Innovative Use of Soft-Tip CTO Guidewire for Challenging In Situ Aortic Arch Branch Reconstruction in Two TEVAR Cases by Prof. Chang Guangqi and Prof. Li Zilun’s Team

Percutek Therapeutics
Developer of Minimally Invasive Cardiovascular Treatment Devices

Today, I will introduce to youProfessor Chang Guangqi / Li Zilun's Team from the First Affiliated Hospital of Sun Yat-sen UniversityBrought bySharing of Two Challenging In-situ Reconstruction TEVAR Surgeries for Supra-aortic BranchesOne case of penetrating aortic ulcer, with only a 15-degree angle between the left subclavian artery and the aortic arch. Another case involved Type I endoleak after single-branched stent TEVAR. Using only a 0.018" CTO guidewire with a soft tip to penetrate the membrane, Professor Chang Guangqi and Professor Li Zilun’s team successfully performed in-situ supra-aortic reconstruction.
Case 1
Medical History Introduction
Gender:Male
Age:74 years old
Chief Complaint:Aortic ulcer found during examination half a month ago.
History of Present Illness:Half a month ago, an examination at another hospital revealed a penetrating aortic ulcer. The patient subsequently visited our emergency department for further treatment and was diagnosed with a penetrating aortic ulcer and hypertension.
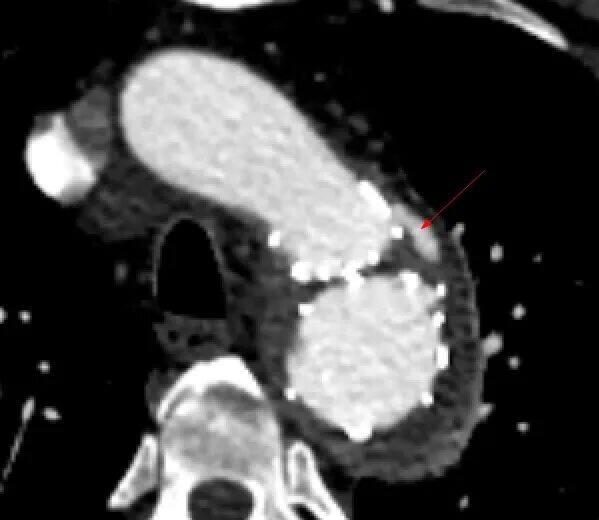
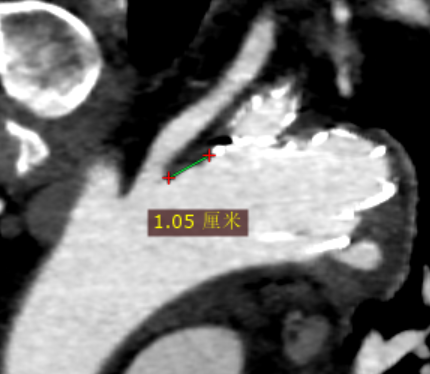
Preoperative CTA Details:Thrombus formation with partial penetrating ulcer in the aortic arch, left subclavian artery, and thoracoabdominal aorta; lesion size approximately 20*30mm. The aortic diameter at the posterior margin of the left common carotid artery is 33.5mm, and the aortic diameter at the anterior margin of the left subclavian artery is 32mm. The distance between the posterior margin of the left common carotid artery and the anterior margin of the left subclavian artery is 8mm. The distance between the posterior margin of the left common carotid artery and the proximal end of the penetrating ulcer is approximately 15mm. There is mural thrombus at the root of the left subclavian artery.

Preoperative CTA 3D Reconstruction
Preoperative CTA Cross-Section
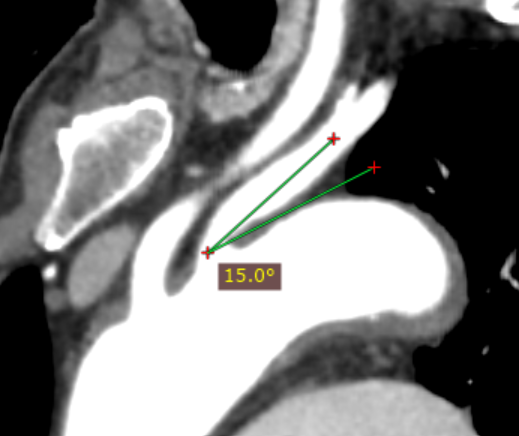
15-degree angle
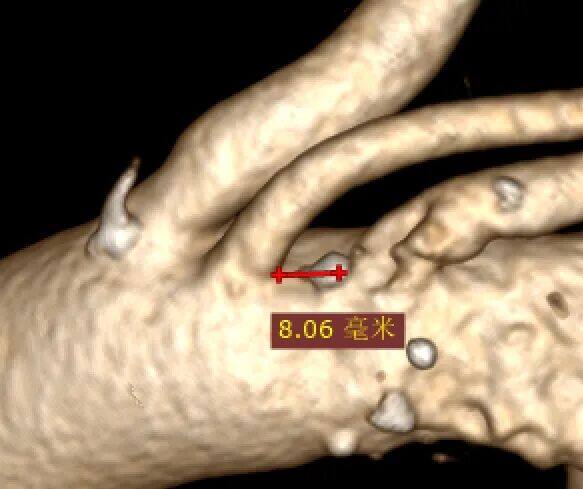
Subclavian Distance
Preoperative CTA 3D Reconstruction
Surgical Difficulties
The left subclavian artery originates from the aortic arch at a 15° acute angle, posing a challenge for in-situ fenestration angle control during surgery.
Thrombus attached to the aortic arch and left subclavian artery with penetrating ulcer; the lesion is located at the anterior wall of the root of the left subclavian artery, with insufficient proximal anchoring zone.
Surgical Plan Design
Endovascular Repair of Thoracic Aortic Stent Graft Directly Covering the Left Subclavian Artery:Simple operation, clear effect, but covering the left subclavian artery may cause clinical manifestations of posterior circulation ischemia and upper limb ischemia in patients.
Endovascular Repair of Thoracic Aortic Stent Graft + Left Subclavian Artery Chimney Technique:The surgical procedure is relatively simple, but there is a higher possibility of endoleaks. The effect on arch dissection aneurysms is not ideal, and the mid-to-long-term outcomes are suboptimal.
Endovascular Repair of Thoracic Aortic Stent Graft with In Vitro Fenestration:The tumor closure has a good effect, which can preserve the original hemodynamic characteristics, but the operation is complex. The stent needs to be modified preoperatively according to the measurement results, which is time-consuming. Intraoperatively, precise alignment of the ultra-selection window is required, posing higher risks.
Single-branched Stent Thoracic Endovascular Aortic Repair:The tumor closure effect is good, but the angle between the subclavian artery and the aortic arch is too small, increasing the risk of branch stent occlusion in the long term.
Plan Five
Endovascular Repair of Thoracic Aortic Stent Graft + In-situ Fenestration:The tumor closure is effective, and there is no need to modify the stent before surgery. However, the in-situ fenestration of traditional aortic covered stents requires advanced interventional devices such as in-situ fenestration needles, lasers, and biopsy needles for special membrane-piercing procedures.
After comprehensive evaluation, we choosePercutek Therapeutics Thoracic Aortic Stent GraftPerform endovascular repair and reconstruct the left subclavian artery using the in-situ fenestration technique.
Surgical Procedure
Endovascular Repair of Penetrating Ulcer of the Aortic Arch + Fenestrated Stent Reconstruction of the Left Subclavian Artery
1. A pigtail catheter was introduced via the left brachial artery sheath for ascending aortography: Blood flow in both common carotid arteries was unobstructed, blood flow in the left subclavian artery was unobstructed with slight stenosis at the ostium, both vertebral arteries were patent and of equal potential, and the Willis circle was intact. A penetrating ulcer was observed on the anterior wall near the lesser curvature distal to the ostium of the left subclavian artery. It was decided to perform endovascular repair of the aortic arch penetrating ulcer + fenestrated stent reconstruction of the left subclavian artery.
Bilateral vertebral arteries are patent and equipotential, Willis circle is intact.
A penetrating ulcer is visible on the anterior wall side of the distal small curve beyond the origin of the left subclavian artery.
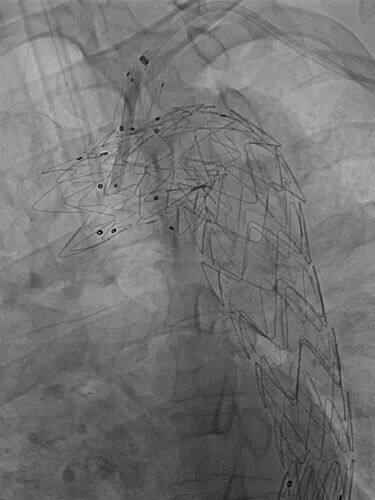
2. The left brachial artery was replaced with a hard mud鳅 guidewire, and a 7F Fustar steerable sheath was used, with the tip of the sheath placed at the origin of the left subclavian artery. A Back-up Meier guidewire was introduced via the right femoral artery and advanced into the ascending aorta to form a loop for support. Along this guidewire, a Percutek Therapeutics PTBS3632180 covered stent was delivered. The leading edge of the covered stent was aligned with the posterior edge of the origin of the left common carotid artery, and the stent was deployed. Angiography showed: precise stent positioning, good isolation of the penetrating ulcer in the aortic arch, no impact on blood flow in the left common carotid artery, and delayed visualization of the left subclavian artery.
The front edge of the Percutek Therapeutics PTBS3632180 stent graft is aligned with the left margin of the left common carotid artery orifice.
Angiography confirmed accurate stent placement and smooth blood flow in the left common carotid artery after the release of the covered stent.
3. A Fusmart steerable catheter was introduced into the left brachial artery sheath, and the catheter tip was positioned directly opposite the covered stent at the aortic arch. A Connect 250T guidewire was advanced through the catheter to successfully puncture the membrane. The TrailBlazer support catheter was then advanced into the main stent body. Sequential dilation of the fenestrated area was performed using a 3-40mm Armada balloon, a 5-30mm Sterling balloon, and an 8-40mm Mustang balloon. An 8-58mm Lifestream covered balloon-expandable stent was advanced over the guidewire, with its distal end placed approximately 10mm into the covered stent before deployment.
Adjusting the deflectable catheter head is crucial for the stent graft at the aortic arch.
Multi-angle fluoroscopy confirms adjustable catheter head is properly aligned with the covered stent.
The Connect 250T guidewire was used to successfully puncture the membrane and enter the main stent, then advanced down to the ascending aorta.

Multi-angle透视 Confirms Successful Membrane Rupture
Follow-up 5-30mm Sterling Balloon Dilation Window Opening

Follow-up on 8-40mm Mustang Balloon Dilation Window Opening

Multi-angle Confirmation of Balloon Dilation

Left subclavian angiography confirmed the fenestration morphology
Continue 8-40mm Mustang Balloon Dilation Window Opening
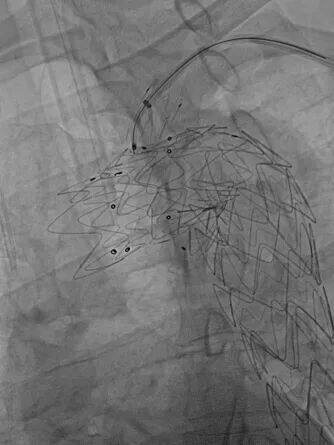
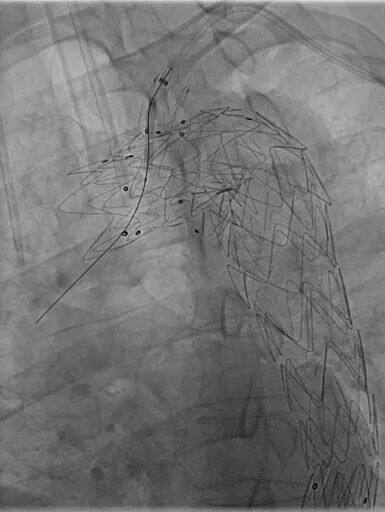
Placement of 8-58mm covered balloon-expandable stent approximately 10mm into the covered stent

Balloon-Expandable Branch Stent
4. Final angiography showed: all stents were in good position and shape, the penetrating ulcer of the aortic arch was completely isolated without endoleak, and the blood flow of the brachiocephalic artery, left common carotid artery, and left subclavian artery was unobstructed.
Contrast of the Left Subclavian Artery, Blood Flow Through the Branch Stent is Unobstructed
Final Angiography
Postoperative Follow-up
Before discharge, the patient underwent CTA examination, which showed that the penetrating ulcer of the aortic arch was well isolated without endoleak; the branch stent was patent with good morphology; and the vertebral artery blood supply was good.
Postoperative CTA 3D Reconstruction
Case 2
Medical History Introduction
Gender:Male
Age:44 years old
Chief Complaint:Abdominal pain for about 20 days after aortic dissection surgery.
History of Present Illness:The patient suddenly developed chest and back pain about one month ago and was diagnosed with aortic dissection at a local hospital. The patient underwent single-branched stent TEVAR surgery and was discharged 20 days ago. Three days after discharge, the patient developed upper abdominal distension and colic symptoms. The patient came to our emergency department for further diagnosis and treatment and was diagnosed with type I endoleak after endovascular repair of aortic dissection.
Preoperative CTA Details:Type I endoleak formation at the stent level of the aortic arch, with an aortic diameter of approximately 27mm at the posterior edge of the left common carotid artery, and a distance of 10mm between the posterior edge of the left common carotid artery and the anterior edge of the left subclavian artery.
Preoperative CTA 3D Reconstruction
Preoperative CTA Cross-Section
Schematic Diagram of Endoleak
Schematic Diagram of the Anchoring Area
Preoperative CTA 3D Reconstruction
Surgical Difficulties
Stent wrinkles on the concave side after single-branched stent TEVAR, Type I endoleak occurred, and insufficient proximal anchoring zone.
After the single-branched stent TEVAR procedure, a branched stent was implanted in the left subclavian artery. The ostial stenosis of the left subclavian artery posed challenges for controlling the angle during the in-situ fenestration.
Surgical Plan Design
The patient has already been implanted with a single-branched stent. Considering the medium- to long-term treatment outcomes and the difficulty of intraoperative manipulation, after comprehensive evaluation, we also chose thoracic endovascular aortic repair (TEVAR) and performed in-situ branch reconstruction to rebuild the left subclavian artery.
Surgical Procedure
1. Angiography via a pigtail catheter introduced through the left brachial artery sheath: Blood flow is unobstructed in both common carotid arteries, and in the left subclavian artery with slight stenosis at the ostium. The left vertebral artery shows slight dominance but remains patent; the Willis circle is intact. Contraction along the lesser curvature of the aortic arch and descending aortic stent is visible, with Type Ia endoleak observed near the proximal end of the stent. The false lumen is significantly opacified with substantial flow.
The Circle of Willis is intact, with the left vertebral artery being slightly dominant and patent.
Visible shrinkage on the concave side of the aortic arch and descending aorta stent
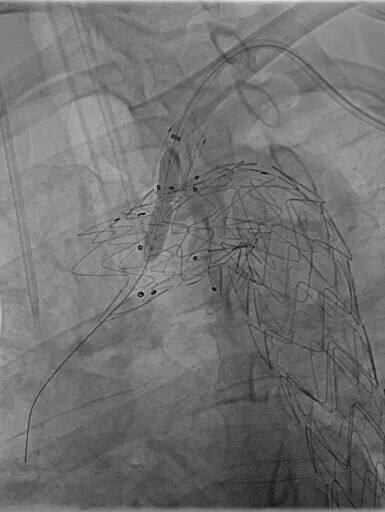
2. The tip of the 7F long sheath of the left brachial artery was placed at the ostium of the left subclavian artery. A Back-up Meier guidewire was introduced via the left femoral artery and advanced into the ascending aorta to form a loop for support. Along this guidewire, the Percutek Therapeutics PTBS3228180 covered stent was delivered. The leading edge of the covered stent was aligned with the posterior edge of the ostium of the left common carotid artery before stent deployment. Angiography showed: precise stent positioning, good exclusion of the false lumen of the dissection, no impact on blood flow in the left common carotid artery, delayed visualization of the left subclavian artery, and retrograde blood flow in the left vertebral artery.
Implantation of Percutek Therapeutics PTBS3228180 stent graft, flush with the posterior edge of the left common carotid artery origin.
Angiography after the deployment of Percutek Therapeutics' stent graft showed precise stent positioning, good exclusion of the false lumen in the dissection, and no endoleak.
3. The left brachial artery was replaced with a Fusmart adjustable catheter. After passing through the original branch stent, the tip was placed at the opening of the left subclavian artery. The catheter tip was adjusted to face the covered stent at the aortic arch. Along this catheter, a Connect 250T guidewire was inserted to successfully puncture the membrane. Then, a 3-40mm Sterling balloon was advanced into the main body of the stent. After balloon dilation, a 4-40mm Pesseo balloon, a 6-30mm Sterling balloon, and a 7-60mm Mustang balloon were used successively for graded expansion and shaping of the fenestrated area.

Adjust the deflectable catheter tip to face the covered stent.
Multi-angle confirmation of adjustable catheter head alignment with covered stent
Connect 250T Guidewire with Adjustable Curved Catheter for Membrane Puncture

Guidewire advanced to the ascending aorta
Follow-up 3-40mm Sterling Balloon Dilation Window Opening
Follow-up 4-40mm Passeo Balloon Dilation Window Opening
Follow-up on 6-30mm Sterling Balloon Dilation Window Opening
Follow-up 7-60mm Mustang Balloon Dilation Window Opening and Multi-angle Observation
4. A 9-38mm Lifestream covered balloon-expandable stent was advanced over the guidewire, with the distal end entering approximately 5mm into the covered stent through the fenestration for deployment.
The blood flow of the left subclavian artery, left vertebral artery, and left brachial artery is unobstructed with normal velocity.
Ascending Aortography
Intraoperative Procedures

— Summary of Case Experience —
The two cases shared in this presentation include: one case where the ulcer involves the root of the left subclavian artery, and the left subclavian artery is nearly parallel to the aortic arch. Effectively reconstructing the supra-aortic branches during endovascular aortic repair while ensuring long-term prognosis poses a challenge. The other case involves Type I endoleak after single-branched stent thoracic endovascular aortic repair with thrombosis occurring within the subclavian branch stent. Choosing a surgical approach that preserves the supra-aortic branches while resolving the endoleak issue also presents a challenge.
Both cases selected the Percutek Therapeutics thoracic aortic stent graft for endovascular repair. This innovative stent graft is currently the only product on the market capable of achieving in-situ reconstruction solely through guidewire penetration. It offers precise positioning, no endoleaks, and during the procedure, the membrane can be easily punctured using only a 0.018" CTO guidewire with a soft tip. The fenestration area of the graft is easy to penetrate and expand, and after stent implantation, the structure is well-formed with no membrane leakage. The in-situ branch reconstruction aortic endovascular repair procedure is simple to perform, reducing the requirements for the selection of endovascular tools. The immediate outcomes of aortic endovascular repair and left subclavian artery reconstruction in both cases met the preoperative planning expectations. Short-term, mid-term, and long-term effects remain to be further observed.
Key Instruments for This Case:Percutek Therapeutics Thoracic Aortic Stent Graft, Connect 250T Guidewire, Fusmart Adjustable Bend Catheter.

Professor Guangqi Chang
Professor, Chief Physician, Doctoral Supervisor and Postdoctoral Mentor, Director of the Vascular Surgery Department (National Key Discipline and Key Clinical Specialty) at the First Affiliated Hospital of Sun Yat-sen University, Director of the Vascular Thyroid Breast Center at the First Affiliated Hospital of Sun Yat-sen University, Director of the Sun Yat-sen University Vascular Surgery Research Center. Renowned Lingnan Physician, Leading Talent in Guangdong Province Medicine. Chairman of the Southern China Vascular Conference.
Academic Positions: Vice President of the Vascular Surgery Branch of the Chinese Medical Doctor Association, Vice President of the Vascular Surgery Branch of the Cross-Straits Medical and Health Exchange Association, Vice Chairman of the Vascular Surgery Professional Committee of the National Cardiovascular Disease Expert Committee, Vice Chairman of the Vascular Surgery Branch of the China International Exchange Promotion Association for Medical and Healthcare, Vice Chairman of the Vascular Medicine Branch of the Chinese Research Hospital Association, Vice Chairman of the Vascular Device Branch of the China Medical Device Industry Association, Standing Committee Member of the Interventional Physician Branch of the Chinese Medical Doctor Association, Member of the Tissue Repair and Regeneration Branch of the Chinese Medical Association, Vice President of the Guangdong Clinical Medicine Association, Former Chairman of the Vascular Surgery Branch of the Guangdong Medical Association, Chairman of the Guangdong-Hong Kong-Macao Greater Bay Area Vascular Surgery Alliance, Future Chairman of the Vascular Medicine Branch of the Guangdong Medical Doctor Association, Standing Director and Chairman of the Vascular Medicine Committee of the Guangdong Health Management Society, Senior Academician of the Hong Kong Academy of Medicine, International Member of the American Society for Vascular Surgery (SVS). Deputy Editor-in-Chief and Editorial Director of the Chinese Journal of Vascular Surgery, Deputy Editor-in-Chief and Editorial Director of the Chinese Journal of Vascular Surgery (Electronic Edition), Editorial Board Member of the Annals of Vascular Surgery.
With over 30 years of experience in vascular surgery, he has created multiple internationally precedent-setting surgical cases. In China, he was the first to propose a new staging method for aortic dissection, suggesting that endovascular treatment during the subacute or chronic phase of aortic dissection can significantly reduce in-hospital mortality. His achievements have been featured in various media outlets, including Science and Technology Daily, People's Daily (Health Client), Science and Technology China, Yangcheng Evening News, Southern Daily, Information Times, Guangzhou Daily, Southern Metropolis Daily, Guangdong Television, and Guangzhou Television.
Published over 100 SCI and Chinese core journal papers as the first or corresponding author, won one First Prize of Huaxia Medical Science and Technology Award and one First Prize of Guangdong Provincial Science and Technology Progress Award, presided over five projects funded by the General Program of the National Natural Science Foundation of China and three provincial or ministerial level projects. Authored and translated four books, and co-authored five monographs.
Successively awarded the honorary titles of "Good Doctor of Yangcheng", "Famous Doctor of Lingnan", and "Good Doctor of Safe China". In 2018, selected as a leading medical talent in Guangdong Province, and in 2019, received the "Health Guardian—Outstanding Contribution Award" from China Health Television. Awarded the title of "2023 (9th) Annual Figure of Renowned Doctors with Excellent Medical Skills and Ethics".

Professor Li Zilun
The First Affiliated Hospital of Sun Yat-sen University,Chief Physician, Postdoctoral Cooperation Supervisor, Doctoral Supervisor, Master's Supervisor,Deputy Director of the Vascular Surgery Department at the First Affiliated Hospital of Sun Yat-sen University.Graduated from the Seven-Year Program at Sun Yat-sen Medical School, and jointly trained for a Ph.D. by Sun Yat-sen University and Mayo Clinic.
Deputy Chairman of the Youth Committee of the Vascular Medicine Professional Committee of the Chinese Research Hospital Association;Vice Chairman of the First Committee of the Vascular Surgery Branch of the Guangzhou Medical Association;Editorial Board Member of the Second Editorial Committee of the Chinese Journal of Vascular Surgery (Electronic Edition);Communicating Editor and English Editor of the Chinese Journal of Vascular Surgery.
Hosted 11 scientific research funds, including 3 National Natural Science Foundation projects, 2 Provincial Natural Science Foundation projects, and 1 Municipal Key project.Selected for Guangdong Special Support Plan's "Hundred, Thousand, and Ten Thousand Talents Project" Young Top Talents, Zhujiang Technology Rising Stars, and other talent programs.
Published 31 English academic papers as the first or corresponding author (including co-corresponding author) in internationally renowned journals such as *Cell Metabolism* (2 papers), *STTT*, *Hypertension*, *ATVB* (2 papers), *Autophagy*, and *JAHA*, with a cumulative citation count of approximately 1,400 times.

In 1964, the Department of Vascular Surgery at the First Affiliated Hospital of Zhongshan Medical College, one of the earliest vascular surgery departments in China, was officially established. Under the leadership of renowned surgical experts Professor Guorui Chen and Professor Yongjie Lin, the department grew from small to large, from weak to strong, gradually developing into a well-known vascular surgery department in China and the leading one in South China. After Professor Shenming Wang became the director of the vascular surgery department in 1997 and the academic leader in 2004, he actively adjusted the academic development direction, introduced several of the latest treatment technologies from abroad, and organized various national training courses to promote their application. Within a relatively short period, the vascular surgery department of the First Affiliated Hospital of Zhongshan (Zhongshan No.1) developed into a leading vascular surgery center in China. After Professor Guangqi Chang became the new director of vascular surgery in 2014, he continued to expand and make progress, further strengthening the overall capabilities of our hospital's vascular surgery department and maintaining its leading position among vascular surgery centers in China. In December 2003, the Vascular Surgery Research Center of Sun Yat-sen University was established; in March 2005, the first independent vascular surgery branch in China — the Vascular Surgery Branch of the Guangdong Medical Association — was founded; in 2000, vascular surgery became a key discipline of Class A in Guangdong Province; in 2001, the Department of General Surgery of Zhongshan No.1 Hospital, with vascular surgery as one of its main development directions, was rated as a national key discipline by the National Education Commission, and passed the reevaluation for the national key discipline in 2007; in 2012, it was again rated as a national clinical key specialty by the Ministry of Health, and passed the reevaluation in 2017; in 2014, this center was awarded the Vascular Disease Engineering Technology Research Center of Guangdong Province Science and Technology Department, and in 2015, it was approved by the National Development and Reform Commission to establish the National-Local Joint Engineering Laboratory for Vascular Disease Diagnosis and Treatment Technology, passing the reevaluation in 2020. In 2020, it was rated as a core unit of the National Radiology and Treatment Clinical Research Center. Currently, under the leadership of Professor Shenming Wang, the academic leader, and Director Guangqi Chang, the center continues to aim at international and domestic top levels, formulating practical goals and research directions for discipline construction, actively building a high-level professional talent team, and maintaining its leading position in basic and clinical research in South China and its status as a top-tier academic level in China. The center has talents with high academic attainments in medical treatment, teaching, scientific research, and other aspects, including 14 practicing physicians, 2 non-invasive examination specialists, 22 nurses, 14 doctoral and master’s students, 10 postdoctoral fellows, and 3 research assistants. Among them, 7 have obtained senior titles above associate professor level, 6 are doctoral supervisors, and 8 have studied or trained at prestigious medical schools or vascular surgery centers in countries such as the United States, Australia, Japan, and Spain.
The medical service capacity of the Vascular Surgery Department at the First Affiliated Hospital of Sun Yat-sen University ranks first in Guangdong Province and the South China region. The discipline leader, Professor Wang Shenming, and the department director, Professor Chang Guangqi, are both renowned experts in the field of vascular surgery in China. They also respectively serve as the Honorary President and Vice President of the Vascular Surgery Physicians Branch of the Chinese Medical Doctor Association, and the former and current Chairmen of the Vascular Surgery Branch of the Guangdong Medical Association. Currently, the specialty reputation of the vascular surgery department at the First Affiliated Hospital of Sun Yat-sen University ranks among the top in China, making it a well-known vascular surgery research and clinical treatment center in China. Each year, our department secures more than four provincial and national scientific research funds, enrolls more than eight doctoral and master's students, accepts more than 12 visiting doctors from all over China, conducts more than one large-scale free clinic event, and holds more than eight training workshops on new technologies and standardized practices. The total number of participants attending the training workshops organized by our department exceeds 800 people. The China Southern Vascular Conference, jointly organized by the Vascular Surgery Research Center of Sun Yat-sen University and the Vascular Surgery Branch of the Medical Associations of eleven southern provinces, has successfully held sixteen sessions so far. The number of attendees has grown from an initial 60-plus to 4,700 now, making it one of the largest and most influential conferences in the field of vascular surgery in China.
The Vascular Surgery Department of the First Affiliated Hospital of Sun Yat-sen University admits more than 2,500 inpatients annually and performs over 2,000 surgeries each year. The main treatment areas include: aortic dissection, thoracic aortic aneurysm, abdominal aortic aneurysm, carotid body tumor, carotid artery stenosis, lower extremity arterial sclerosis occlusion, acute arterial embolism, large vessel vasculitis, deep venous valve insufficiency of the lower extremities, varicose veins of the lower extremities, deep vein thrombosis of the lower extremities, vascular injury, congenital arteriovenous fistula, thromboangiitis obliterans, and cavernous hemangioma, among others. Meanwhile, the vascular surgery department has introduced several new technologies, successfully treating many complicated and critically ill cases. Both the difficulty of the surgeries and the quality of their completion are at leading levels in China. These new technologies include: in-situ fenestration technology to reconstruct the three branches above the aortic arch for treating aortic arch diseases, branch stent technology to reconstruct the left subclavian artery for treating aortic dissection, "octopus" technology and branch stent technology for treating thoracoabdominal aortic aneurysms, external stent fenestration technology for treating juxtarenal abdominal aortic aneurysms, hybrid surgery for complex aortic arch lesions, chimney stent technology and periscope technology for treating complex aortic dissections, open surgery combined with autologous renal transplantation for treating juxtarenal abdominal aortic aneurysms, branch stent technology for reconstructing the internal iliac artery, open and endovascular treatment for complex abdominal aortic aneurysms, rapid thrombectomy combined with iliac vein stent implantation for treating acute deep vein thrombosis of the lower extremities, debulking technology plus drug-coated balloon treatment for refractory lower extremity arterial sclerosis occlusion, and more.
In the past five years, more than 100 papers have been published, including over 50 SCI papers. There are 10 SCI articles with IF>5.0. Currently, there are 14 ongoing funded projects, including 10 national scientific research funds. In the past five years, 10 authorized patents have been obtained. The clinical research project "Study on the Treatment and Pathogenesis of Aortic Aneurysms and Aortic Dissections" completed by this center after years of efforts has won both the first prize of the 2014 Guangdong Province Science and Technology Award and the first prize of the 2014 Huaxia Medical Science and Technology Award, marking that the research level of this center in the field of aortic disease research is already at the forefront in China.

END
Copyright Statement: This platform aims to help medical and health professionals better understand the latest developments in relevant disease areas. The information content published on this platform does not imply agreement with its descriptions or viewpoints, but is merely intended to provide more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will address them as soon as possible. This information is solely for medical and health professionals to stay informed, and such information cannot replace professional medical guidance in any way, nor should it be regarded as medical advice. If such information is used for purposes other than staying informed, this platform and its authors shall not bear any related responsibility.Contact Email for Cooperation:vascular@edoctor.work。
