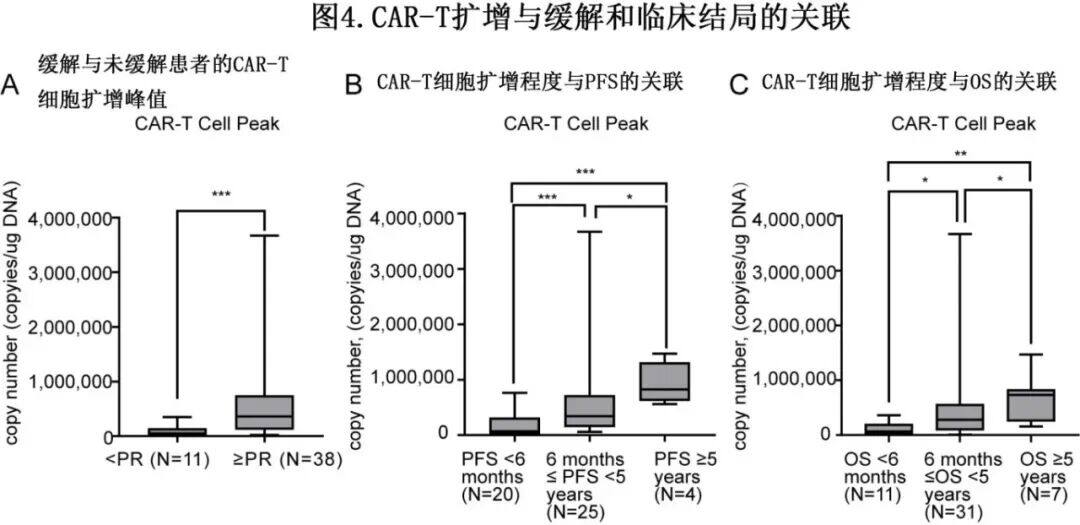
Median Time to Peak Concentration(Tmax)On day 11 and day 28, the proliferation of CAR-T cells significantly decreased.Significant Association Exists Between CAR-T Cell Expansion and Clinical OutcomesPatients who achieved ≥PR had higher peak levels of CAR-T cells compared to those who did not reach PR (Figure 4A). Patients who had not progressed within 5 years after infusion also exhibited higher peak expansion of CAR-T cells than those who progressed (Figure 4B). Additionally, patients with longer OS had higher peak CAR-T copy numbers (Figure 4C). Further evaluation was conducted on the persistence of CAR-T cells for ≥6 months.(n=21), ≥12 months(n=14), ≥24 months(n=8)And ≥36 months(n=2)The impact showed that patients with persistent CAR-T cells had significantly improved PFS and OS compared to those without detectable CAR-T cells in their blood, thus confirming the potential of CAR-T cell persistence as a predictive indicator for long-term treatment success.
Safety
Well tolerated during long-term follow-up, with a toxicity profile consistent with previous reports.Overall, 100% of patients experienced at least one adverse event (AE). The most common long-term (after 28 days) grade ≥3 AEs were hematological adverse events, including neutropenia (38.8%, 19/49), anemia (40.8%, 20/49), thrombocytopenia (30.6%, 15/49), and lymphopenia (26.5%, 13/49). No secondary primary malignancies or late-onset immune effector cell-associated neurotoxicity syndrome (ICANS) were observed.
Predictive Factors of PFS
HDS269B demonstrated significant efficacy in RRMM patients, but with variations in long-term outcomes; thus, the authors categorized patients based on PFS: <6 months.(n=20), ≥12 months(n=20), ≥24 months(n=15), ≥36 months(n=10), ≥48 months(n=9)And ≥60 months(n=4)Notably, 70% of patients with PFS <6 months had received ≥4 lines of treatment, compared to only 22% of patients with PFS ≥48 months.
In univariate Cox regression analysis, prior ≥4 lines of therapy and CAR-T cell persistence ≥6 months were significant predictors of PFS. Patients with prior ≥4 lines of therapy had significantly worse PFS compared to those with <4 lines of therapy.(7.50 vs 21.0 months; HR=2.372, P=0.017; Figure 2A). However, multifactorial Cox regression analysis only foundCAR-T cell persistence ≥6 months is an independent predictor of PFS.
Predictive Factors of OS
Classify patients based on OS: <6 months(n=11), ≥12 months(n=30), ≥24 months(n=21), ≥36 months(n=18), ≥48 months(n=15)And ≥60 months(n=7)In patients with OS<6 months, the incidence of EMD was significantly higher than in those with OS≥60 months (55% vs. 0%, P=0.017). Additionally, 91% of patients with OS<6 months had received ≥4 lines of therapy, compared to 29% in patients with OS≥60 months.
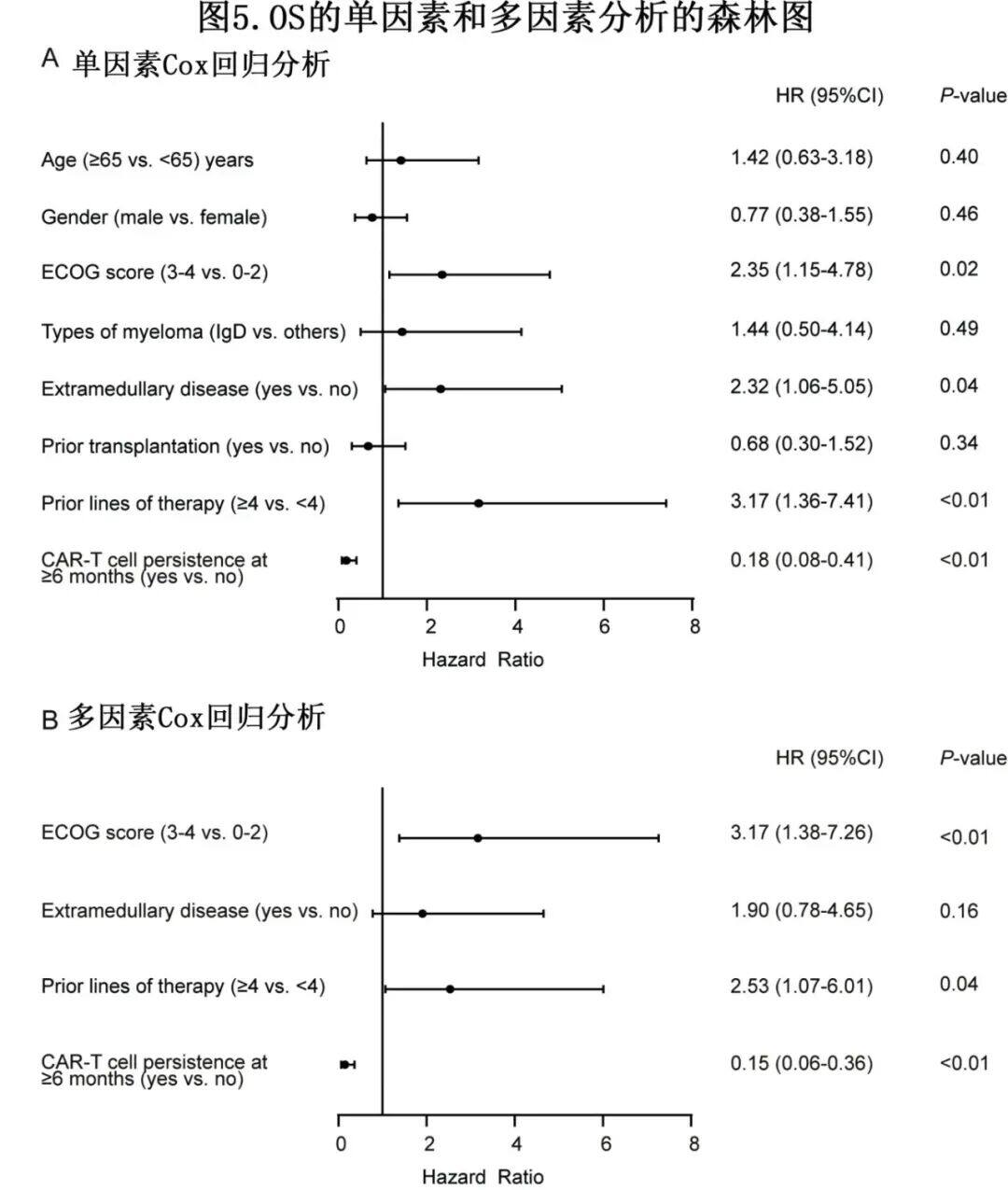
In univariate Cox regression analysis, ECOG 3–4 (HR=2.35, P=0.02), EMD (HR=2.32, P=0.04), and prior ≥4 lines of therapy(HR=3.17,P=0.01)Associated with shorter OS (Figure 5A), while CAR-T cell persistence ≥6 months is associated with longer OS.(HR=0.18,P<0.01)Multivariate analysis revealed that,ECOG 3-4 (HR=3.17, P=0.01) and prior ≥4 lines of treatment(HR=2.53,P=0.04)It is an independent predictor of shorter OS, while CAR-T cell persistence ≥6 months is significantly associated with longer OS (HR=0.15, P<0.01) (Figure 5B).
Summary
eMedClub
This article reports on BCMA CAR-T cells (HDS269B)Five-Year Follow-Up Results of 49 RRMM Patients, Including Those with Poor Physical Status(ECOG 3-4, n=20),and factors affecting long-term outcomes were identified. With a median follow-up of 59.0 months, the overall response rate was 77.55%. The median PFS and OS were 9.5 months and 20.0 months, respectively, with 5-year PFS and OS rates of 21.3% and 34.1%, respectively. Patients with ECOG scores of 0-2 showed significantly prolonged survival, with a median PFS of 11.0 months and a median OS of 41.8 months. Early MRD negativity, higher and sustained CAR-T cell expansion, and absence of extramedullary disease were associated with better survival outcomes. No new CAR-T cell therapy-related toxicities were observed during long-term follow-up. Importantly, ECOG 0-2, prior treatment lines <4, and CAR-T cell persistence ≥6 months were independently associated with longer survival.
The 5-year long-term follow-up results highlight the BCMA CAR-T cells(HDS269B)The sustained efficacy and safety of the treatment, particularly in ECOG 0-2 patients, are noteworthy. Additionally, the number of prior treatment lines and CAR-T cell persistence ≥6 months are significant independent predictive factors. Therefore, poor performance status is not an absolute contraindication for CAR-T therapy; however, better performance status and earlier application of CAR-T cell therapy will offer more benefits to multiple myeloma patients, suggesting a need for exploration and application in frontline settings.
Exciting Live Broadcast Preview
Press and hold to scan the QR code to participate immediately ↓
June 26 (Wednesday) 19:00-20:30
Universal Cell Therapy Special Forces —— Serum-free Cell Culture of γδ T Cells



Share

Collection

Like

In view