Sinocell Bio's TCR-T Therapy SCG142 Receives IND Approval in China, Demonstrating Over 70% Tumor Shrinkage and Complete Viral Clearance

SCG Cell Therapy
Innovative Immunotherapy Developer


On January 2, 2025, SCG SCIENCE (DALIAN) CO., LTD announced that the Center for Drug Evaluation of the National Medical Products Administration (NMPA) has approved the Investigational New Drug (IND) application for its next-generation TCR-T cell therapy, SCG142, primarily for the treatment of HPV infection-related malignant tumors.
Human Papillomavirus (HPV) is an extremely common sexually transmitted pathogen. HPV infection can cause over 90% of anal and cervical cancers, approximately 70% of vaginal and vulvar cancers, 60% of penile and oropharyngeal cancers. It is estimated that globally, there are 630,000 new cancer cases and 350,000 cancer-related deaths annually associated with HPV infection.
The advent of SCG142 will provide a new option for the treatment of such solid tumors. SCG142 is a fully natural HPV-specific TCR-T cell therapy product with high affinity. The research and development team successfully screened for a fully natural HPV-specific TCR and combined it with a novel chimeric switch receptor pluripotent T cell enhancement module independently developed by SCG SCIENCE (DALIAN) CO., LTD. This product can effectively overcome the harsh tumor microenvironment, converting inhibitory signals into co-stimulatory signals—a key feature that is crucial for achieving effective immunotherapy in solid tumors!

▲Screenshot source“NMPA”
The occurrence of certain cancers may be related to viral infections, such as human papillomavirus (HPV)-associated epithelial cancers (e.g., HPV-related cervical cancer) and hepatitis B virus (HBV)-associated hepatocellular carcinoma (HCC). These virus-related cancers are usually incurable at advanced stages and resistant to chemotherapy, making it urgent to seek new treatment methods. The emergence of TCR-T therapy, which possesses both anti-cancer and antiviral effects, brings new hope to such patients!
In addition to the SCG142 TCR-T cell therapy mentioned at the beginning, which has received IND approval from China's NMPA, SCG Science (Dalian) Co., Ltd. also has another TCR-T therapy under development—SCG101—that caused a huge sensation upon its debut!
Liver cancer is the sixth most common cancer globally, with more than 900,000 new cases annually. Hepatitis B virus (HBV) infection is the leading cause of liver cancer, and HBV-related hepatocellular carcinoma accounts for over 80% of liver cancer cases in China. After HBV infection, viral DNA integrates into the host genome, which can lead to genomic instability of the host cells, expression of virus-related oncogenes, and induction of inflammatory and oxidative stress responses, causing abnormal regeneration of hepatocytes. Ultimately, multiple mechanisms together contribute to the development of hepatocellular carcinoma.
SCG101 is a hepatitis B antigen-specific TCR-T cell therapy that can specifically target HBV antigen-related T-cell epitopes, effectively eliminating HBV-HCC tumor cells, HBV-DNA-integrated precancerous lesion cells, and HBV-infected cells. After infusion, it forms specific memory T-cell subsets, enabling SCG101 to achieve long-term self-renewal capability and functionality, sustaining continuous anti-tumor and antiviral effects. Clinical data show that SCG101 exhibits significant anti-tumor and antiviral activity. Its latest breakthrough clinical data was presented at the International Society for Cell & Gene Therapy (ISCT) conference held in Paris, France. A patient diagnosed with HBV-related hepatocellular carcinoma achieved partial response (PR) after receiving a single dose of SCG101, with a 74.5% reduction in tumor size and 100% clearance of hepatitis B infection.
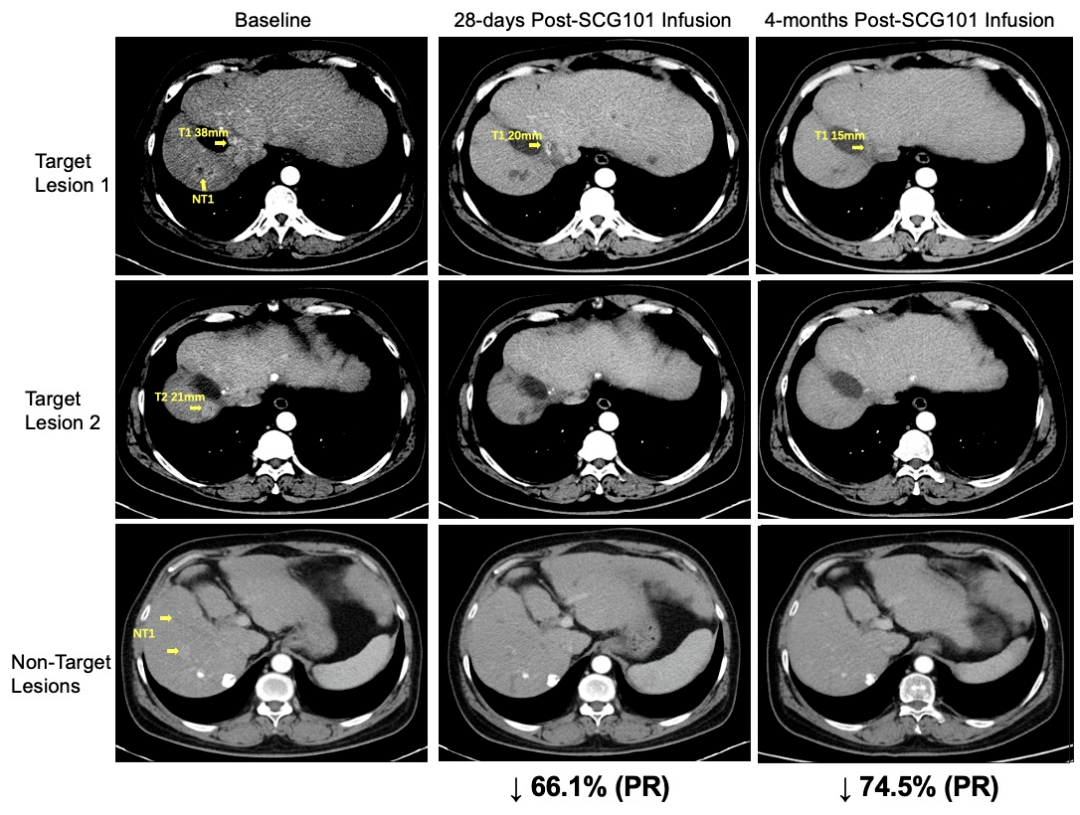
1、Significant Tumor Shrinkage: The patient received a single infusion of SCG101.Day 28,The tumor target lesion decreased by 66% compared to baseline, reaching partial response (PR)., and inTumor further reduced by 74.5% in the 4th month of treatment;Another lesion has completely disappeared.It is worth mentioning that the patient did not receive any other anti-tumor treatments during the trial period. As of the time of data collection,The patient's tumor has not progressed for more than 6.9 months, and the patient remains in a sustained state of remission.。
▼Radiological changes in the patient before and after the infusion of SCG101
▲Source of the Image“SCG"**, owned by the original author. If we unintentionally infringe on intellectual property rights, please contact us for removal."**
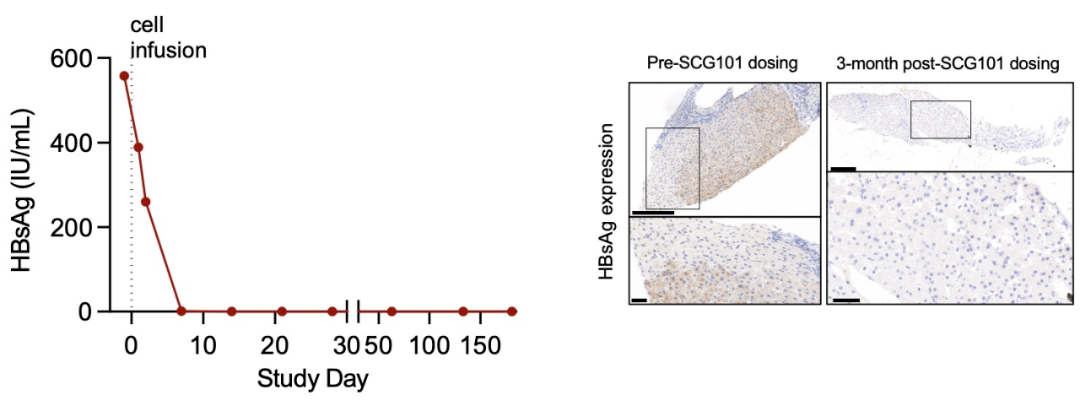
2、HBV Infection Remission: Immunohistochemical analysis of the liver before and after infusion showed,100% Clearance of Hepatitis B Surface Antigen-Positive Hepatocytes Achieved, HBV serological marker HBsAg before SCG101 infusion557.96 IU/mL, dropping to on Day 7 post-infusion1.3 IU/mL,On Day 28, it further decreased to0.08 IU/mL(See the figure below for details).
▼Changes in HBsAg Levels Before and After SCG101 Infusion in This Patient
▲Source of the Image“SCG"`, owned by the original author. If we unintentionally infringe on intellectual property, please contact us for removal."
The good news is that several TCR-T therapies under research are currently conducting related clinical trials for gynecological malignancies (cervical cancer, endometrial cancer, ovarian cancer), head and neck tumors, and hepatitis B virus-related hepatocellular carcinoma. Chinese patients also have the opportunity to benefit from this new powerful tool for solid tumors: TCR-T therapy!
Cancer patients who wish to participate can submit their treatment history, recent pathological examination, imaging and blood tests, discharge summary, and other relevant materials toGlobal Cancer Doctors Network Medical Department (400-666-7998), conduct a preliminary assessment or understand the detailed inclusion and exclusion criteria!

HPV-Related Epithelial Cancers Include Squamous Cell Carcinomas and Adenocarcinomas of the Cervix, Oropharynx, Anus, Vulva, Vagina, and Penis. These cancers express the E6 and E7 oncoproteins, which are viral antigens driving malignancy and are absent in healthy tissues, making them attractive targets for studying genetically engineered T-cell therapies (TCR-T) in epithelial cancers.
The National Cancer Institute of the United States launched a "First-in-Human Phase I/II Clinical Study of TCR-T Therapy for HPV-Related Epithelial Cancer (NCT02858310)", this study enrolled a total of 12 patients with metastatic HPV16-positive epithelial cancer, with a median age of 50 years (range 32-70 years), including6 cases of cervical cancer, 4 cases of anal cancer, 1 case of oropharyngeal cancer, 1 case of vaginal cancer(Three of the cervical cancer tumors were adenocarcinomas, and all other tumors were squamous cell carcinomas), and all patients had previously received platinum-based therapy before enrollment to receive E6 TCR-T cell treatment.
The results showed that: the tumors of most patients regressed, although the depth and duration of regression varied. Two patients in the highest dose group achieved objective tumor response (see figure below for details).
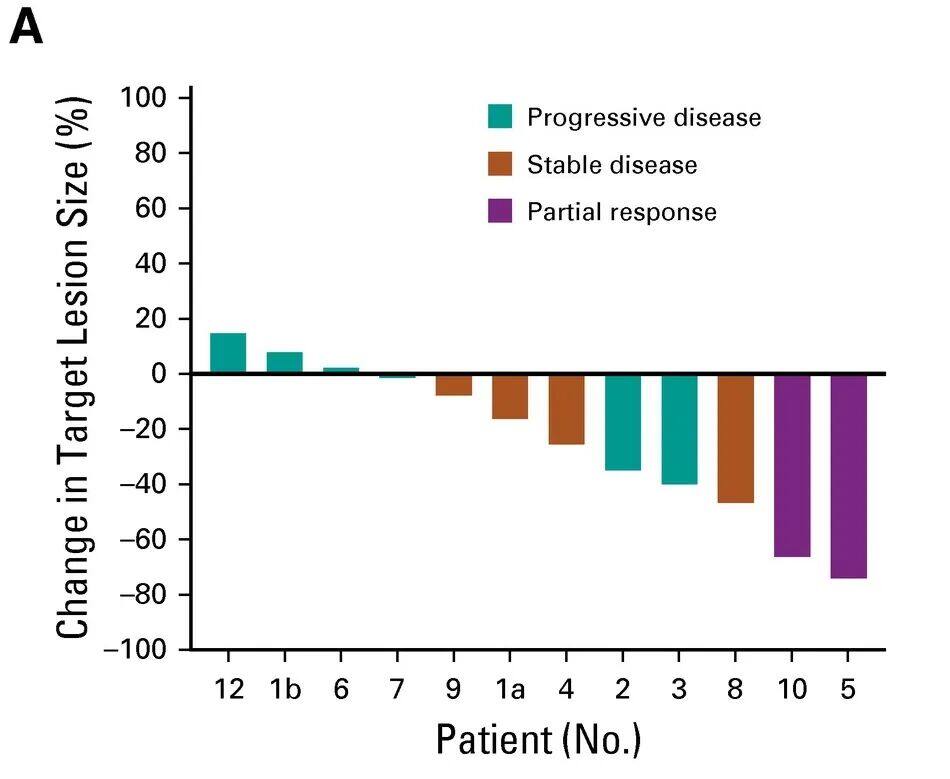
▲Source of the Image“JCO",Copyright belongs to the original author. If intellectual property rights are unintentionally infringed, please contact us for removal."
Notably, one 48-year-old female patient (Patient 5) with anal squamous cell carcinoma and three metastases, after receiving E6 TCR-T cell therapy,One tumor lesion completely regressed, and two tumors partially regressed.The patient had previously received treatments such as radiotherapy, fluorouracil + mitomycin, and cisplatin + capecitabine, but all showed unsatisfactory results, with disease progression observed in both lungs. The patient subsequently enrolled to receive E6 TCR-T cell therapy, and post-treatment results showed,Her condition miraculously achieved partial remission (PR),Specifically manifested asOne lung tumor completely regressed, and two lung tumors partially regressed., all were removed as they progressed. More surprisingly,Three years after TCR-T treatment, the patient still shows no signs of disease recurrence.(See the figure below for details).
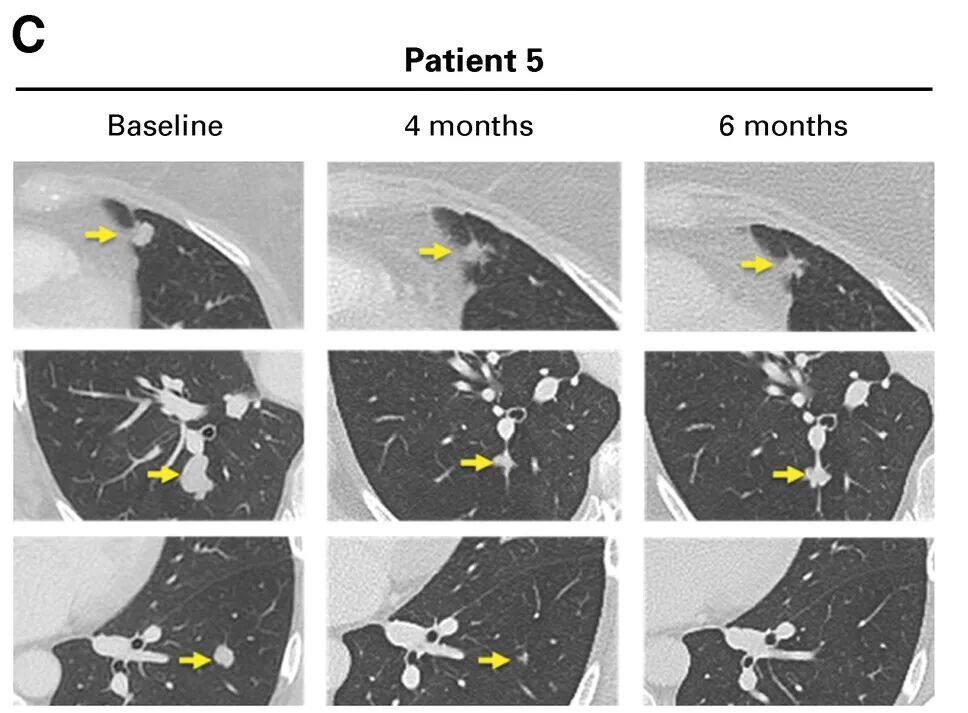
▲Source of the Image“JCO"`, owned by the original author. If we unintentionally infringe on intellectual property rights, please contact us for removal."
Note: Contrast-enhanced CT scan shows tumor response in Patient 5. Partial regression of two lesions (top and middle rows), complete regression of one lesion (bottom row).
TCR-T cell therapy, an immunotherapy based on genetic engineering, is a promising treatment method. It involves genetically modifying the patient's T cells to express specific TCRs, which can recognize tumor-associated antigens presented by major histocompatibility complex (MHC) on cancer cells. By utilizing the natural TCR-MHC interaction, it targets a broader range of intracellular antigens, including neoantigens derived from mutated proteins, offering significant advantages in treating solid tumors.
Compared with traditional cancer therapies, TCR-T cell therapy has the following significant advantages:
1. TCR-T cell therapy is highly specific as it targets patient-specific tumor antigens, thereby minimizing collateral damage to normal tissues.
2. TCR-T cell therapy can provide a lasting immune response, with the modified T cells able to survive and function effectively in the body for an extended period.
3. TCR-T cell therapy has the potential to overcome drug resistance in certain tumors that are unresponsive to conventional treatments, and it has demonstrated significant efficacy in treating hematologic malignancies and certain solid tumors.
In recent years, TCR-T cell therapy has gained widespread attention and achieved significant progress in the field of cancer treatment. The number of clinical trials has increased year by year from 2006 to 2024, peaking between 2019 and 2024. As of August 1, 2024, a total of 417 interventional clinical trials have been registered globally. North America conducted 84 trials (48.3%), Asia conducted 62 trials (35.6%), and Europe conducted 8 trials (4.6%) (see details in the figure below).
On August 2, 2024, the world witnessed the groundbreaking approval and market launch of the first-ever TCR-T therapy targeting solid tumors — afami-cel (TECELRA®), primarily for the treatment of adult patients with unresectable or metastatic synovial sarcoma.Read the original article for more details: The Most Expensive Immunotherapy in History is Born! Can the $5.2 Million TCR-T Therapy in the U.S. Really "Cure" Cancer?
▼Global Distribution of Clinical Trials for TCR-T Cell Therapy in Cancer Treatment
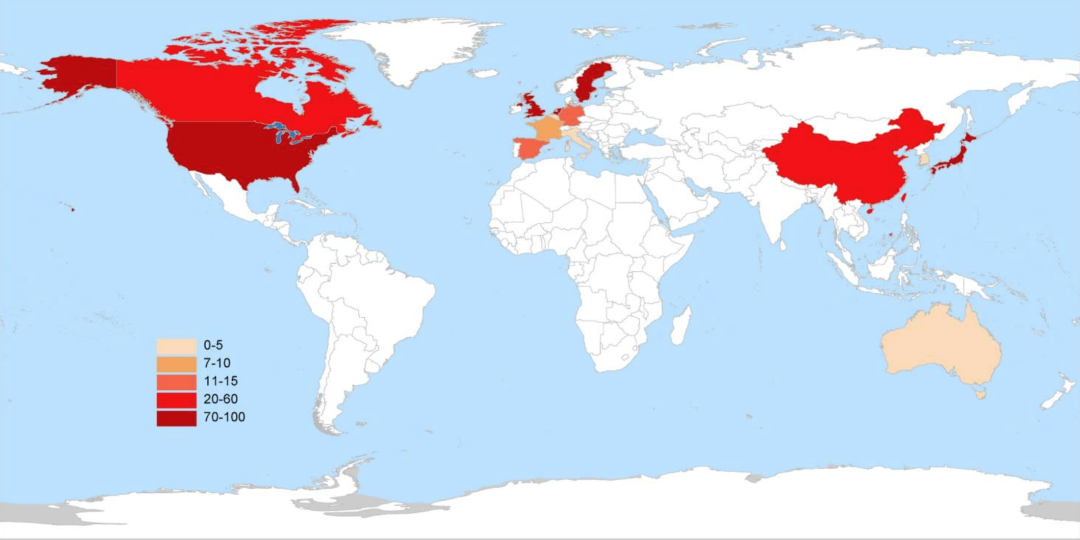
▲Source of the Image"Front Immunol", the copyright belongs to the original author. If we unintentionally infringe on intellectual property rights, please contact us for removal.
Currently, the TCR-T cell therapy under research mainly targets the 10 most commonly studied types of cancer, including:Soft Tissue Sarcoma (STS), Melanoma, Esophageal Cancer, Non-Small Cell Lung Cancer (NSCLC), Liver Cancer, Colorectal Cancer, Ovarian Cancer, Gastric Cancer, Acute Lymphoblastic Leukemia (ALL), Non-Hodgkin's Lymphoma (NHL)。

The main targets of currently researched TCR-T cell therapies are as follows:
1、NY-ESO-1: Namely, Cancer-Testis Antigen 1B (CTAG1B), is a primary target for soft tissue sarcoma and shows significant correlation with non-small cell lung cancer, esophageal cancer, melanoma, liver cancer, and ovarian cancer, among others.
2、MAGE:MAGE family members, especially MAGE-A4, exhibit high targeting potential in soft tissue sarcoma and esophageal cancer.
3、IL2RA (i.e., Interleukin-2 Receptor α Chain): Mainly targets melanoma, with moderate targeting in other cancers.
4、CD19: Mainly targeting Acute Lymphoblastic Leukemia (ALL) and Non-Hodgkin's Lymphoma (NHL).
5、KRAS: Mainly targeting colorectal cancer.
6、Other Targets: Including TNF receptor superfamily member 17 (TNFRSF17), CD22, CD38, CD33, C-type lectin domain containing 14A (CLEC14A), etc., which exhibit consistent but lower targeting potential in various cancers (see figure below).
▼Disease and Target Distribution in TCR-T Cell Cancer Clinical Trials
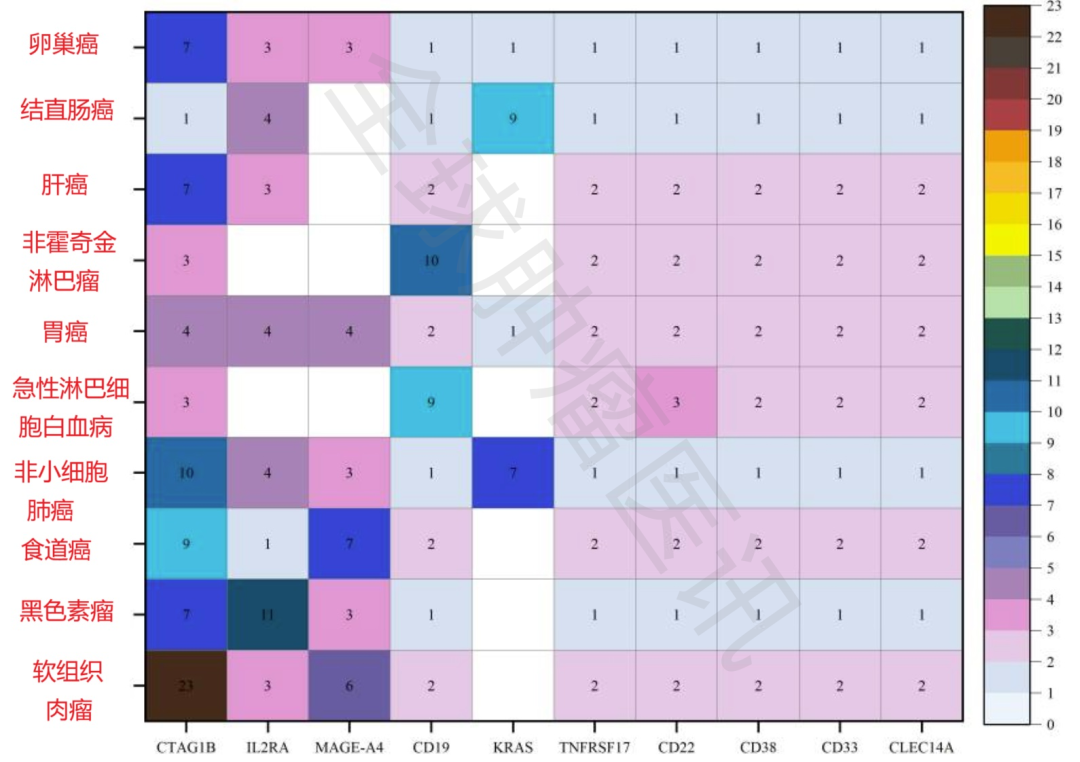
▲Source of the Image"Front Immunol", the copyright belongs to the original author. If we unintentionally infringe on intellectual property rights, please contact us for removal.
For patients with advanced melanoma who are resistant to immune checkpoint blockade (ICB) or BRAF-targeted therapy, new treatment methods are necessary. The emergence of BNT221 brings new hope to such patients! BNT221 is a personalized neoantigen-specific autologous T-cell product derived from peripheral blood. The globally renowned journal *Nature Medicine* recently reported impressive data from a Phase 1 clinical study (NCT04625205) on "the use of BNT221 TCR-T therapy for treating unresectable or metastatic melanoma resistant to ICB"!
A total of 9 patients with unresectable or metastatic melanoma who were resistant to ICB were enrolled in this study to receive BNT221 treatment. Among them, 3 patients received BNT221 at dose level (DL) 1, and 6 patients received DL2 treatment.
The results showed that: among the 9 patients who received treatment,The best overall response for 6 patients was stable disease (SD).Among them, 4 patients with stable conditions (NAC03, NAC07, NAC08, and NAC09) experiencedTumor Regression, evaluated according to the Response Evaluation Criteria in Solid Tumors (RECIST) 1.1,Up to -20% reductionTwo patients (NAC08 and NAC09) reported自觉Tumor-related symptoms improved., includingImproved range of motion, reduced edema in the affected limb, enhanced basic activities of daily living。
▼Clinical Response Waterfall Plot Based on RECIST 1.1
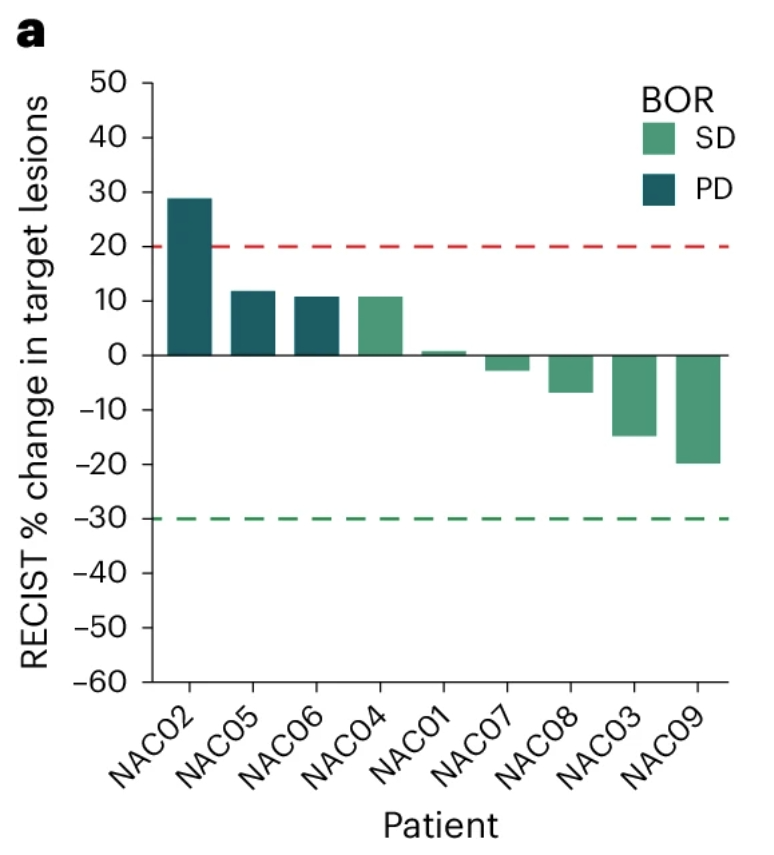
▲Source of the Image“SCG"**, owned by the original author. If we unintentionally infringe on intellectual property rights, please contact us for removal."**
It is worth mentioning that,Patient NAC09 showed the largest reduction in tumor size., six weeks after the infusion of BNT221 TCR-T cells, a computed tomography (CT) scan showed thatThe target lesion in the left axilla decreased by 20%.,Significant reduction in non-target lesions (including secondary axillary lymph nodes and millimeter-sized pulmonary lesions)(see the figure below). In addition, immunohistochemical analysis showed increased T-cell infiltration in the patient's tumor.
▼CT Scan Comparison of Patient NAC09 Before and After TCR-T Treatment
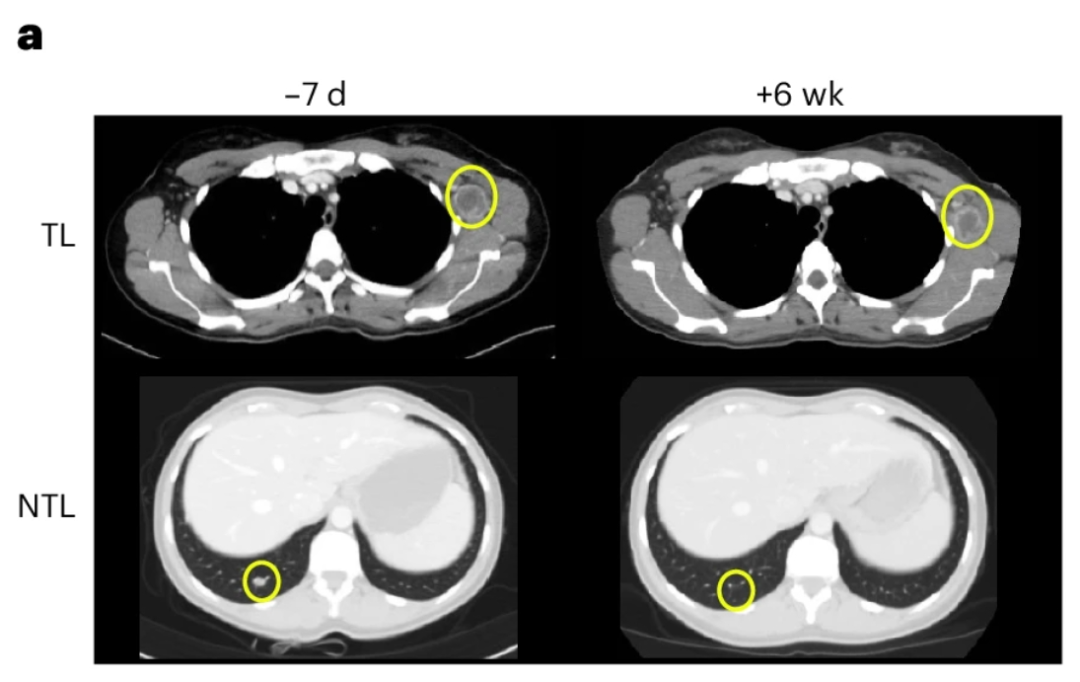
▲Source of the Image“SCG"`, owned by the original author. If we unintentionally infringe on intellectual property rights, please contact us for removal."
Note:
① The circular area highlights the target lesion (top) and non-target lesion (bottom), with regression observed between Day -7 and Week +6.
②NTL - Represents Non-Target Lesions; TL - Represents Target Lesions.
Non-Small Cell Lung Cancer (NSCLC) accounts for more than 80% of all lung cancer cases. NSCLC can be further divided into three major histological subtypes: Lung Adenocarcinoma (LADC), Lung Squamous Cell Carcinoma (LSCC), and Large Cell Lung Cancer (LCLC), with LADC being the most common subtype. For patients with advanced NSCLC (Stage IIIb and IV), surgical treatment options are often unavailable, and systemic treatments such as radiotherapy, chemotherapy, targeted therapy, and immunotherapy are primarily used. However, the incidence of severe side effects from chemotherapy and radiotherapy is high; targeted therapy may encounter resistance; additionally, some lung cancer patients do not respond to checkpoint immunotherapy. Therefore, there is an urgent need for new immunotherapy strategies for patients who do not respond to immune checkpoint therapies. Recent studies have found that NY-ESO-1 is a promising target for cancer immunotherapy, demonstrating good safety and efficacy, and is expressed in 11.8%~21% of non-small cell lung cancers.
Recently, the well-known journal "Oncology Letters" reported a "Application of NYESO1-Specific TCR-T Cell Therapy Leads to Significant Tumor Reduction to Partial Remission in Advanced Non-Small Cell Lung Cancer"A classic case!" This study enrolled four patients with HLA-A2 positive NY-ESO-1 metastatic non-small cell lung cancer (NSCLC), who received lymphodepleting chemotherapy, followed by adoptive transfer of NY-ESO-1 TCR-T cells + systemic IL-2 treatment.
The results showed that two patients who received three (Patient 1) and two (Patient 2) infusions of NY-ESO-1 TCR-T cell therapy achieved clinical responses. According to the Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 criteria,Patient 1 had stable disease (SD) nearly 3 months after adoptive transfer of NY-ESO-1 TCR-T cells.(Table I).Patient 2 achieved partial response (PR) at 4 months post-treatment.(NCT02457650)。
Notably, one of the patients was a 44-year-old HLA-A2 positive female with advanced lung adenocarcinoma (LADC) who was NY-ESO-1 positive (Patient 2). This patient also carried an EGFR mutation and had previously undergone six cycles of combination chemotherapy (docetaxel and carboplatin), but with unsatisfactory results, as her disease continued to progress. She subsequently received treatments with gefitinib and erlotinib, but these were also ineffective. A follow-up CT scan in September 2015 showed progressive disease (PD) in the right hilar region, mediastinum, right pleura, right hepatic lobe, and liver capsule, leaving no further clinical treatment options available at that time. However, there was still hope. A bronchoscopic biopsy of the right lung tumor revealed strong NY-ESO-1 positivity by immunohistochemical staining, leading to her enrollment in NY-ESO-1 TCR-T cell therapy.
Surprisingly,CT scan on Day 43 after the first TCR-T cell infusion showed, the patientRegression of primary lung lesion and liver metastasis, pleural effusion absorbed, lung re-expanded(See the figure below for details),The primary lung lesion decreased from 95×86×54 mm to 64×44×54 mm.,The liver metastasis lesion shrank from 19.8×19.6×20 mm to 10×10×10 mm., according to RECIST 1.1 for efficacy evaluation,The patient miraculously achieved partial remission (PR).。
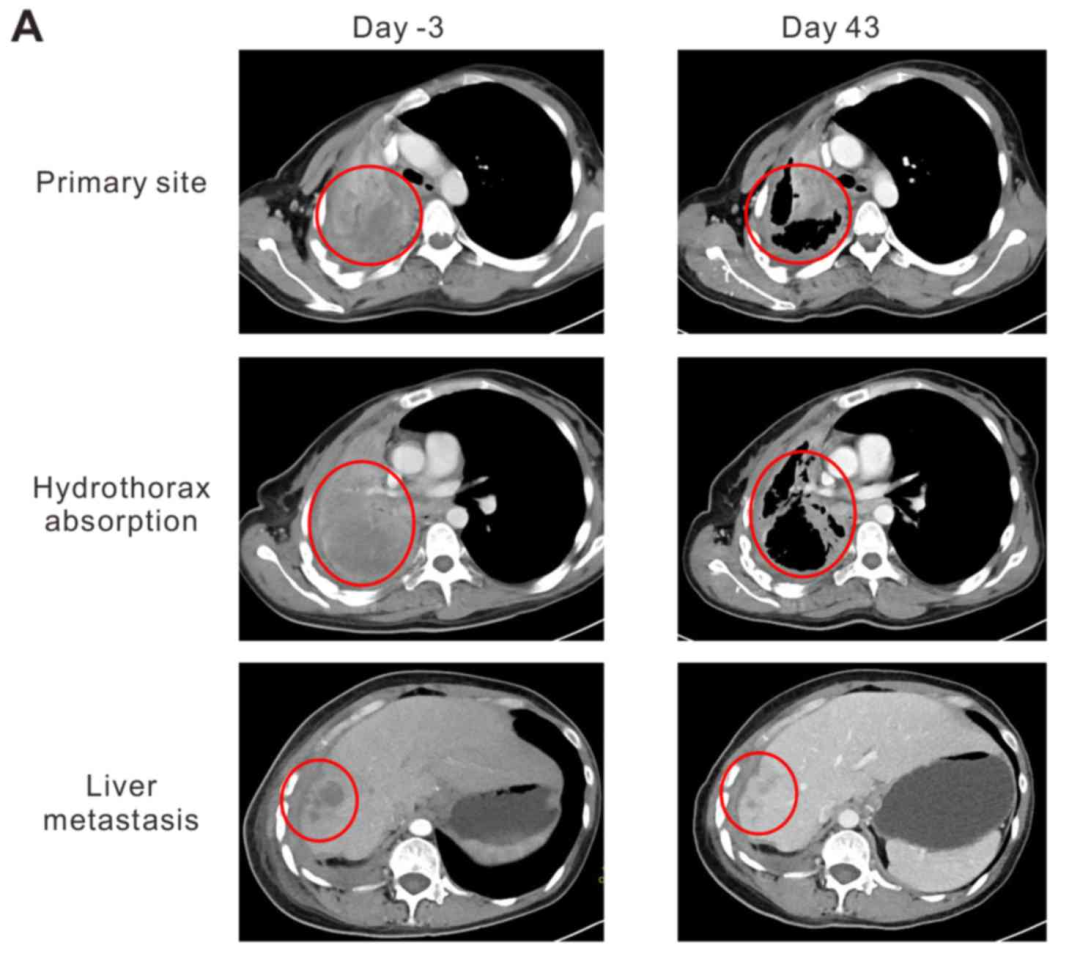
▲Source of the Image“Oncology "Letters", the copyright belongs to the original author. If we unintentionally infringe on intellectual property rights, please contact us for removal.
Note:
①CT scan showed: The primary tumor was located in the right hilar region and had metastasized to the mediastinum, right pleura, right lobe of the liver, and hepatic capsule prior to T-cell infusion.
② In January 2016 (Day 43), a CT scan performed two months after the first T-cell infusion showed: objective regression of the primary lung tumor and liver metastases, as well as pleural effusion absorption and lung re-expansion.
Moreover,Tumor markers (CEA, CA125, CA199) decreased after the initial infusion of TCR-T cells., which increased subsequently (4 weeks after the first infusion of TCR-T cells), and a similar change was observed after the second infusion of NY-ESO-1 TCR-T cells (see the figure below for details).
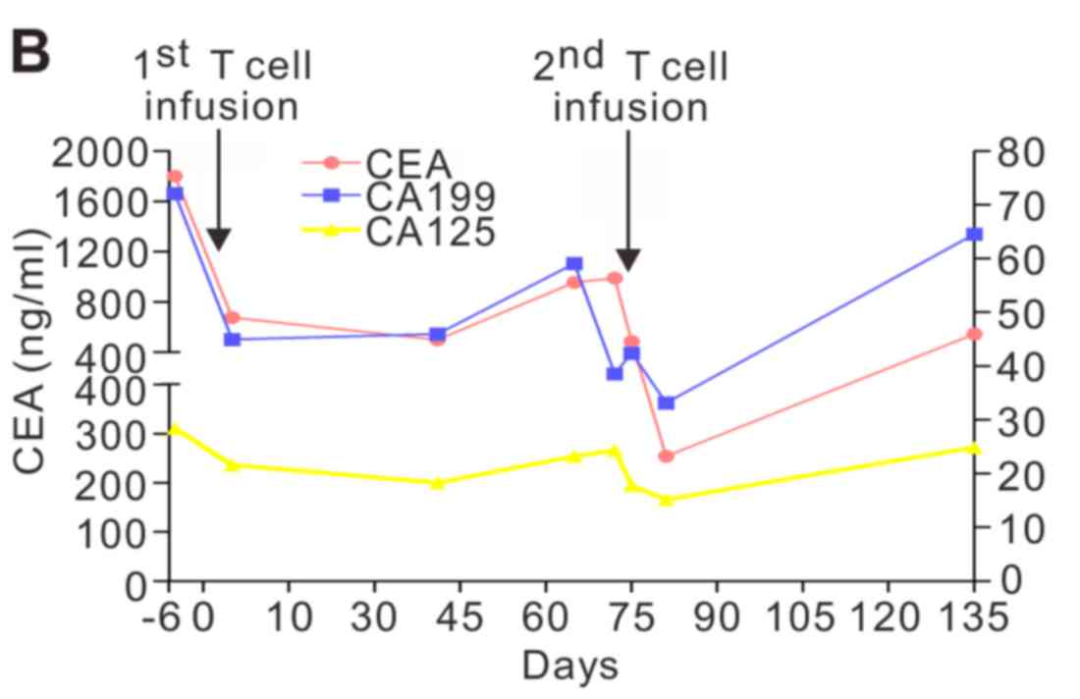
▲Source of the Image“Oncology "Letters", the copyright belongs to the original author. If we unintentionally infringe on intellectual property rights, please contact us for removal.
NotableIt is, the patient'sThe Karnofsky Performance Status (KPS) improved after infusion, increasing from 50 to 90, with symptoms of hemoptysis and chest pain being alleviated., these results all indicate that TCR-T cell therapy improved the clinical symptoms of patients.
TCR-T Therapy and CAR-T Both Belong to T Cell Therapy, but TCR-T Therapy Has a Wider Range of Target Antigens and Is Considered More Promising in Fighting Solid Tumors. More Remarkably, TCR-T Therapy Pioneers a "Two Birds with One Stone" Novel Treatment Approach, Demonstrating Effectiveness, Safety, and Feasibility in Simultaneously Targeting Cancer and Viral Infections. Therefore, In Recent Years, Researchers Have Attempted to Apply TCR-T Therapy to Treat Cervical Cancer [Mainly Related to Human Papillomavirus (HPV) Infection], Hepatitis B Virus-Related Hepatocellular Carcinoma, and Other Types of Cancer, Showing Impressive Results.
Patients seeking help from TCR-T, CAR-T, TILs therapies or other new anti-cancer technologies at home and abroad can submit their treatment history, recent pathology reports, and imaging examination results toGlobal Cancer Doctors Network Medical Department (400-666-7998), conduct a preliminary assessment or apply for domestic and international oncology consultations to seek personalized treatment options that suit their own conditions.
[1]Borgers J S W,et al.Personalized, autologous neoantigen-specific T cell therapy in metastatic melanoma: a phase 1 trial[J]. Nature Medicine, 2025: 1-13.
https://www.nature.com/articles/s41591-024-03418-4
[2]Li J,et al.Clinical advances and challenges associated with TCR-T cell therapy for cancer treatment. Front Immunol. 2024 Oct 8;15:1487782.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11493697/
[3]Xia Y,et al.Treatment of metastatic nonsmall cell lung cancer with NYESO1 specific TCR engineeredT cells in a phase I clinical trial: A case report[J]. Oncology letters, 2018, 16(6): 6998-7007.
https://www.spandidos-publications.com/10.3892/ol.2018.9534
[4]Doran S L,et al.T-cell receptor gene therapy for human papillomavirus–associated epithelial cancers: a first-in-human, phase I/II study[J]. Journal of Clinical Oncology, 2019, 37(30): 2759-2768.
https://ascopubs.org/doi/10.1200/JCO.18.02424
[5]https://www.cde.org.cn/main/xxgk/listpage/4b5255eb0a84820cef4ca3e8b6bbe20c
[6]https://www.scgcell.com/newsinfo/6283011.html
This article is original content from Global Oncology Doctors Network. Reproduction is strictly prohibited without authorization.
Scan to Add Patient Group
Cancer News|New Technologies|Drug Development|Leading Experts
Join the group to receive free anti-cancer resources