GSK's Blenrep Emerges as a Dark Horse in Multiple Myeloma with Breakthrough Combination Therapy Data Supporting New MAA

GSK
Pharmaceutical R&D Manufacturer
On July 22, 2024, the European Medicines Agency (EMA) accepted GSK's Marketing Authorization Application (MAA) for Blenrep (Belantamab mafodotin), an antibody-drug conjugate (ADC) targeting B-cell maturation antigen (BCMA), in combination with bortezomib plus dexamethasone (BorDex) or pomalidomide plus dexamethasone (PomDex), for the treatment of relapsed or refractory multiple myeloma (RRMM).
This application is based on the interim results of Phase 3 clinical trials DREAMM-7 and DREAMM-8, both of which met their primary endpoints, demonstrating a statistically significant and clinically meaningful improvement in progression-free survival (PFS) for the Blenrep combination therapy group compared to the standard treatment group. The median PFS for patients receiving Blenrep combination therapy (N=243) was 36.6 months (95% CI: 28.4-NR), nearly two years longer than the 13.4 months (95% CI: 11.1-17.5) observed in the active control group (N=251). Patients receiving Blenrep combination therapy experienced a nearly 60% reduction in the risk of disease progression or death (HR: 0.41, 95% CI: 0.31-0.53, p<0.00001), achieving the primary endpoint of this trial.
As for the key secondary endpoint of overall survival (OS), the median OS for both groups has not yet been reached. However, the Blenrep combination therapy has already demonstrated early and significant clinical benefits (HR: 0.57, 95% CI: 0.40-0.80, p=0.00049), and follow-up for OS is still ongoing.
In later-line treatment, Carvykti (BCMA CAR-T), the star product for MM, showed a PFS of 34.9 in the CARTITUDE-1 clinical trial.months, while J&J announced the early clinical data of PFS 20.9 for the combination therapy of its CD3/BCMA bispecific antibody (Teclistamab) and CD3/GPRC5D bispecific antibody (Talquetamab).Months.
As the world's first BCMA-targeted ADC therapy, Blenrep received accelerated approval from the FDA in 2020 as a monotherapy for adult patients with relapsed or refractory multiple myeloma (RRMM) who have previously received at least four prior lines of therapy, including an anti-CD38 monoclonal antibody, a proteasome inhibitor, and an immunomodulatory agent.
Within just five months of approval, and solely from its use in late-line clinical applications, Blenrep generated $43 million in revenue for GSK. In 2021, it achieved a performance of $122 million. In the second quarter of 2022, Blenrep’s revenue grew by 43% year-over-year, reaching $36 million.
However, in November 2022, GSK suddenly announced that Blenrep did not meet the clinical endpoint in the Phase III trial DREAMM-3 for RRMM. The DREAMM-3 study is a "head-to-head" superiority trial designed to evaluate the efficacy comparison of Blenrep monotherapy versus pomalidomide combined with low-dose dexamethasone (PomDex).
In the study, the median PFS for Blenrep was 11.2 months compared to 7 months for PomDex; secondary endpoints included overall response rate (ORR), duration of response (DOR), and overall survival (OS). The ORR for Blenrep and PomDex was 41% and 36%, respectively; the 12-month DOR rates were 76.8% and 48.4%, respectively. Safety was consistent with prior trials.
The failure of this confirmatory trial was a devastating blow to Blenrep. After all, the basis for the FDA's accelerated approval of its market entry was the belief that the ultimate benefits would be proven. Just 15 days after Blenrep’s confirmatory trial failed, GSK, at the request of the FDA, swiftly withdrew the drug from the U.S. market.
Obviously, GSK has not abandoned the development of Blenrep, but has quickly achieved success by making adjustments to the clinical plan.
Blenrep is composed of a humanized anti-BCMA monoclonal antibody and the cytotoxic drug MMAF conjugated via a non-cleavable linker (Figure 1), which can eliminate myeloma cells through multiple mechanisms of action.
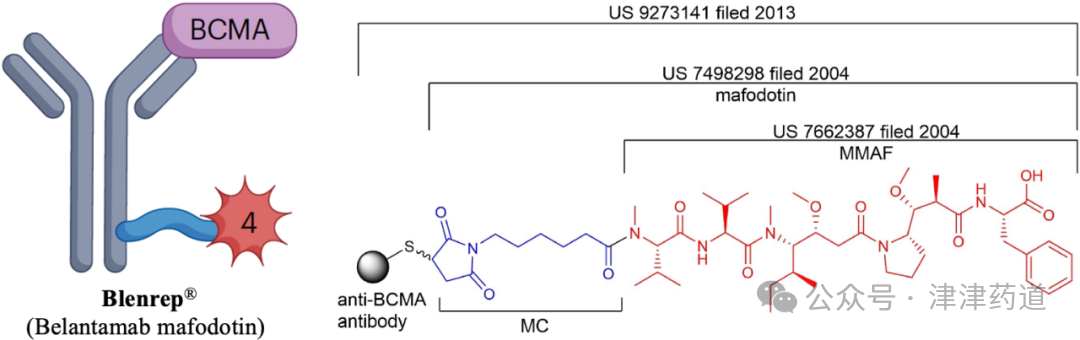
Figure 1. Schematic diagram of Blenrep structure
As the entire ADC field focuses its efforts on solid tumors, Blenrep's clinical success reminds us that ADCs still have great potential in hematological malignancies. Moreover, ADCs used for blood cancers often do not require bystander killing, so the considerations for Linker/Payload selection may differ from those for solid tumor ADCs.
It is currently impossible to predict the impact of Blenrep on the market share of bispecific antibodies and CAR-T. In the future, bispecific antibodies, CAR-T, and ADC may coexist in the long term in MM treatment, and their combination may bring better therapeutic effects.
Currently, Chinese companies that have laid out ADCs for hematological tumors include at least GPRC5D-ADC (LM-305; already transferred to AstraZeneca) by Limin Pharmaceuticals, BCMA-ADC (JS115) by Junshi Biosciences, and BCMA-ADC (HDP-101) by Huadong Medicine. We look forward to their clinical performance.
Scan the WeChat QR code to add the editor of the Antibody Circle.Those who meet the requirements can join the Antibody Circle WeChat group!
Please indicate: Name + Research Direction!