
Nanobody BCMA CAR-T
BCMA CAR-T Cell Therapy Shows Significant Efficacy in Multiple Myeloma (MM). The classical CAR consists of four parts: an extracellular antigen recognition domain, a transmembrane domain, an intracellular co-stimulatory domain (such as 4-1BB and/or CD28), and a CD3ζ signaling domain. CAR-T cells typically use the single-chain variable fragment (scFv) of a monoclonal antibody (mAb) as their antigen recognition domain. Nanobodies, which can serve as the variable domain of heavy-chain antibodies (VHH), have smaller size, higher stability, and a single-domain structure compared to traditional single-chain variable fragments. They also exhibit higher affinity and specificity. Notably, nanobodies show lower immunogenicity compared to murine monoclonal antibodies, potentially making them safer for use in CAR-T cell therapy.
S103 CAR-T cells are a Class I new drug with full independent intellectual property rights independently developed by Senlangbio. It is an innovative CAR-T product based on Senlangbio’s nanobody CAR screening and validation platform. Hebei Yanda Lu Daopei Hospital and Beijing Lu Daopei Hospital conducted research exploring the efficacy and safety of S103 CAR-T in treating multiple myeloma, which was recently published in *Blood Advances*.
Research Methods & Results
CAR-T Structure: The S103 CAR-T cell therapy construct used in the study contains two nanobodies (dVHH) targeting BCMA.

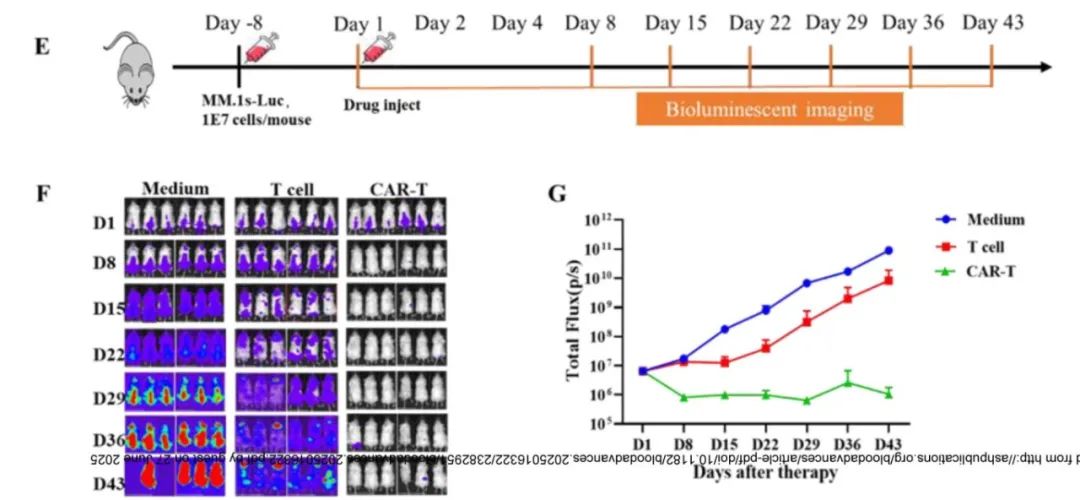
Preclinical Study: In vitro cytotoxicity assays were performed using the NCI-H929-Luc cell line, and in vivo anti-tumor efficacy was tested in the NPG mouse model. At effector-to-target (E:T) ratios of 1:1, 3:1, and 10:1, the lysis rates of S103 CAR-T cells against NCI-H929-Luc cells were 55.5%±18.5%, 86.6%±12.3%, and 97.1%±2.7%, respectively, significantly higher than those of the control group. In the NPG mouse model, complete tumor clearance was achieved by Day 8 post-infusion in the S103 CAR-T cell group, with no tumor recurrence observed during the study period.
Clinical Study Design:Patients undergo autologous peripheral blood lymphocyte collection, followed by lymphodepleting chemotherapy, and then receive S103 CAR-T cell infusion. Efficacy evaluation includes immunoglobulin electrophoresis, free light chain analysis, bone marrow aspiration and biopsy (including detection of minimal/measurable residual disease [MRD] by flow cytometry), as well as whole-body PET-CT or localized CT imaging.
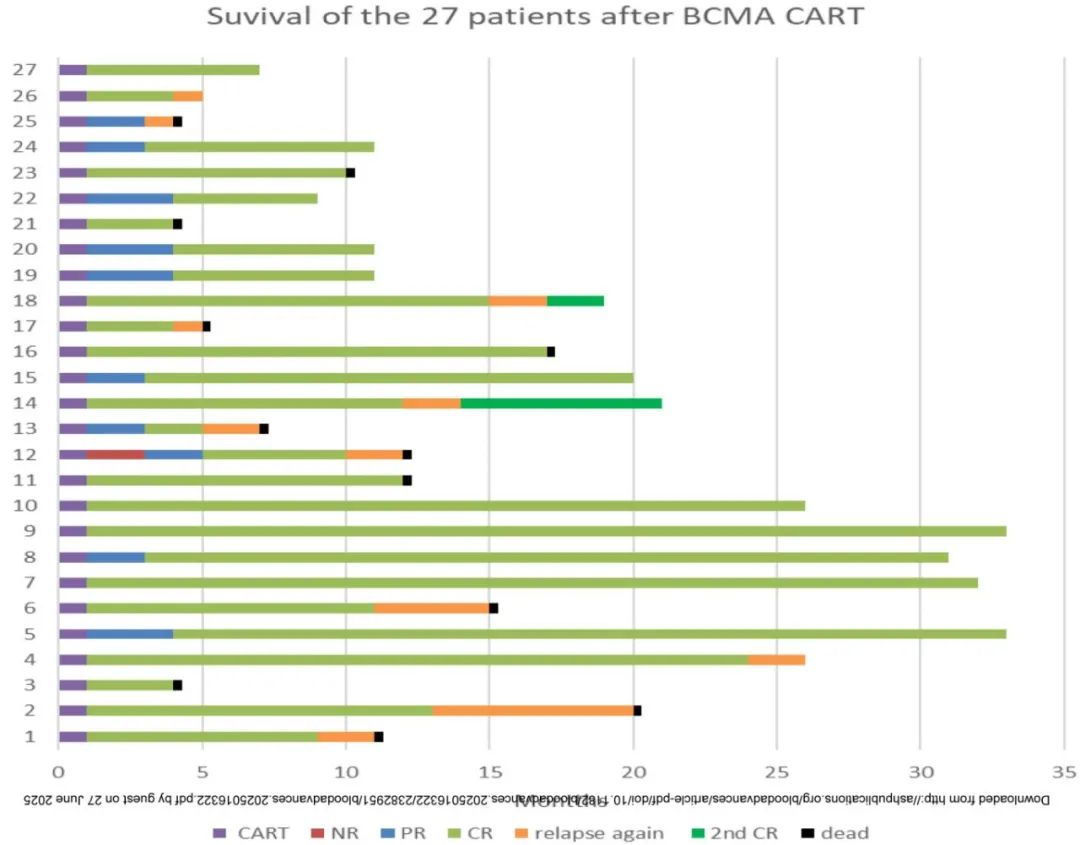
Patient Characteristics: A total of 27 patients were enrolled, including 4 cases of plasma cell leukemia and 1 case of undifferentiated plasma cell myeloma. The median age was 58 years, the median time from initial MM diagnosis to recurrence was 34 months, and the median number of prior treatment lines was 5. Eleven patients had extramedullary disease (EMD). Eleven patients exhibited high-risk genetic abnormalities, including 4 cases of TP53 mutations. The median BCMA expression rate was 53.3%.
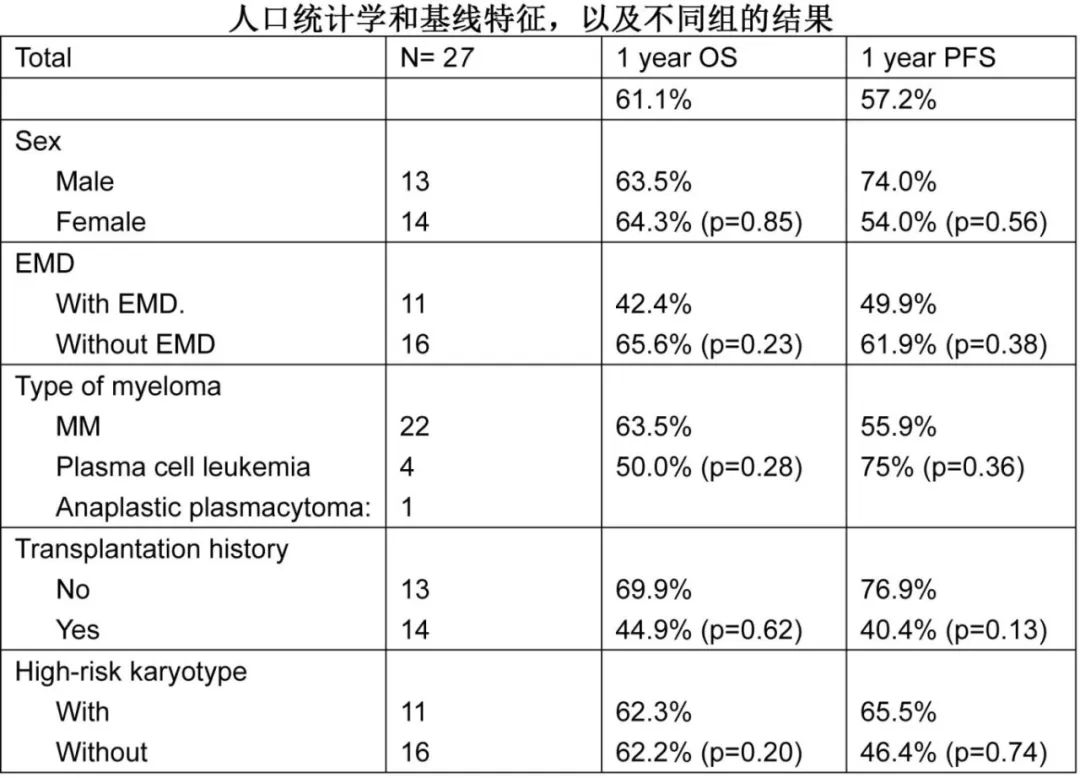
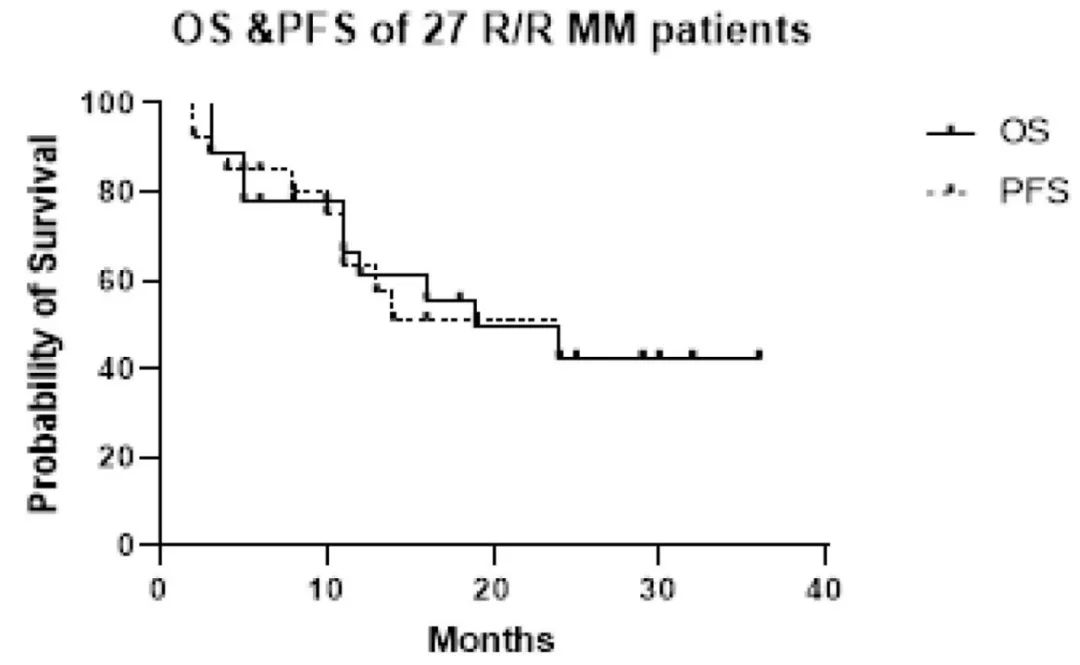
Efficacy Evaluation: One month later, the overall response rate (ORR) was 96.3% (26/27), with a complete response (CR) and very good partial response (VGPR) rate of 59.2% (16/27). At three months, the ORR reached 100% (27/27), and the CR+VGPR rate was 81.5% (22/27). The median duration of response was 11 months (2-36 months). The 1-year overall survival (OS) rate was 61.1%, and the progression-free survival (PFS) rate was 57.2%. The 2-year OS and PFS rates were 42.3% and 42.4%, respectively. Eleven patients died, seven due to disease progression and four from infections.
Efficacy in High-Risk Patients: Among 11 patients with high-risk cytogenetic abnormalities and/or TP53 mutations, 72.7% achieved CR within 3 months after BCMA-CAR-T cell infusion, with a 1-year OS of 62.3% and a 1-year PFS of 65.5%.
Plasma Cell Leukemia Subgroup: Among the 4 patients, all reached ORR within one month, 3 reached CR+VGPR, and 1 experienced disease progression (PD) within three months.
Extramedullary Disease (EMD) Subgroup: Among 11 patients, the ORR at one month was 100%. At three months, 9 patients still had a response, including 5 with CR+VGPR. The 1-year OS and PFS were 42.4% and 49.9%, respectively.
Central Nervous System (CNS) Infiltration Subgroup: All 3 patients initially presented with paralysis, achieving PR at one month; at three months, 2 cases reached CR.
Patients with no BCMA expression: Two patients with undetectable BCMA expression by flow cytometry also achieved CR through S103 CAR-T therapy and maintained long-term disease-free survival.
Safety:Four patients experienced grade 2 cytokine release syndrome (CRS), and one patient experienced grade 3 CRS. One patient developed grade 1 neurotoxicity. Of the 27 patients, 26 developed fever within three months after BCMA CAR-T cell infusion. Other common adverse events included vomiting, abdominal pain, and fatigue. Infections were significant complications following CAR-T treatment, including four cases of viral infections, seven bacterial infections, and five fungal infections. Four patients died due to infection-related complications.
Summary
BCMA CAR-T Therapy (S103 CAR-T) Utilizing Dual Nanobody VHH Targeting BCMA Demonstrates High ORR and Manageable Safety Profile in Treating Patients with Relapsed or Refractory Plasma Cell Myeloma, Including High-Risk Populations (High-Risk Cytogenetic Abnormalities, EMD, Plasma Cell Leukemia, and Undifferentiated Plasma Cells). These Findings Highlight the Potential of S103 CAR-T Therapy in Improving Clinical Outcomes Across Different Clinical Scenarios.
References
Xian Zhang, Lin Wang, Junfang Yang, Xiaona Hu, Hui Wang, Lina Zhang, Xiaoge Zhou, Ying Liu, Qinglong Wang, Peihua Lu; Efficacy and Safety of BCMA Nanobody CAR-T Cell Therapy in Relapsed or Refractory Plasma Cell Myeloma. Blood Adv 2025; bloodadvances.2025016322. doi: https://doi.org/10.1182/bloodadvances.2025016322
