Genentech's Breakthrough Study: TIGIT and PD-L1 Co-Blockade Emerges as a Promising Strategy in Cancer Immunotherapy

Genentech
Pharmaceutical R&D Manufacturer
On December 16, 2024, Ira Mellman's team at Genentech published a research article titled "TIGIT and PD-L1 co-blockade promotes clonal expansion of multipotent, non-exhausted antitumor T cells by facilitating co-stimulation" in the journal Nature Cancer. The study findings indicate,PD-1 and TIGIT inhibition contributes to the formation of a tumor-reactive CD8 T cell lineage in draining lymph nodes.And determine their immune fate in tumors, thereby improving therapeutic efficacy. Analysis of clinical trial samples suggests that similar mechanisms may also occur in cancer patients.
https://www.nature.com/articles/s43018-024-00870-6
TIGIT and PD-1 Blockade
01
In CD8 tumor-infiltrating lymphocytes (TILs), the expression of TIGIT and PD-1 is highly correlated. PD-1 primarily regulates the co-stimulation of CD28, while TIGIT and PD-1 jointly regulate the function of CD226, which is the activating counter-receptor of TIGIT. In addition to indicating exhaustion or commitment to exhaustion, the expression of PD-1 may also reflect the activation state of T cells. The extent to which checkpoint blockade, particularly the blockade of TIGIT alone or in combination with PD-1, can reprogram CD8 T cells committed to exhaustion pathways or prevent the commitment to exhaustion during development remains a critical unknown.
To answer these questions, the team employed a multi-chamber, multi-omics single-cell approach, analyzing over 245,000 T cells. The team studied not only the characteristics of CD8 T cells in dLNs and tumors but also those in the blood. Sampling these three key tissue compartments provided deeper insights into the spatial and temporal impacts of TIGIT and PD-1 blockade on T cell fate decisions.
Anti-PD-L1 and Anti-TIGIT Can Reshape CD8 T Cell Trajectories to Varying Degrees
02
After using anti-TIGIT therapy, gp70 Ccl5 cells in the blood migrate to the tumor and form the Ccl5.2 phenotype within the tumor. Ccl5.2 cells differentiate into Cytotox.2 cells, which further differentiate into other cytotoxic and mitotic (pre-exhaustion) phenotypes. Compared with anti-TIGIT and combination therapies, treatment with anti-PD-L1 and FTY720 results in a higher degree of differentiation of gp70 Cytotox.2 cells into other phenotypes. These results indicate that,Anti-TIGIT, especially in combination therapy, can promote an immune response characterized by the influx of tumor-specific Ccl5.1 T cells, whereas anti-PD-L1 and FTY720 treatments mainly induce the differentiation of existing Cytotox.2 T cells within the tumor.
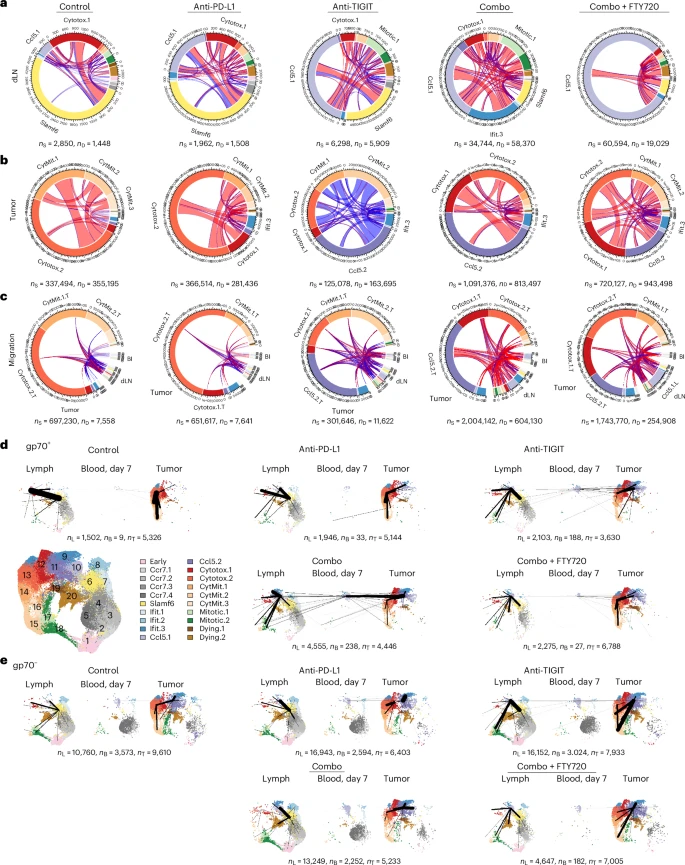
Relationship of CD8 T cell clusters within and between tissues in CT26 tumor-bearing mice after anti-TIGIT and/or anti-PD-L1 therapy.
Relationship Between CD8 T Cell Clusters and the Response to Tiragolumab Plus Atezolizumab Treatment
03
The composite gene signature score, consisting of the average expression levels of CCL5, CXCR3, and CXCR6, was significantly higher in CITYSCAPE patients than in non-responders. Compared with P+A, a high gene signature score in T+A treated patients was associated with favorable OS HR, while a low signature score showed no significant correlation with OS benefit. Classification of patients based on high or low gene signature scores revealed that OS was improved in T+A patients with high gene signature scores compared to those with low scores. In the Phase 3 OAK study of atezolizumab monotherapy in previously treated patients with locally advanced or metastatic NSCLC, the composite gene signature score was also associated with improvements in progression-free survival and OS.
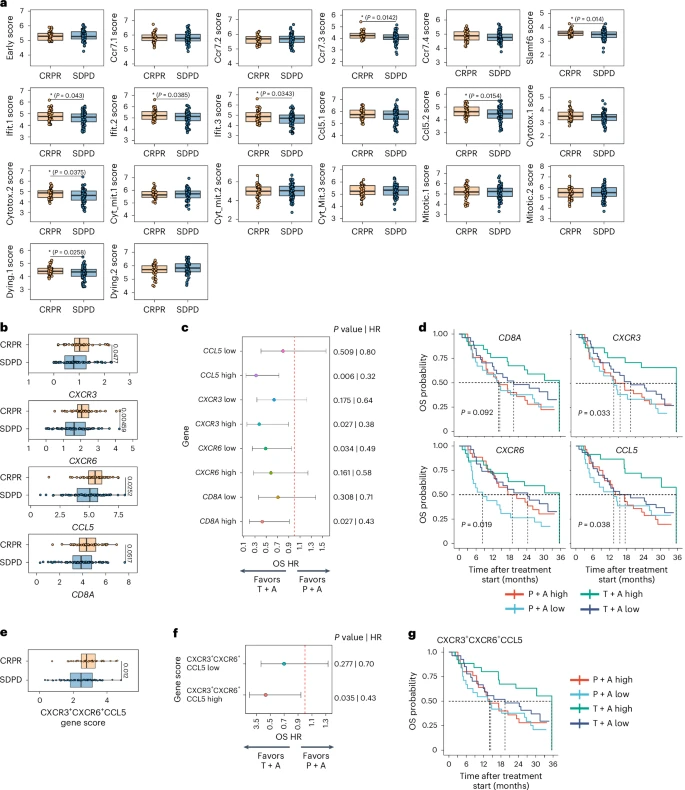
Human CD8 T Cell Clusters and Gene Signatures Associated with Clinical Responses to Tiragolumab and Atezolizumab.
Summary
04
1. The Role of PD-1 and TIGIT:PD-1 and TIGIT Guide T Cell Fate in Both dLNs and Tumors: T Cell Activation, Expansion, and Differentiation Begin in dLNs, While the Final Determination of Teff or Tex Cell Progression Occurs in the Tumor.
2. T Cell Population in the Blood:After combination therapy, the blood mainly exhibited a single population of CD8 T cells (Ccl5.1 cluster), which were expanded in the dLNs and also detected in the tumor.
3. Differences in the inhibitory effects of PD-1 and TIGIT:Both promote the differentiation of tumor-specific T cells from the Tscm compartment into the Ccl5.1 transitional cell population in dLNs, but anti-PD-L1 treatment also showed differentiation toward the Cytotox.1 phenotype, while anti-TIGIT and combination treatments demonstrated a second phase of broad differentiation from the Ccl5.1 phenotype into other phenotypes.
4. Tscm and Tpex Cells as Therapeutic Targets:Tscm or Tpex cells are considered targets for PD-1-PD-L1 targeted immunotherapy and may also be targets for PD-L1-TIGIT combination therapy.
5. The Effect of Combination Therapy on Progenitor Cell Populations:The combination therapy of anti-PD-L1 and anti-TIGIT acts on precursor cell populations, which may be defined by the Slamf6 cluster in dLNs and subsequently the Ccl5.1 and Ccl5.2 clusters in tumors.
6. Clinical Significance of Combination Therapy:The high-quality anti-tumor T cells generated by combination therapy can exert effector functions in a less suppressive environment, potentially offering greater clinical benefits for more patients compared to using anti-PD-(L)1 alone.
7. The Potential of Combination Therapy Strategies:Using combination treatment strategies such as anti-TIGIT and anti-PD-L1 to drive these two mechanisms may lead to more durable responses and better survival outcomes.
References:
1.Mellman, I., Chen, D. S., Powles, T. & Turley, S. J. The cancer-immunity cycle: indication, genotype, and immunotype. Immunity 56, 2188–2205 (2023).
2.Chiang, E. Y. & Mellman, I. TIGIT–CD226–PVR axis: advancing immune checkpoint blockade for cancer immunotherapy. J. Immunother. Cancer 10, e004711 (2022).