Prof. Peng Hongying's Team: Scoring Balloon for Recurrent Outflow Stenosis in AVG

DK Medtech
Vascular Interventional Balloon Product Developer


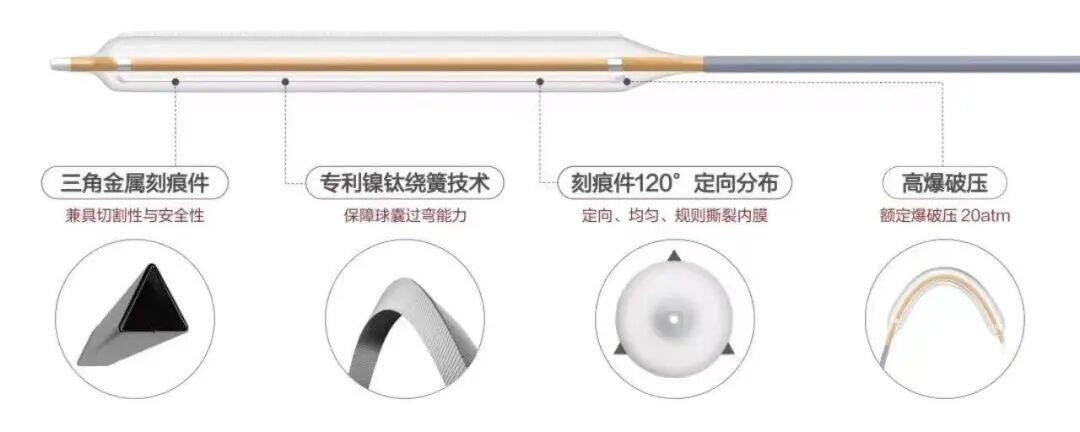
With the vigorous development of China's peripheral vascular intervention market, ordinary peripheral balloons have entered a stage of full competition. However, for the increasing number of highly resistant stenotic lesions, ordinary balloons tend to cause complications such as excessive vascular injury, flow-limiting dissections, and hematomas. On the other hand, pressure-focused balloons utilize cutting/notching components positioned between the inner wall of the blood vessel and the outer diameter of the balloon during expansion, which enhance localized pressure and enable efficient directional dilation. This reduces vascular elastic recoil, representing a new direction in the evolution of vascular intervention balloons.
DK Medtech's independently developed DKutting™ High-Pressure Scoring Balloon, featuring an exclusive patented design (CN201810478242.X), boasts numerous advantages such as excellent deliverability, uniform expansion, and high burst pressure. In terms of overall product performance, it can be described as a "hexagonal warrior," with virtually no weaknesses. This marks a significant breakthrough for local enterprises in innovating to catch up with and surpass top-tier imported products.
DK Medtech Special Release[Professor Peng Hongying's Team: The Use of Scoring Balloons for Recurrent Stenosis in AVG Outflow Tracts] Case Presentation, demonstrating the detailed operations of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized procedures and technical applications during surgery, prevention of complications, and perioperative management, etc., the aim is to promote the standardization of diagnosis and treatment for vascular stenosis and occlusive diseases, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for future diagnosis and treatment, benefiting more clinical patients.

Scored Balloon for Recurrent Stenosis in AVG Outflow Tract
Peng Hongying, Xu Xiang from Baiyun Hospital Affiliated to Guizhou Medical University

Patient Information
Basic Information:Elderly Male, 71 Years Old.
Chief Complaint:Maintenance hemodialysis for 6+ years, poor fistula function for 1 week.
History of Present Illness:More than 6 years ago, the patient was diagnosed with "chronic kidney disease stage 5" and started maintenance hemodialysis treatment via a right internal jugular vein TCC, three times per week, continuing regularly until now. Over 2 years ago, the patient underwent a "left upper limb arteriovenous graft (AVG) formation surgery" under brachial plexus anesthesia at our hospital. One month later, after the AVG had matured, it was used for maintenance hemodialysis treatment, three times per week. One week ago, during dialysis, the patient experienced elevated venous pressure accompanied by prolonged post-dialysis bleeding time, without swelling or pain in the limb on the side without the AVG. The pump-controlled blood flow rate was 220 ml/min.
Past Medical History:A history of type 2 diabetes for over 20 years, hypertension for over 15 years, and cerebral infarction for over 8 years.
Physical Examination:The general condition is good. A "U"-shaped loop of subcutaneous prosthetic vessel (brachial artery-basilic vein) is visible from the left forearm to the inner upper arm. The pulsation of the entire prosthetic vessel can be palpated, and a high-pitched murmur can be heard at the venous anastomosis.
Admission Diagnosis:
Stenosis of Left Upper Limb Arteriovenous Graft Fistula
Chronic Kidney Disease Stage 5, Hemodialysis Status
Type 2 Diabetes Diabetic Nephropathy
Hypertension
Old cerebral infarction
Previous interventional treatment
Time | Main Treatment Process |
September 2018 | Established left forearm AVF, right internal jugular vein TCC for maintenance hemodialysis treatment. |
January 2019 | Left forearm AVF occlusion, perform left upper arm AVF |
February 2019 | Occlusion of the left upper arm AVF, continue maintenance dialysis using the right internal jugular vein TCC. |
February 2022 | Established AVG between the brachial artery and basilic vein in the left forearm, and began using AVG while successfully removing the TCC from the right neck in March of the same year. |
November 2022 | PTA Treatment for Venous Outflow Tract Stenosis in Forearm AVG |
June 2023 | Left forearm AVG venous outflow tract stenosis with thrombosis treated by AVG thrombolysis + PTA |
December 2023 | PTA Treatment for Stenosis of the Venous Outflow Tract in Left Forearm AVG |
April 2024 | Elevated venous pressure during dialysis accompanied by prolonged hemostasis time, ultrasound suggests venous outflow tract stenosis |
Preoperative Analysis
Preoperative Analysis:Combined with vascular ultrasound assessment, AVG reflux vein stenosis is considered, mainly caused by intimal hyperplasia. Planning to perform ultrasound-guided balloon angioplasty of the left upper limb arteriovenous graft.
Surgical Objective:
Main Objectives:Relieve Stenosis of the Venous Outflow Tract in Artificial Vessels;
Secondary Objectives:Using a scored balloon to evenly tear the hyperplastic intima and media, reducing the occurrence of late-stage refractory stenosis and improving the long-term patency rate of the fistula.
Surgical Strategy/Plan:Under ultrasound guidance, puncture the venous end of the artificial arteriovenous fistula, insert a 6F vascular sheath, and pass a 0.035 guidewire through the stenotic segment of the venous outflow tract. The target lesion is severely narrowed. First, use an ordinary balloon to pre-dilate the stenotic vessel segment, then switch to a scoring balloon to begin dilating the stenotic vessel segment.
Surgical Procedure
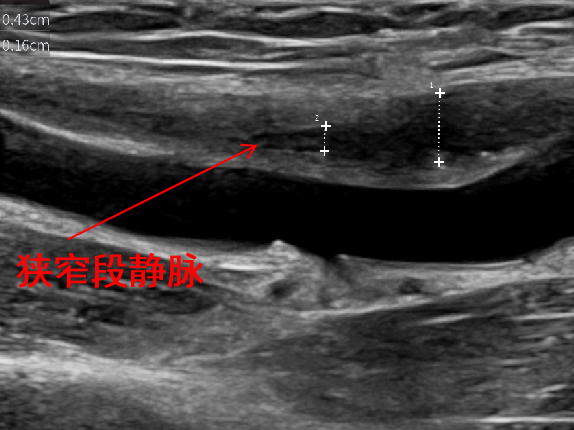
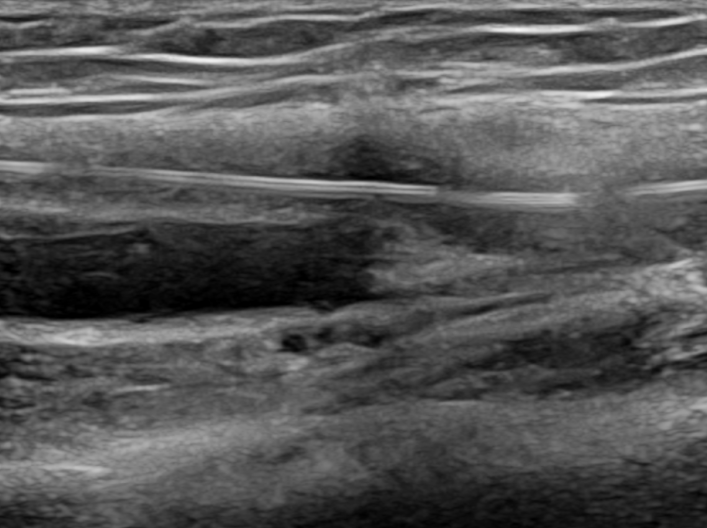
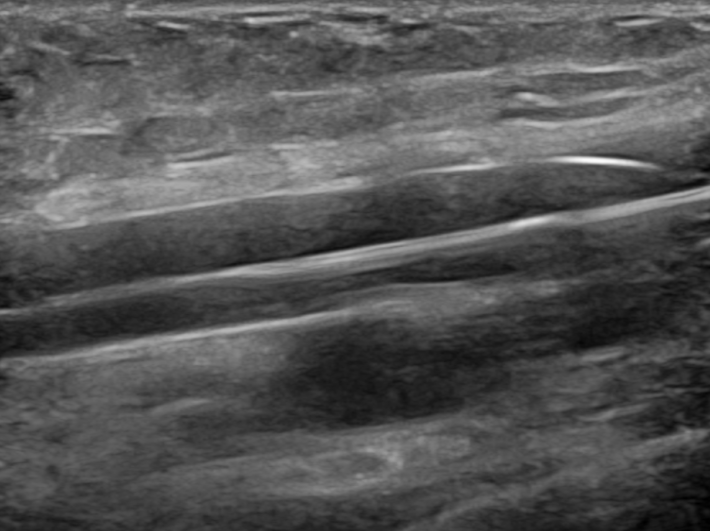
Severe stenosis near occlusion of AVG venous outflow tract, with the narrowest inner diameter of 1.6mm.
The stenotic segment is approximately 63% narrower compared to the diameter of the surrounding normal blood vessels.
Preoperative measurement of brachial artery blood flow was approximately 510 ml/min.
Under ultrasound guidance, a 6F sheath was inserted into the venous end of the artificial vessel, while 15mg of heparin injection was administered. A 0.035 guidewire passed through the stenosis at the venous outflow tract of the AVG.
0.035 guidewire successfully passed through the stenotic site of the outflow tract
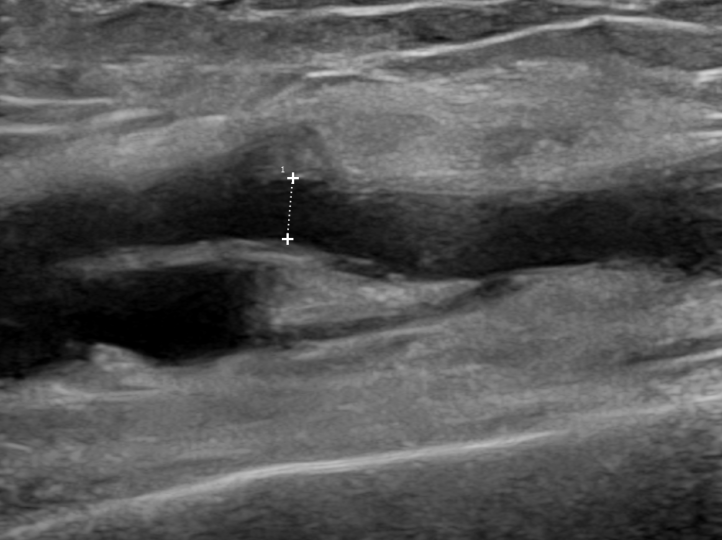
Pre-dilation with a 5mm high-pressure balloon
After the dilation, the stenosis improved compared to before, but there was still significant rebound.
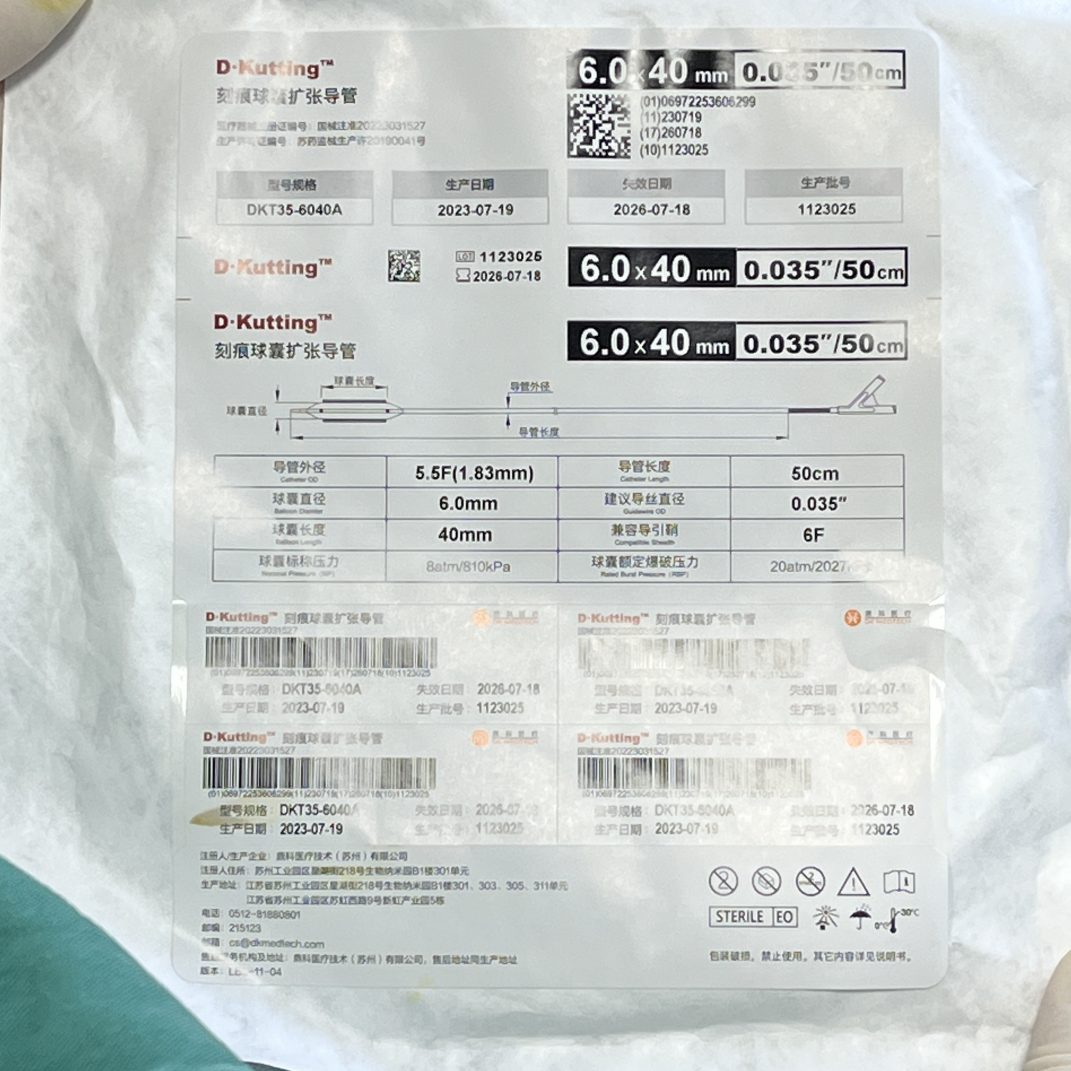
Re-expanded using the DK Medtech 6.0×40mm scored balloon, DKutting.
The narrowed part was dilated again with a scored balloon at 20 atm for 3 minutes.
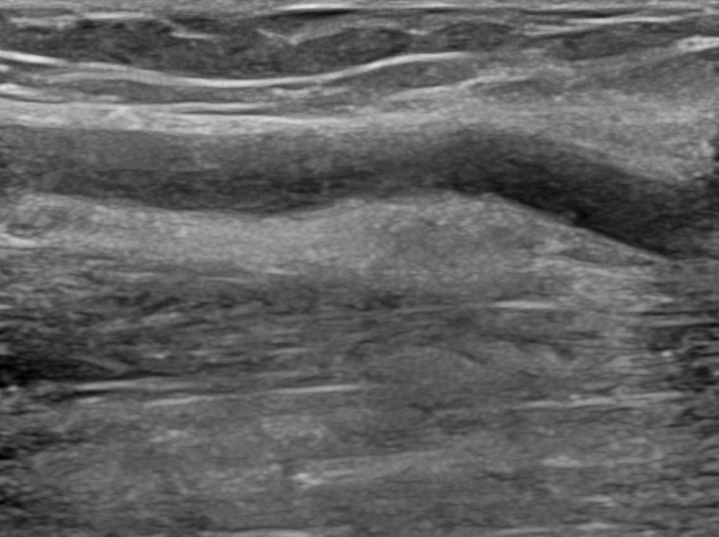
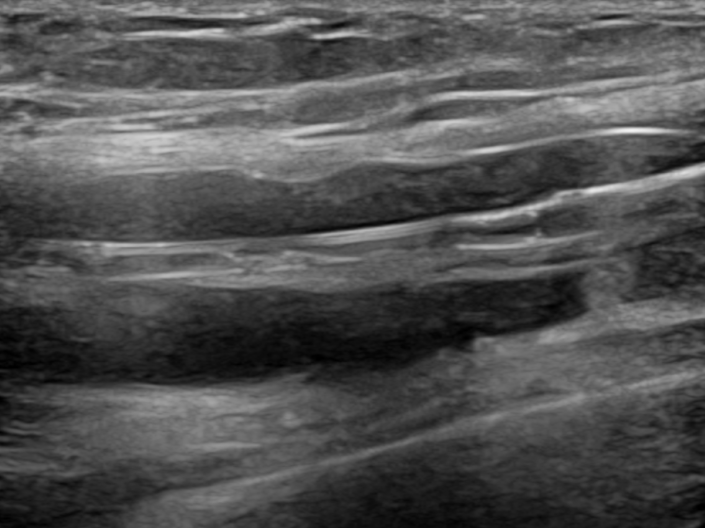
After dilation, the stenosis was significantly improved compared to before.
The inner diameter of the original narrowest part is 3.2mm, with recoil less than 30%.
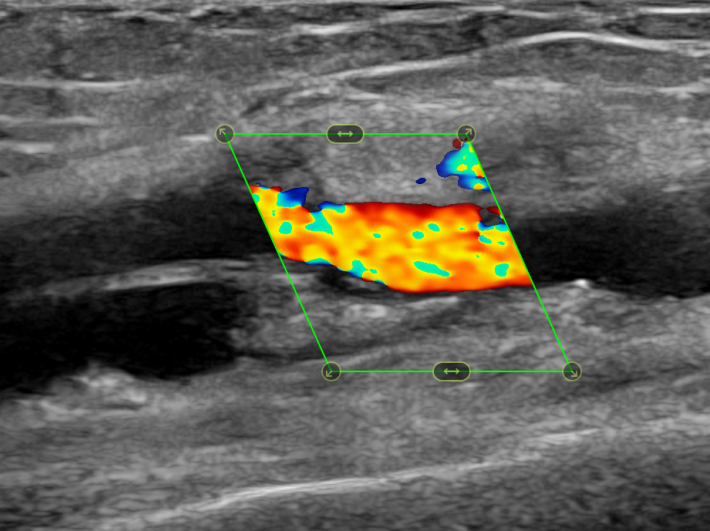
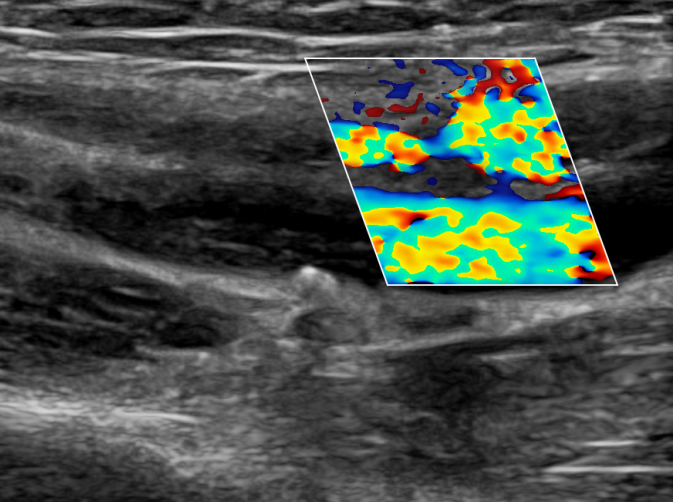
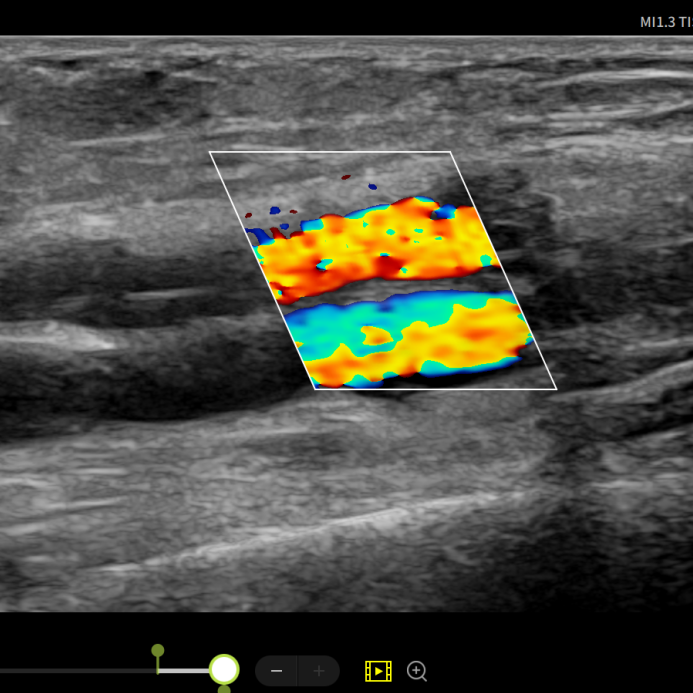
Postoperative Blood Flow Signal Filling
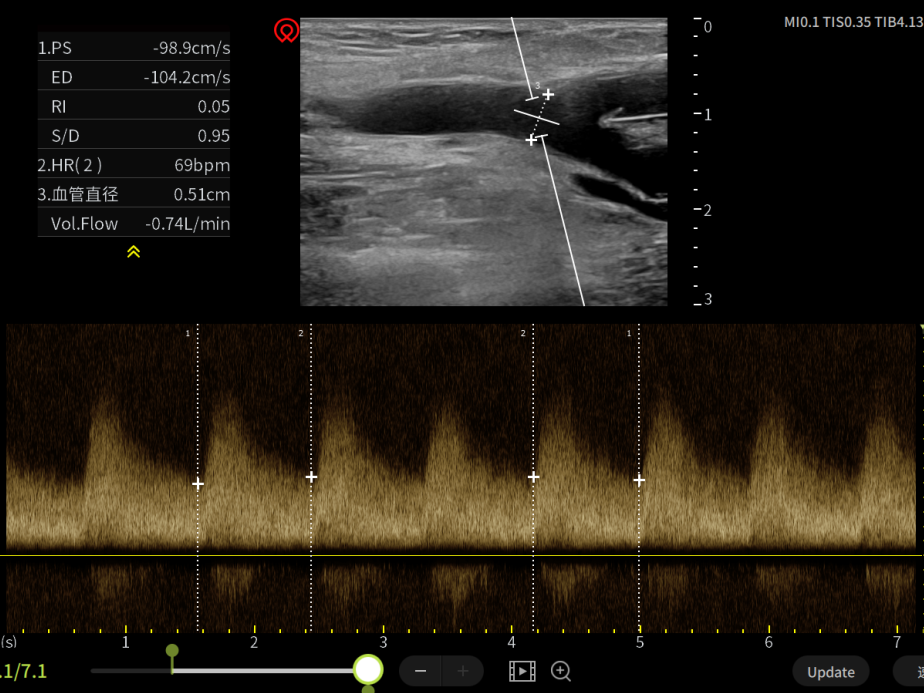
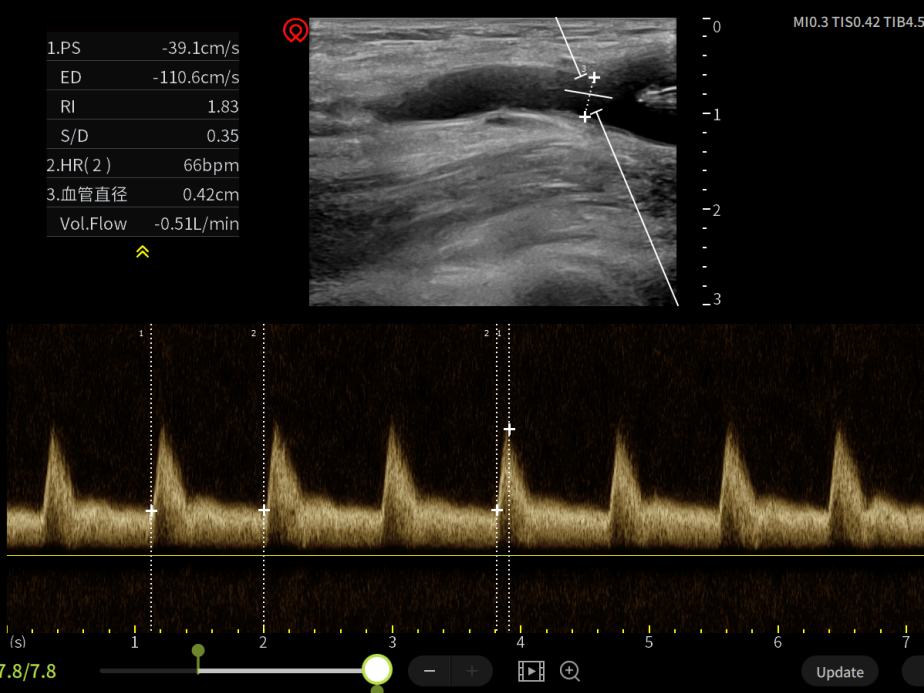
Postoperative measurement of brachial artery blood flow was approximately 740ml/min, and the venous pressure during dialysis was normal on the second day after surgery.
Follow-up
Discharge Status:
Postoperative patients had good thrill in their internal fistula, normal venous pressure during dialysis the next day, and a pump-controlled blood flow rate of 250ml/min. The hemostasis time was less than 15 minutes after dialysis.
Instructed to revisit the vascular access clinic 3 months post-operation.
Case Summary
Case Characteristics:Repeated stenosis of the venous outflow tract in arteriovenous grafts, accompanied by intimal hyperplasia.
Surgical Strategy/Technical Key Points:The 6mm scored balloon D-Kutting dilation treatment not only easily relieves stenosis compared to a regular 7mm balloon, but also prevents irregular tearing of the vascular intima, reducing the occurrence of refractory stenosis in the later stage.
Features/Usage Tips of the Device:Under ultrasound guidance, the sheath was proficiently inserted to avoid repeated puncture damage to the artificial blood vessel; before starting dilation, it was ensured that the balloon covered the target lesion site, and after the balloon was inflated, constant attention was paid to whether the balloon had shifted; the maintenance time after dilation needed to be more than 60 seconds to ensure the scoring elements were fully and evenly torn.

Introduction of Experts


Professor Peng Hongying
Surgeon of This Case
Vice President of Baiyun Hospital Affiliated to Guizhou Medical University, Director of the Nephrology and Rheumatology Department, Chief Physician, Master's Graduate Supervisor, Senior Visiting Scholar at Peking University, Innovative Leading Scholar at Peking Union Medical College.
Standing Committee Member of the Kidney Disease Rehabilitation Committee of the Chinese Association of Rehabilitation Medicine; Standing Committee Member of the Blood Purification Committee of the Chinese Research Hospital Association; Executive Director of the Kidney Disease Branch of the China Association for Promoting Traditional Chinese Medicine Research; Vice Chairman of the Nephrology Committee of the Guizhou Province Integrated Traditional Chinese and Western Medicine Association; Vice Chairman of the Clinical Nephrology Immunology Branch of the Guizhou Province Immunology Society; Vice Chairman of the Nephrology Committee of the Guizhou Province Traditional Chinese Medicine Association; Review Expert for the Center for Degree and Graduate Education of the Ministry of Education.
Long-term engagement in the clinical, teaching, and research work of kidney diseases, blood purification, and rheumatic immune diseases, with rich experience.Proficient in the diagnosis and treatment of various diseases, critical conditions, and complex疑难diseases at the undergraduate level.Awarded the Second Prize of the Guizhou Medical Association Science and Technology Award.Hosted and participated in more than 10 national, provincial, and municipal scientific research projects, published over 50 papers, co-authored 5 books and university textbooks, and obtained 4 patents.

Dr. Xu Xiang, Attending Physician
Surgeon of This Case

Department Introduction


The Nephrology and Rheumatology Department of Baiyun Hospital Affiliated to Guizhou Medical University is a unit of the National Clinical Research Center for Kidney Diseases' Chronic Kidney Disease Full-Process Management Center; a key member unit of the Guizhou Kidney Disease Quality Control Center; a core unit of the Guizhou Clinical Research Center for Kidney Diseases; a training base for specialized nurses in blood purification in Guizhou Province; Fresenius Blood Purification Education Academy; a member unit of the Nephrology Alliance of West China Hospital of Sichuan; currently, the ward has 38 open beds, and the hemodialysis center is equipped with 63 dialysis machines, one ultrasound machine, one phase contrast microscope, one body composition analyzer; two high-flow oxygen machines, two real-scenario operation training machines for specialized nurses, an advanced cardiopulmonary resuscitation defibrillation simulator, central venous puncture model, simulated arm, and other equipment. The medical team consists of 48 people, including six senior titles, 15 intermediate titles, and one full-time hemodialysis engineer, forming a vibrant team. In recent years, the department has participated in six national multi-center studies, led more than 20 provincial, municipal, and district-level projects; won a second prize for scientific and technological achievements from the Guizhou Medical Association; participated in the writing of industry standards (guidelines) and textbooks more than ten times, obtained 19 patents; three municipal new technologies; more than ten district-level new technologies; published more than ten SCI papers. The department carries out diagnosis and treatment of various primary and secondary kidney diseases, performs renal biopsy, urine red blood cell phase detection, peritoneal dialysis catheter insertion/removal, colon dialysis, blood purification, establishment and maintenance of vascular access, and integrated management of chronic kidney disease, achieving remarkable results. In addition to maintenance dialysis for uremia, the hemodialysis center also applies blood purification to the treatment and rescue of critically ill patients in multiple clinical disciplines such as severe immune system diseases, multi-organ failure, sepsis, refractory heart failure, liver failure, severe pancreatitis, acute drug and poison poisoning, improving the success rate of rescuing critically ill patients.
Copyright Statement: This platform aims to help medical and health professionals better understand the latest developments in relevant disease areas. The information published on this platform does not imply agreement with its descriptions or viewpoints, but is merely intended to provide more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will address them as soon as possible. The information is solely for medical and health professionals to stay informed, and such information cannot replace professional medical guidance in any way, nor should it be regarded as medical advice. If such information is used for purposes other than staying informed, this platform and the author shall not bear any related responsibilities.Contact Email for Cooperation:vascular@edoctor.work。
