Arbutus Biopharma Announces Phase 3 Clinical Data Publication for ABO1020, an mRNA Vaccine Targeting SARS-CoV-2 Omicron BA.4/5 Variants

Abogen
Nucleic Acid Drug Developer
2024Year7Month17Day,Cell PressMedical Flagship JournalMedPublished Abogen's COVID-19 Variant (BA.4/5)mRNAVaccine (Code Name:ABO1020`) Phase III efficacy clinical data. According to the information previously released by Abogen through its official WeChat account and various public channels,`ABO1020Based on its proprietary patentedmRNA-LNPIterative development of technology platforms can be conducted in2-8℃Stable storage and transportation with no international patent risks.
As the COVID-19 pandemic recedes, market demand for COVID-19 vaccines continues to decline. Having risen to prominence during the pandemic by accumulating numerous advantages,mRNATechnology is still highly anticipated for its unique advantages, becoming a key direction for future innovative vaccine development. Following the termination of cooperation with Walvax Biotechnology,, the first internationally published multi-center Phase III efficacy clinical study independently completed by the Abogen team. What are the research results and analytical insights? Here, we provide an interpretation and brief commentary on the main and noteworthy outcomes of this study, along with related discussions.
ABO1020Phase III Clinical AdoptionRandomized, Double-blind, Placebo-controlled Design, Evaluation of previous vaccinations2Agent or3Inactivated COVID-19 Vaccine Population ReceivedEfficacy, Immunogenicity, and Safety of Two Doses of ABO1020 Vaccine.The primary endpoint of the study was symptomatic PCR-positive cases occurring from 14 days after the second dose.. All endpoint cases were evaluated and confirmed by the Endpoint Assessment Committee (EAC).
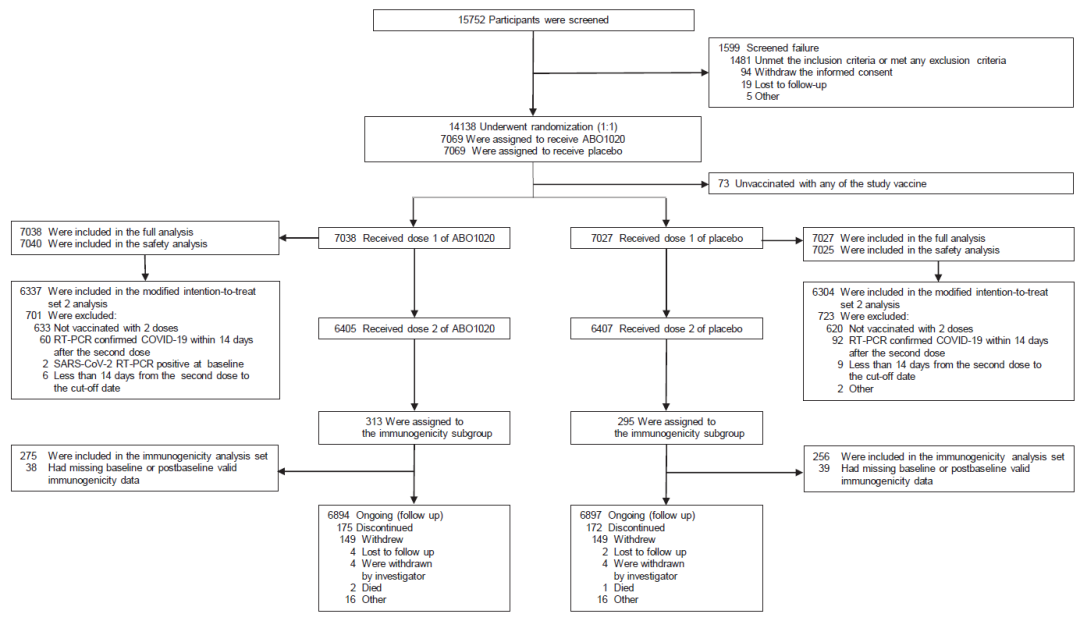
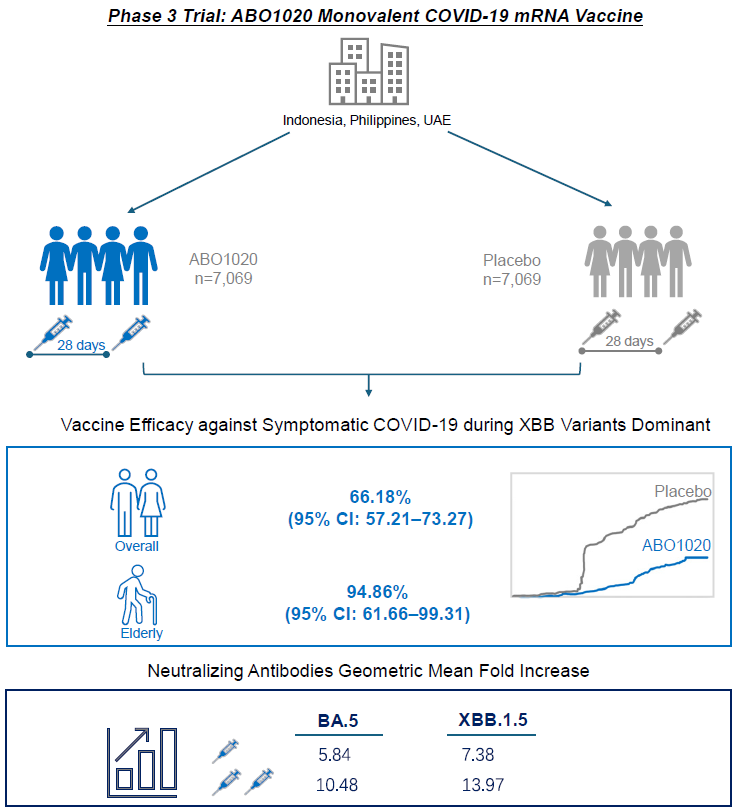
The Phase III clinical trial inOverseas3Countries (United Arab Emirates, Philippines, Indonesia)16Conducted at a research center in China, recruiting14138Subjects aged 18 years and above,Research from2022Year12Month Start to2023Year4Monthly Main Analysis, Time Spent4More than a month to complete enrollment and vaccination366Case EndpointCollect.
Protection Rate
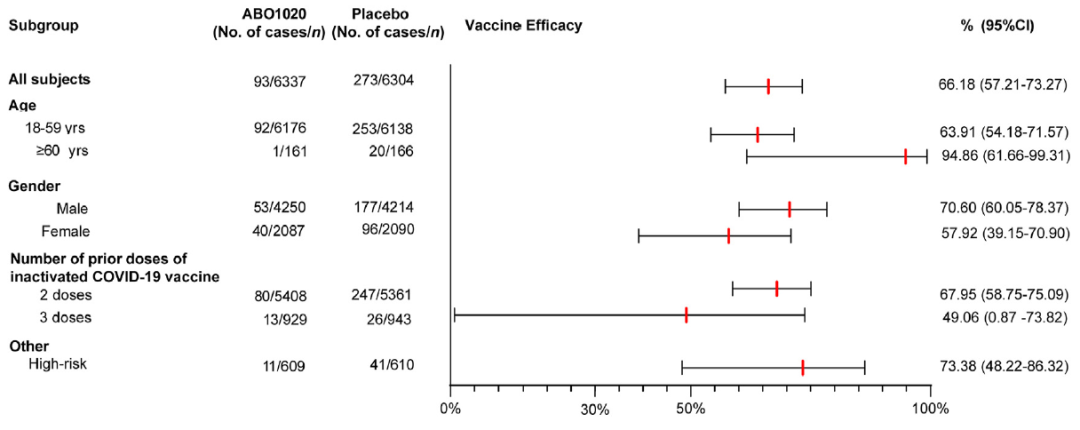
1) The primary endpoint protection rate was 66.18%.(95% CI: 57.21–73.27, p<0.0001). This result meets the WHO evaluation criteria for COVID-19 vaccine efficacy (protection rate ≥50%, lower limit of 95% CI ≥30%). The article also disclosed the number of main endpoint cases sequenced as XBB and its sub-lineages, accounting for 93% of typeable COVID-19 cases, consistent with the dominant circulating strains reported by the GISAID.org Coronavirus Data Platform as XBB and its sub-lineages in the country/region of the study during December 2022 to April 2023.
2) In the subgroup analysis,The protection rate of ABO1020 in the elderly population aged ≥60 is 94.86%.(95% CI: 61.66-99.31). Given the smaller sample size of elderly individuals in the study (349 cases), the trend of higher protection rates observed in the elderly population based on current data needs further validation in a larger sample population.
It is worth noting that,In the study, there were 1,219 cases of high-risk individuals, including elderly people ≥60 years old and those with underlying diseases. The protective rate in this population was 73.38%.(95% CI: 48.22-86.32), which suggests to some extent the protective effect of ABO1020 for high-risk populations.
3) Another interesting subgroup analysis showed,ABO1020In previous vaccinations3The protection rate of the inactivated COVID-19 vaccine in the population is lower than previous vaccinations.2The population receiving the inactivated COVID-19 vaccine. The article analyzes and discusses the possible reasons for this difference, suggesting that it may be related to...Related to the immune imprinting brought about by previous inoculations with more doses of the prototype strain inactivated COVID-19 vaccine,Similar differences have been reported in Professor Cao Yunlong's previously published research results. In addition, previous vaccination3Sample size of the population receiving the inactivated COVID-19 vaccine (2,162Example) Relative to previous vaccinations2Agent (11,903Example) Fewer cases may also be due to the lower protection rate in this subgroup population.95%CIOne of the broader influencing factors.
Immunogenicity
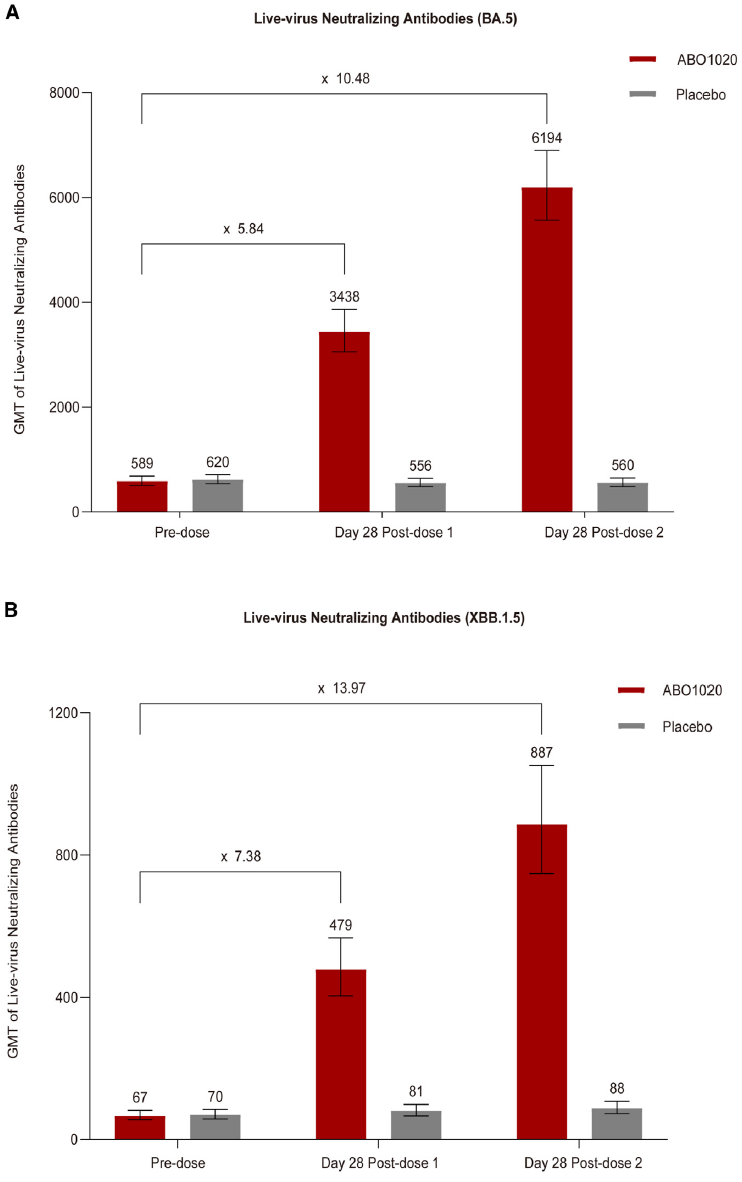
ABO1020 adopts a two-dose vaccination regimen, which undoubtedly increases the process and time required to complete immunization compared to administering a single sequential booster dose in the primary immunized population. The article discusses the necessity and rationale of the two-dose regimen based on actual neutralizing antibody evaluation results and reported studies on immune mechanisms.
1) After one dose of ABO1020, the GMT increase in neutralizing antibodies against Omicron BA.5 and XBB.1.5 live virus were respectively5.84And7.38; After the second dose, the neutralizing antibody GMT increased further, reaching levels10.48Times and13.97Times. Although the antigen sequence of BA.4/5 was no longer the predominant circulating strain (XBB and its sublineages) during the study period, the neutralizing antibody results demonstrated strong immunogenicity and cross-neutralization ability after two doses of ABO1020.
2) This result corroborates a recent study on the immune imprinting mechanism, which showed that repeated vaccination with variant-specific vaccines can break the immune imprinting effect established by prior infection with or vaccination against the prototype strain. This clarifies the situation for individuals who have not previously received a COVID-19 vaccine containing the Omicron strain or have not been infected with the Omicron strain.A two-dose booster vaccination is the recommended strategy to address new mutant strains.
3) In addition, the population in China has mainly received inactivated COVID-19 vaccines in the past, and currently, there are fewer people vaccinated with mRNA vaccines. For the mRNA vaccine-naïve population,It may be a more reasonable strategy to receive the first two doses of mRNA vaccine.`, similar to Moderna SPIKEVAX and Pfizer COMIRNATY, also adopted a two-dose vaccination strategy for primary immunization.`
Safety
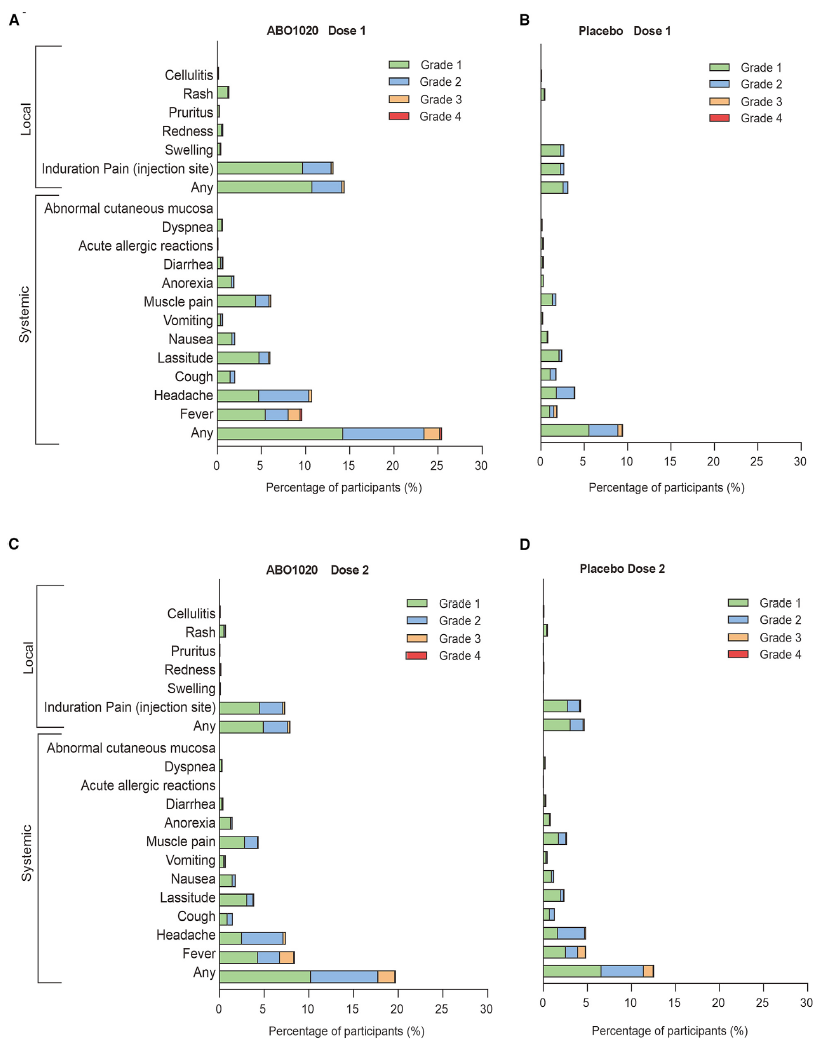
Safety has always been the primary concern for mRNA vaccines. According to the safety data presented in the article, most adverse reactions were grade 1/2, such as transient fever, injection site pain, and headache. The article also discussed the safety data across different doses and age groups:
1)The incidence of adverse reactions after the second dose was lower than that after the first dose.This phenomenon is different from the higher incidence of adverse reactions after the second dose of Pfizer's COMIRNATY vaccine compared to the first dose, and may be related to the inherent immunological properties of the vaccine or the tolerance of the study population.
2)The overall adverse reactions in the elderly are lower than those in young adults., despite the limited sample size, the comprehensive protection rate and safety results leave a positive signal for the benefit/risk evaluation in the elderly population.
Summary
Overall, AbogenABO1020 mRNAThe global Phase III clinical trial of the vaccine has achieved the expected evaluation objectives and standards. Meanwhile, based on the evaluation results of humoral immunity and immune mechanisms, it elucidated the response to mainstream strains in China.2The actual situation is that the immune protection established by the inactivated COVID-19 vaccine is relatively weak.Through the first vaccination2DosemRNAVaccines can break through immune imprinting and provide effective cross-protection against new mutant strains.
This study has several limitations, including the elderly population and prior vaccinations.3The sample size of the population receiving the inactivated COVID-19 vaccine is relatively small, and the results of the corresponding subgroup analysis need to be further observed and validated in a larger population. The immunogenicity subgroup only tested the neutralizing antibodies of live virus for humoral immunity, lacking detection data and related analysis of cellular immune responses. If future studies could explore this further, it might allow for additional discussion on the first vaccination in the population with basic immunity from the inactivated COVID-19 vaccine from the perspective of cellular immunity.2DosemRNAThe Necessity of Vaccines.
In April 2024, the WHO Technical Advisory Group on COVID-19 Vaccine Composition (TAG-CO-VAC) recommended the use of the monovalent JN.1 lineage as an antigen in future COVID-19 vaccine formulations. Although the ABO1020 antigen sequence BA.4/5 is no longer the predominant circulating strain, the results of this Phase III clinical trial are nonetheless a commendable achievement for Abogen's mRNA-LNP technology platform. In the post-COVID era, the broader application and development directions of mRNA technology, as well as the new competitive landscape of China's mRNA sector, have become hot topics of discussion within the industry. The RSV mRNA vaccine has been approved for marketing, the influenza mRNA vaccine succeeded in Phase III clinical trials, and neoantigen mRNA vaccines for cancer treatment have achieved proof-of-concept (POC) success. mRNA vaccines show great potential in applications such as cancer treatment and infectious diseases, with clinical concept validation already completed in several areas. Following the clinical validation of its mRNA technology platform, whether Abogen can advance the development of more product pipelines remains to be seen.