
Breast cancer is the second most common cancer globally and one of the leading causes of cancer-related deaths. Among them, triple-negative breast cancer (TNBC) is a highly aggressive subtype of breast cancer, accounting for 15-20% of all breast cancer cases. Due to the lack of estrogen receptor (ER), progesterone receptor (PR), and HER2 expression, traditional endocrine therapy and HER2-targeted treatments have limited efficacy in these patients. Currently, chemotherapy remains the primary treatment for TNBC, but its effectiveness is limited and it comes with significant side effects. The average overall survival (OS) for patients with advanced or metastatic TNBC is 12 to 18 months, with only about 14% of patients surviving five years post-diagnosis.
Recently, in the field of breast cancer treatment, AstraZeneca's first-in-class AKT inhibitor Truqap (capivasertib) has delivered a disappointing message: the Phase III CAPItello-290 clinical trial, which evaluated capivasertib in combination with paclitaxel as a first-line treatment for locally advanced (inoperable) or metastatic triple-negative breast cancer (TNBC), did not meet the dual primary endpoint of overall survival (OS). It is evident how challenging it is to treat triple-negative breast cancer!

This result not only "disappointed" the R&D team but also once again highlighted the challenges in tackling triple-negative breast cancer. What exactly happened with capivasertib in the Phase III CAPItello-290 clinical trial? What is the current state of treatment for triple-negative breast cancer, and how are targeted therapies progressing? Let’s take a closer look!
Capivasertib Phase III CAPItello-290 Fails in Triple-Negative Breast Cancer
Capivasertib is a first-in-class highly selective inhibitor of AKT1/2/3, achieving breakthroughs in the treatment of HR+/HER2- breast cancer. Previously reported:NMPA Accepts the First AKT-Targeted Drug Capivasertib! New Hope Emerges for Breast Cancer Treatment。
In November 2023, it was approved by the FDA for use in combination with fulvestrant to treat such patients, becoming the world's first approved AKT pathway inhibitor. See:NEJM: Capivasertib for the Treatment of HR-Positive Breast Cancer (CAPItello-291 Study)、Lancet Oncol: Capivasertib Combined with Fulvestrant Significantly Extends Progression-Free Survival in Patients with Advanced Breast Cancer
Phase III CAPItello-290 Clinical Trial Aims to Evaluate the Potential First-Line Treatment Efficacy of Capivasertib Chemotherapy Combination in Specific TNBC Patients. The study specifically assessed two primary endpoints: OS improvement in the overall trial population and OS improvement in the subgroup of patients with tumors carrying PIK3CA, AKT1, or PTEN biomarker alterations, involving 923 patients. In its announcement, AstraZeneca did not provide specific data, only revealing that the Capivasertib combination failed to significantly improve overall survival in either the total study population or the subgroup of patients with specific mutations in the PIK3CA, AKT1, or PTEN genes.
Traditional treatment methods for TNBC, including chemotherapy, radiotherapy, and surgery
Therefore, finding more effective treatment methods is urgent. Studies show that approximately 35% of TNBC cases exhibit alterations in the PIK3CA, AKT1, and PTEN proteins. The Phase III CAPItello-290 trial, which focuses on Capivasertib for treating triple-negative breast cancer, has drawn significant attention.
Advances in Targeted Therapy for Triple-Negative Breast Cancer
In recent years, various targeted treatment strategies have emerged based on specific molecules and signaling pathways expressed in TNBC, including PI3K/AKT/mTOR inhibitors, epidermal growth factor receptor (EGFR) inhibitors, Notch inhibitors, PARP inhibitors, etc.
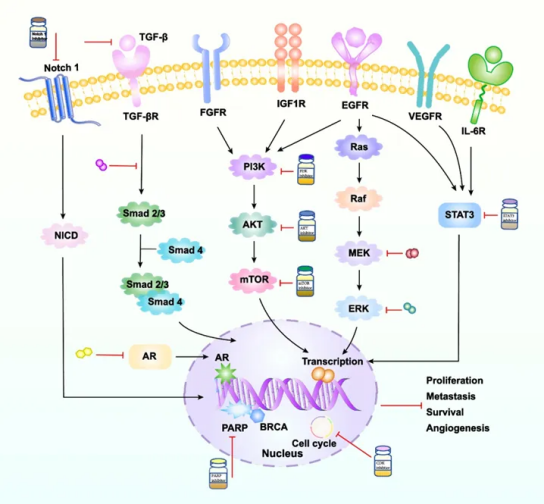
TNBC-Related Signaling Pathways and Their Inhibitors
1.Poly (ADP-ribose) polymerase (PARP) inhibitors
Malignant tumor cells are prone to BRCA gene mutations, such as BRCA1/2 genes in TNBC patients. PARP is a key enzyme for repairing single-strand DNA damage, and PARP inhibitors can lead to "synthetic lethality" in BRCA1/2-deficient cancers. The FDA has approved PARP inhibitors such as Olaparib and Talazoparib for the treatment of HER2-negative BC patients with BRCA mutations.
Olaparib: The OlympiAD trial comparing olaparib monotherapy to standard therapy in HER2-negative metastatic breast cancer demonstrated that, compared with standard therapy, olaparib monotherapy extended median PFS by 2.8 months, reduced the risk of disease progression or death by 42%, and prolonged OS. The OlympiA trial showed that, in the adjuvant treatment of early HER2-negative BC patients carrying BRCA1/2 germline mutations, olaparib significantly improved OS, 3-year invasive disease-free survival (iDFS), and distant disease-free survival (DDFS).
Talazoparib: The EMBRACA trial showed that, compared with chemotherapy, the talazoparib group had longer PFS (8.6 months vs. 5.6 months) and higher ORR (62.6% vs. 27.2%). The NEOTALA trial demonstrated that neoadjuvant talazoparib monotherapy in HER2-negative BC patients with BRCA1/2 germline mutations resulted in a significantly higher pCR rate.
2. Androgen Receptor (AR) Inhibitors
AR-positive expression is found in approximately 12% of HR-negative BC patients. Currently, researchers have explored many AR inhibitors for TNBC treatment. Although clinical trials have demonstrated the efficacy of AR inhibitors in treating TNBC patients, the exact mechanism remains unclear.
Bicalutamide: Clinical Benefit Rate (CBR) for treating TNBC is 19%, mPFS is 3 months, and patients showed good tolerance.
Enzalutamide: In AR-positive TNBC patients, mPFS and mOS were 3.3 months and 17.6 months, respectively; therefore, enzalutamide is recommended for the treatment of AR-positive TNBC patients. The TBCRC032 trial demonstrated that the combination of enzalutamide and taselisib in AR-positive TNBC patients achieved a CBR of 35.7% and an mPFS of 3.4 months.
Abiraterone: The UCBG 12-1 trial evaluating abiraterone in combination with prednisone for AR-positive locally advanced TNBC showed that patients receiving abiraterone had an mPFS of 7.5 months, an ORR of 8.22%, and a CBR reaching 20%.
3.CDK Inhibitors
CDK is a key enzyme regulating the transition of each phase of the cell cycle, and its continuous activation can lead to tumor cell proliferation. CDK4/6 inhibitors mainly suppress the G1-S phase, thereby inhibiting the DNA replication process in cells. The FDA has approved CDK4/6 inhibitors for the treatment of TNBC patients, including Palbociclib and Ribociclib.
Palbociclib: Previous PALOMA-2 and PALOMA-3 trials confirmed that palbociclib combined with endocrine therapy significantly improved PFS in patients with ER+/HER2− BC.
Ribociclib: Similar to palbociclib, ribociclib combined with fulvestrant significantly improves OS in patients with ER+/HER2− BC.
Abemaciclib: Compared with palbociclib, abemaciclib combined with endocrine therapy may prolong iDFS in patients with ER+/HER2− BC, with a favorable safety profile. Additionally, abemaciclib combined with fulvestrant significantly improves PFS and ORR in patients with ER+/HER2− BC.
Clinical trials of CDK4/6 inhibitors for the treatment of TNBC patients are still ongoing.
4. PI3K/AKT/mTOR Signaling Pathway Inhibitors
The PI3K/AKT/mTOR signaling pathway is the most common cancer-activated pathway, leading to the proliferation of tumor cells and a series of other malignant biological behaviors. It has been reported that about 10% of TNBCs have PI3KCA mutations.
LY294002 is the first PI3K inhibitor, and SF1126 is its modified form, which can inhibit tumors and angiogenesis. The combination of SF1126 and gefitinib can induce apoptosis in TNBC cells.
In addition to PI3K inhibitors, there are also AKT inhibitors in clinical trials. AZD5363 is used for the treatment of BC, gastric cancer, and prostate cancer. Ipatasertib as a monotherapy for TNBC. Capivasertib has antitumor activity against tumors with AKT1/E17K mutations. The LOTUS and PAKT studies showed that adding an AKT inhibitor to paclitaxel treatment in mTNBC prolonged PFS. The FAIRLANE study evaluated the efficacy of ipatasertib combined with paclitaxel in the treatment of early TNBC.
Currently, the first-generation mTOR inhibitors have been used to treat breast cancer, but PI3K inhibitors for TNBC are still in Phase I clinical trials.
5. Epidermal Growth Factor Receptor (EGFR) Signaling Pathway Inhibitors
EGFR is an effective therapeutic target for 89% of TNBC patients, and EGFR-targeted drugs have been approved for the treatment of cancer patients, including tyrosine kinase inhibitors (TKIs) such as gefitinib and monoclonal antibodies like cetuximab.
Gefitinib inhibits BC cell proliferation and enhances the cytotoxicity of carboplatin and docetaxel. Moreover, the combination of gefitinib, carboplatin, and docetaxel may synergistically increase cytotoxicity in TNBC cells. In patients with metastatic TNBC, the combination of cetuximab with carboplatin or cetuximab with cisplatin can double the pCR and extend PFS and OS.
6. Fibroblast Growth Factor Receptor (FGFR)
Amplification of FGFR1 or FGFR2 exists in TNBC, and the activation of FGFR1 is associated with the prognosis of OS. Studies have shown that FGFR-targeted therapy has significant efficacy in breast cancer treatment, especially when FGFR is amplified.
7. Vascular Endothelial Growth Factor Receptor (VEGFR)
Currently, the commonly used anti-VEGF drug is bevacizumab. The Phase III RIBBON 1 trial demonstrated that the combination of bevacizumab with capecitabine, anthracyclines, or taxanes improved PFS in patients with mTNBC. Further follow-up analysis showed that compared with the placebo group, the mPFS of TNBC patients in the bevacizumab combination group was significantly prolonged (6.0 months vs 2.7 months), and there was a trend toward improved OS.
8.Notch Signaling Pathway Inhibitors
The abnormal activation of the Notch signaling pathway is associated with the malignant biological behavior and prognosis of TNBC. Therefore, further exploration of the role of TNBC in this signaling pathway will deepen the understanding of the pathogenesis of TNBC, thereby exploring new targeted treatment strategies.
9.STAT3 Signaling Pathway Inhibitors
STAT3 Plays a Key Role in the Progression of TNBC Stem Cells. The Novel STAT3 Inhibitor WZ-2-033 Significantly Suppresses TNBC Proliferation and Tumorigenicity Both In Vivo and In Vitro by Blocking STAT3 Activation.
10. Transforming Growth Factor (TGF)-β Inhibitor
TGF-β is negatively correlated with the prognosis of TNBC patients. The bifunctional fusion protein Bintrafusp alfa is designed to simultaneously inhibit two immunosuppressive pathways in the tumor microenvironment. Studies have shown that compared with monotherapy, Bintrafusp alfa can more effectively block TGF-β and exhibits a stronger anti-tumor response. The anti-TGF-β/PD-L1 bispecific antibody YM101 demonstrates enhanced tumor-suppressive activity against TNBC. TGF-β inhibitors may become an effective treatment for TNBC.
Conclusion
Currently, Triple-Negative Breast Cancer Remains One of the Most Challenging Areas in Tumor Treatment. However, with a deeper understanding of the molecular mechanisms of the disease and continuous progress in new drug development, we have reason to believe that more treatment options will emerge in the future. Although AKT inhibitors faced setbacks in Phase III clinical trials, this will not stop our efforts to tackle "the most aggressive" breast cancer. Let us look forward to a future where breast cancer patients will have more targeted treatment options that are more effective and less toxic.
References:
[1] AstraZeneca’s Truqap Flops in Phase III Triple-Negative Breast Cancer Trial.By Tristan Manalac.Published: Jun 18, 2024.
[2] [2]AstraZeneca's Truqap misses the mark in late-stage triple-negative breast cancer trial.By Fraiser Kansteiner.Jun 18, 2024 9:09am.
[3] Zhu, S., Wu, Y., Song, B. et al. Recent advances in targeted strategies for triple-negative breast cancer. J Hematol Oncol 16, 100 (2023). https://doi.org/10.1186/s13045-023-01497-3
