Patients with extensive-stage small cell lung cancer (ES-SCLC) have a high response rate to first-line treatment, but they almost always experience rapid recurrence and require subsequent treatment. In the United States, before June 2020, Topotecan was the only drug approved for second-line treatment of SCLC. On June 15, 2020, Lurbinectedin was granted accelerated approval by the FDA as a new option for second-line therapy in ES-SCLC. Topotecan remains the only authorized drug for second-line SCLC treatment in the European Union.
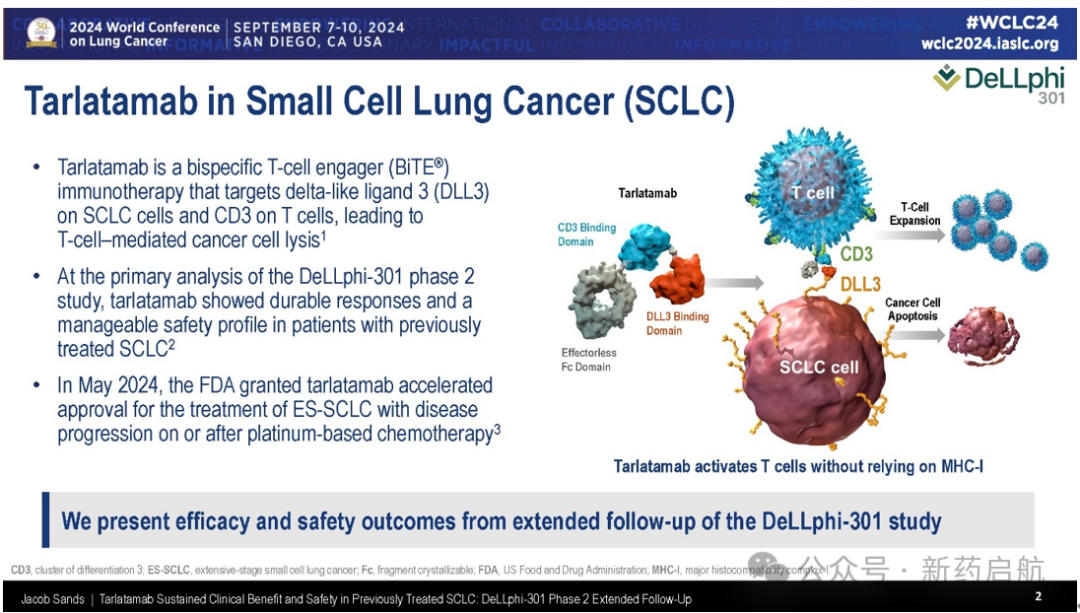
On May 16, 2024, the FDA granted accelerated approval to AMGEN's DLL3/CD3 TCE drug tarlatamab-dlle for second-line treatment of ES-SCLC, enabling targeted therapy. At the WCLC 2024 conference, clinical data updates for both Lurbinectedin and tarlatamab-dlle in second-line treatment of ES-SCLC were presented separately.AMGEN's tarlatamab-dlle,DeLLphi-300 (Phase I Clinical) and DeLLphi-301 (Phase II Clinical, Marketing Application Data) have been fully updated.
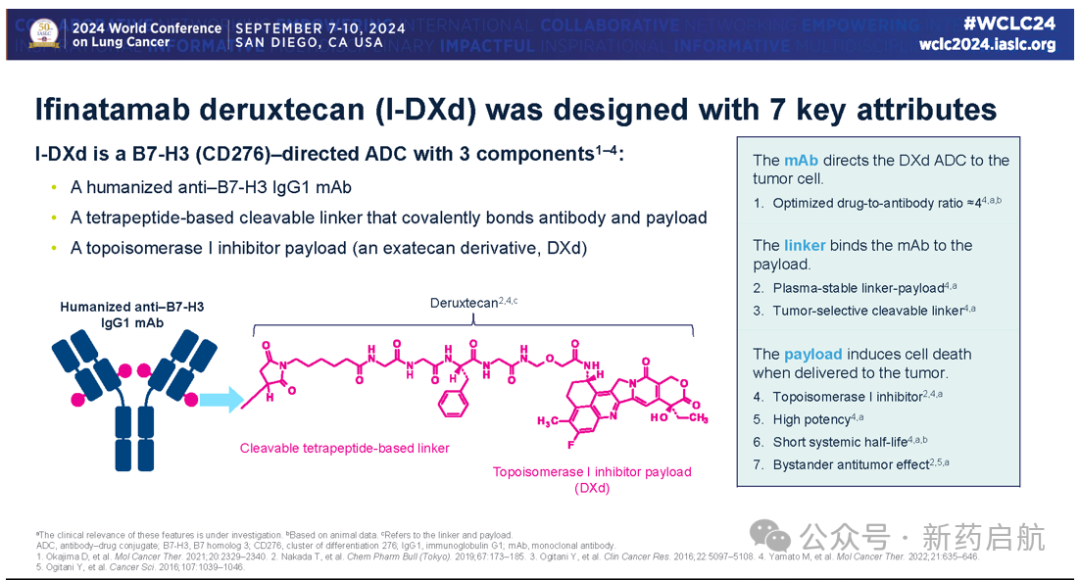
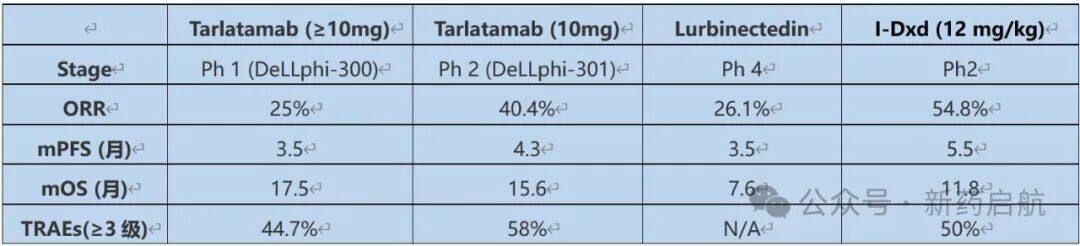
Among the second-line therapies under research for ES-SCLC, ADCs have attracted the most attention, particularly the B7-H3 targeted ADCs. At the recently concluded WCLC 2024 conference, Daiichi-Sankyo's B7-H3 ADC (ifinatamab deruxtecan) released complete Phase II clinical data. Taking this opportunity, a comprehensive comparison of tarlatamab vs B7-H3 ADC vs Lurbinectedin is conducted.If OS is used as the gold standard, the Phase II clinical result of tarlatamab shows an mOS of 15.6 months, the Phase II clinical result of I-Dxd shows an mOS of 11.8 months, and the real-world Phase 4 mOS of Lurbinectedin is 7.6 months.DLL3TCE OS Data Superior to Two Other TherapiesOf course, no direct head-to-head studies have been conducted between different therapies, and baseline differences among patients make direct comparison of trial results inappropriate. Tarlatamab and I-DxdAre undergoing phase III clinical trials of controlled chemotherapy. The ultimate mystery of which is the best second-line treatment for ES-SCLC will be revealed in two years. Not only that,In August this year, MSD and Daiichi-Sankyo announced a collaboration to develop DLL3 TCE, showing a strong momentum to promote the combination of DLL3 TCE and B7-H3 ADC, further competing with Amgen's DLL3 TCE in the SCLC field.
DeLLphi-300
Trial Update
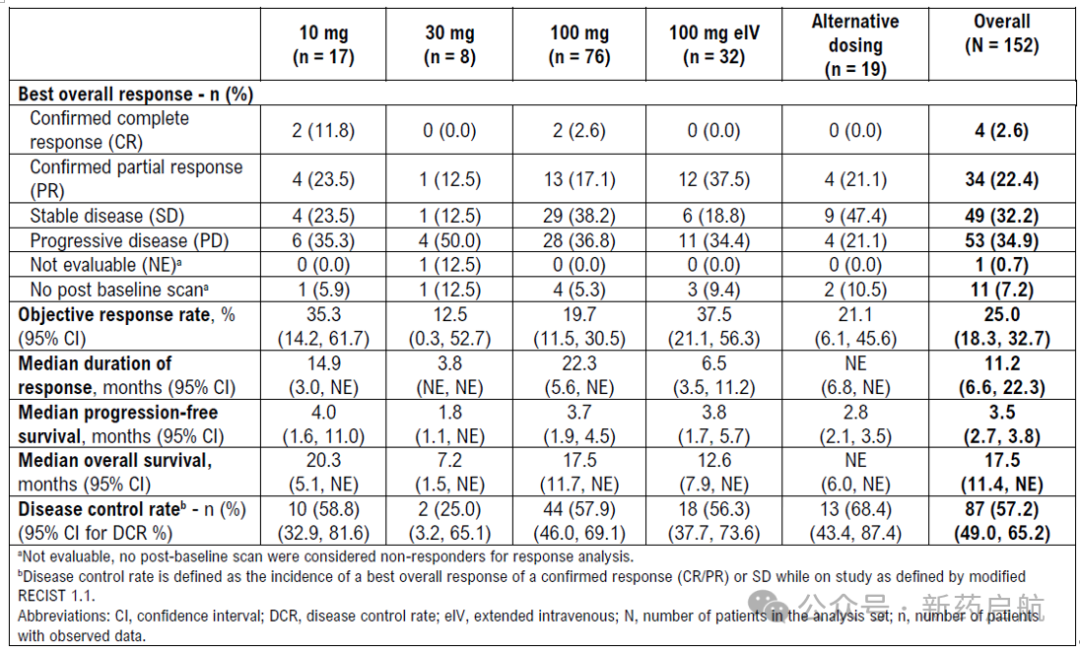
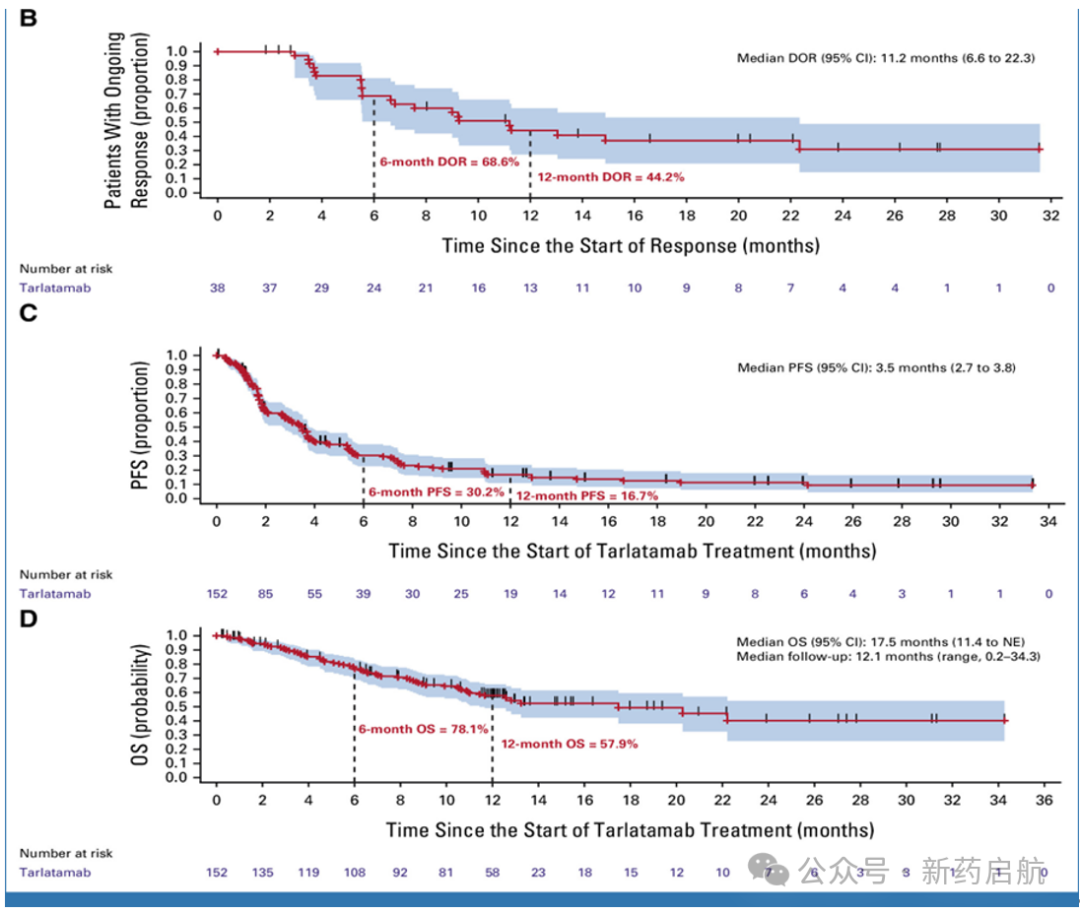
DeLLphi-300TarlatamabPh1 trial, as of October 2, 2023, hasA total of 152 patients received tarlatamab treatment at a dose ≥10 mg.,The median number of previous treatment lines was 2. At baseline, 38 patients (25.0%) had brain metastases. Among the 129 patients with evaluable baseline tumor samples, DLL3 expression was detected in 121 (93.8%). The median follow-up time was 12.1 months (range, 0.2-34.3).In general,ORR was 25.0%(95% confidence interval, 18.3 to 32.7), including four CRs and 34 PRs.mDOR was 11.2 months(95% confidence interval, 6.6 to 22.3),Thirteen patients (34.2%) had a DOR of 12 months or longer, and four patients (10.5%) had a DOR of 24 months or longer.At the data cutoff, 12 patients (31.6%) were still in ongoing remission.Three of the four patients with complete remission have a DOR of at least 20 months, and the response is still ongoing.All 33 responders with evaluable baseline tumor samples had detectable DLL3 expression. DLL3 expression data were unavailable for five responders. Overall,mPFS was 3.5 months (95% confidence interval, 2.7 to 3.8), mOS was 17.5 months (95% confidence interval, 11.4 to not estimable [NE]).。
DeLLphi-301
Trial Update
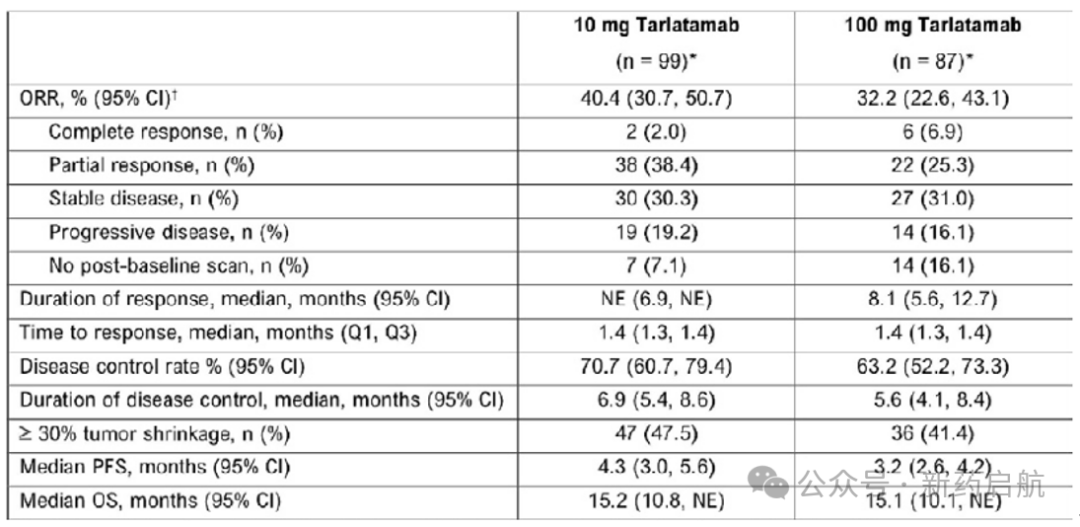
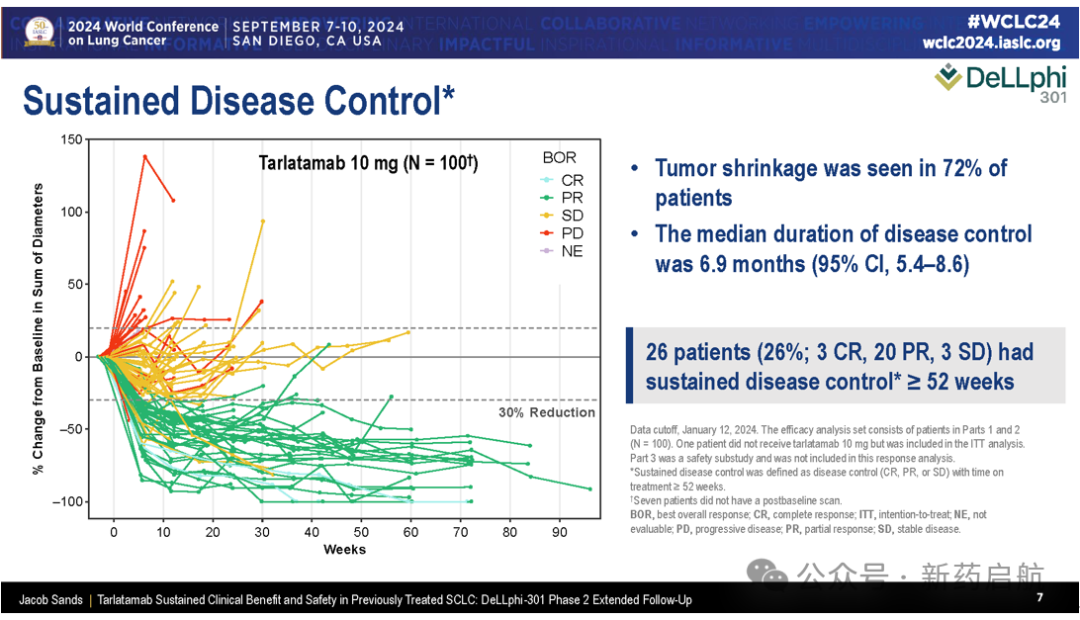
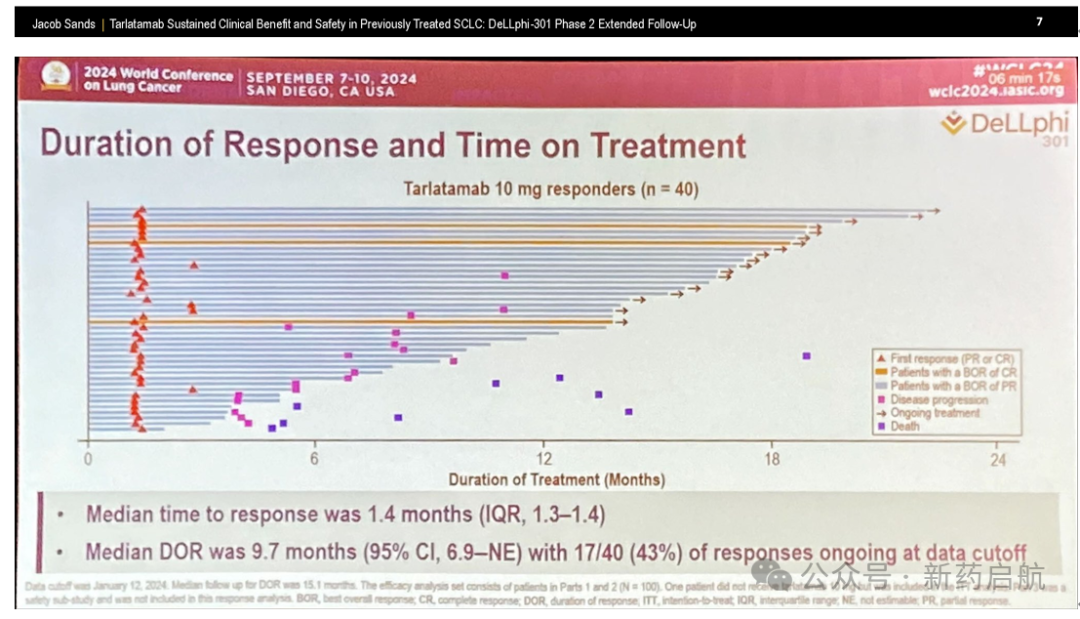
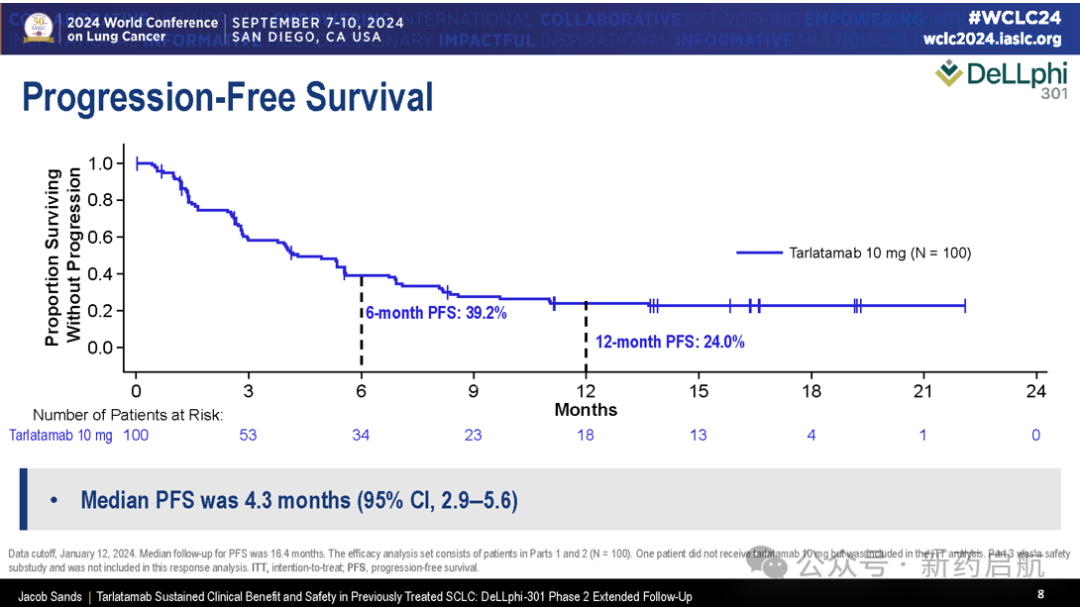
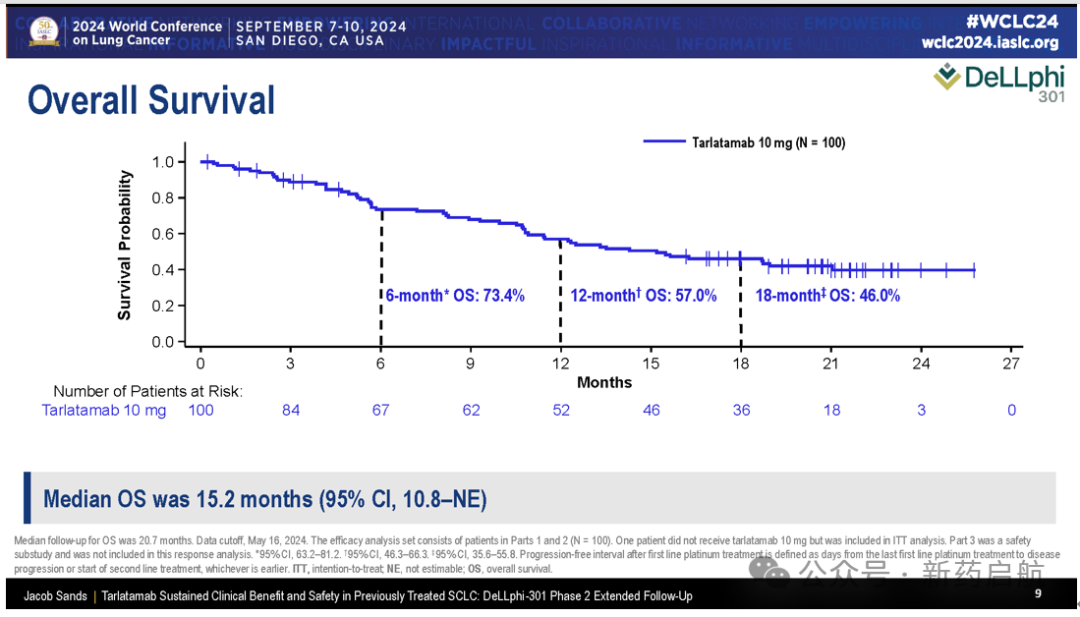
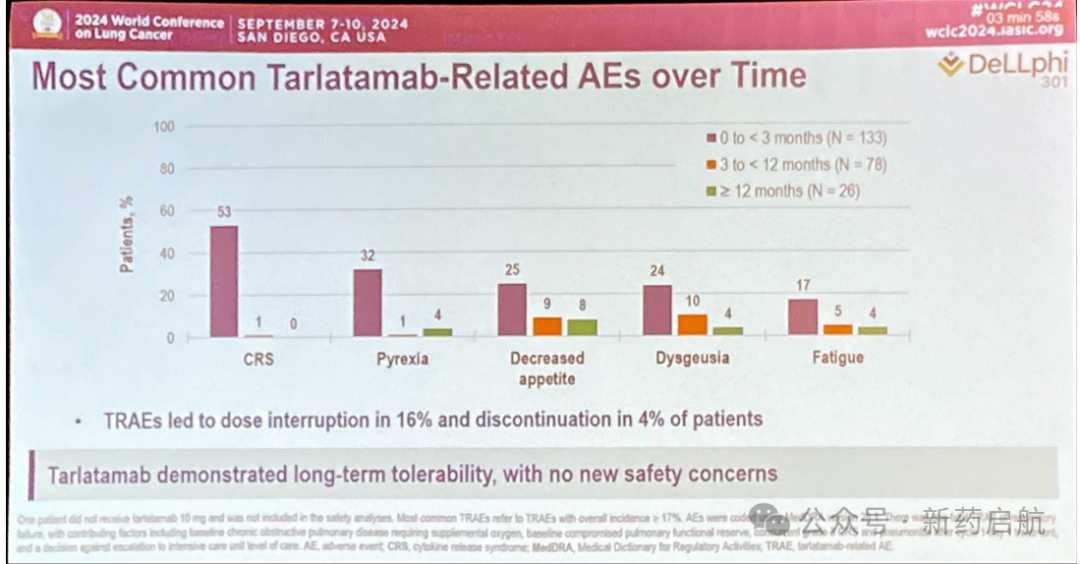
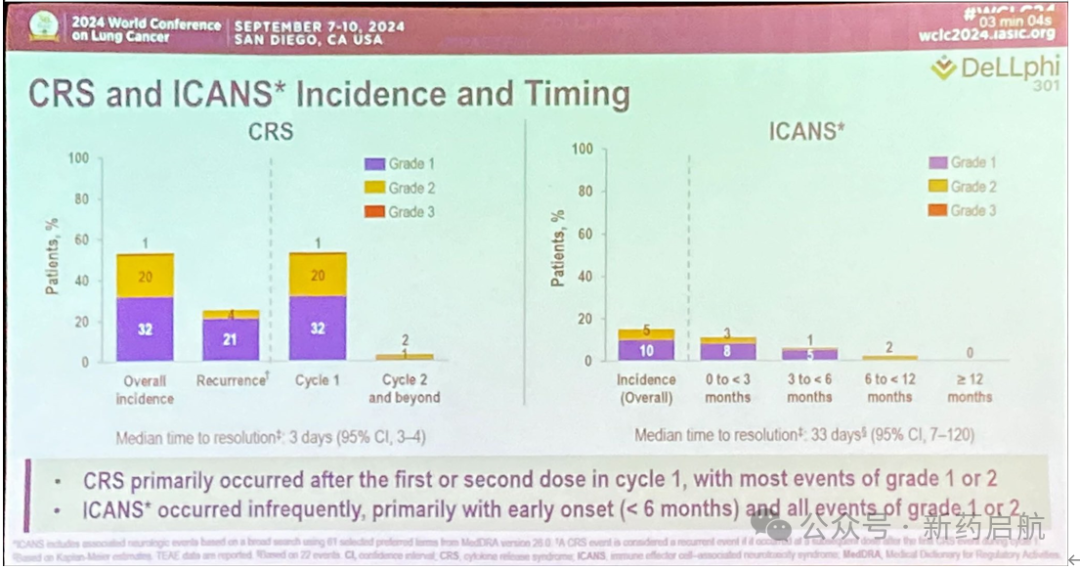
DeLLphi-301 Ph2 Trial in China,A total of 220 patients received treatment with tarlatamab. During the long-term follow-up for efficacy outcomes,The median follow-up time was 13.6 months.(Range 0.1-20.9). For the 10mg dose group, the selected dose for the subsequent Ph3 trial,The ORR was 40.4%, and the mDOR could not be estimated because 19 (47.5%) responders were still responding at the data cutoff. The mPFS for the 10mg dose group was 4.3 months, and the mOS was 15.2 months, with Kaplan-Meier OS estimates of 73.4% at 6 months and 56.7% at 12 months.I-Dxd:IDeate-Lunng01
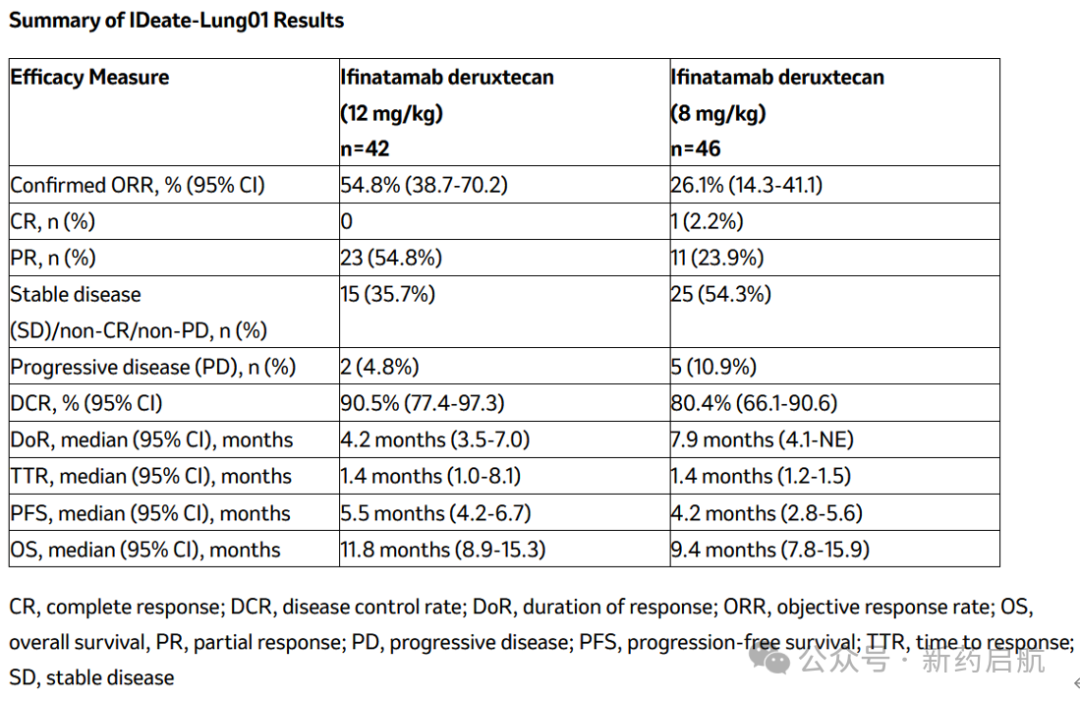
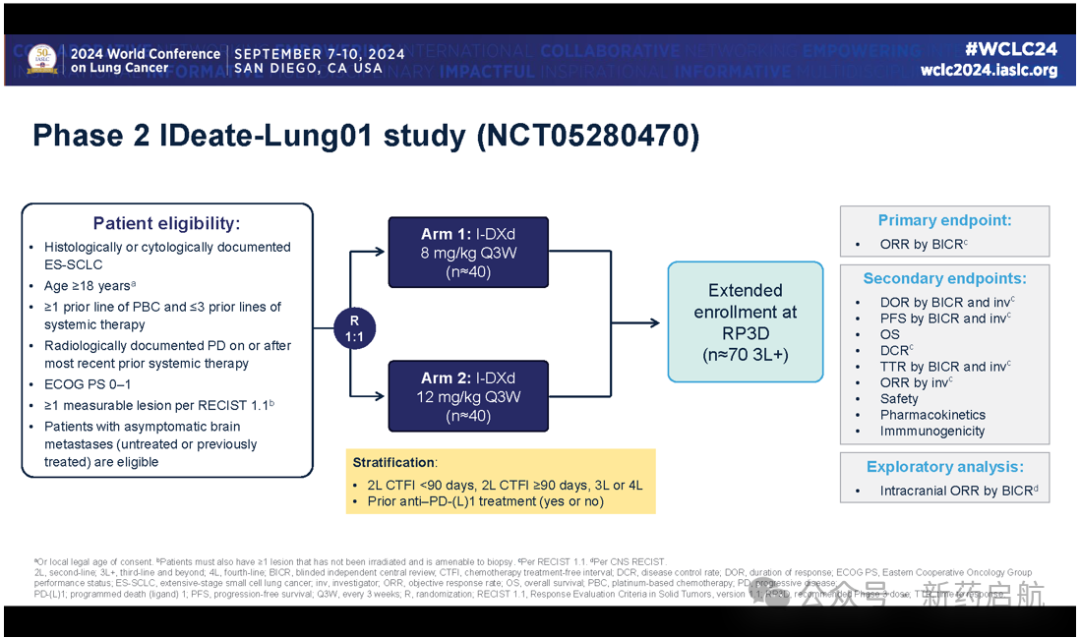
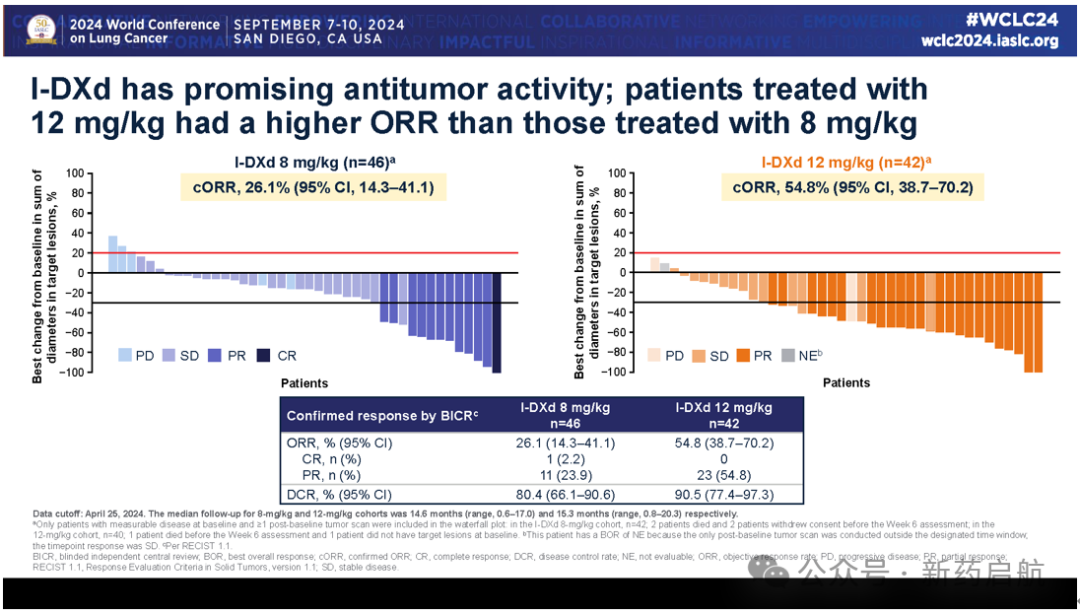
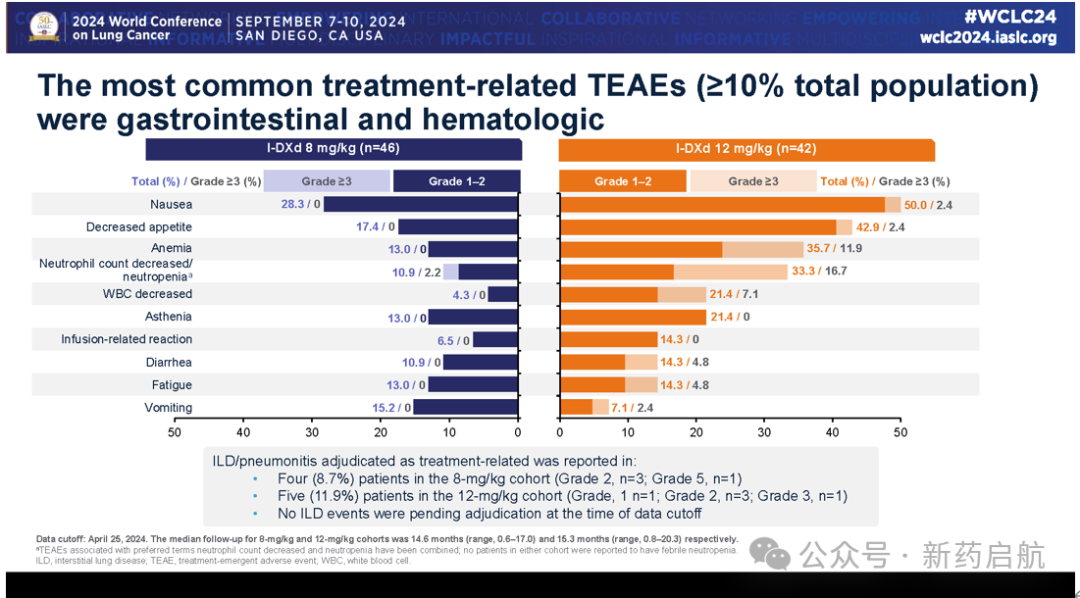
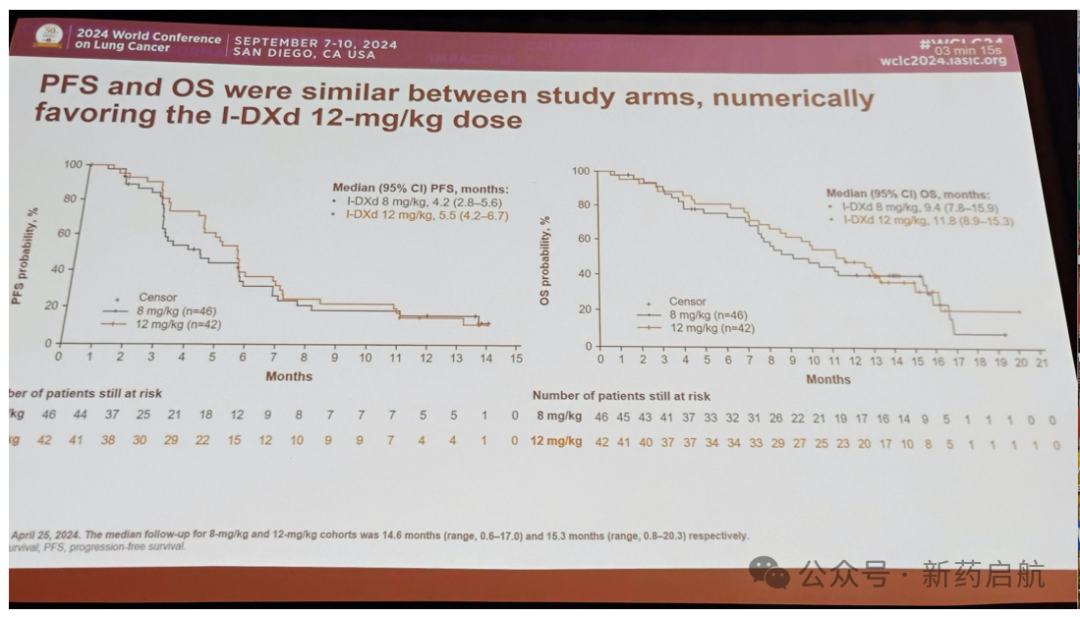
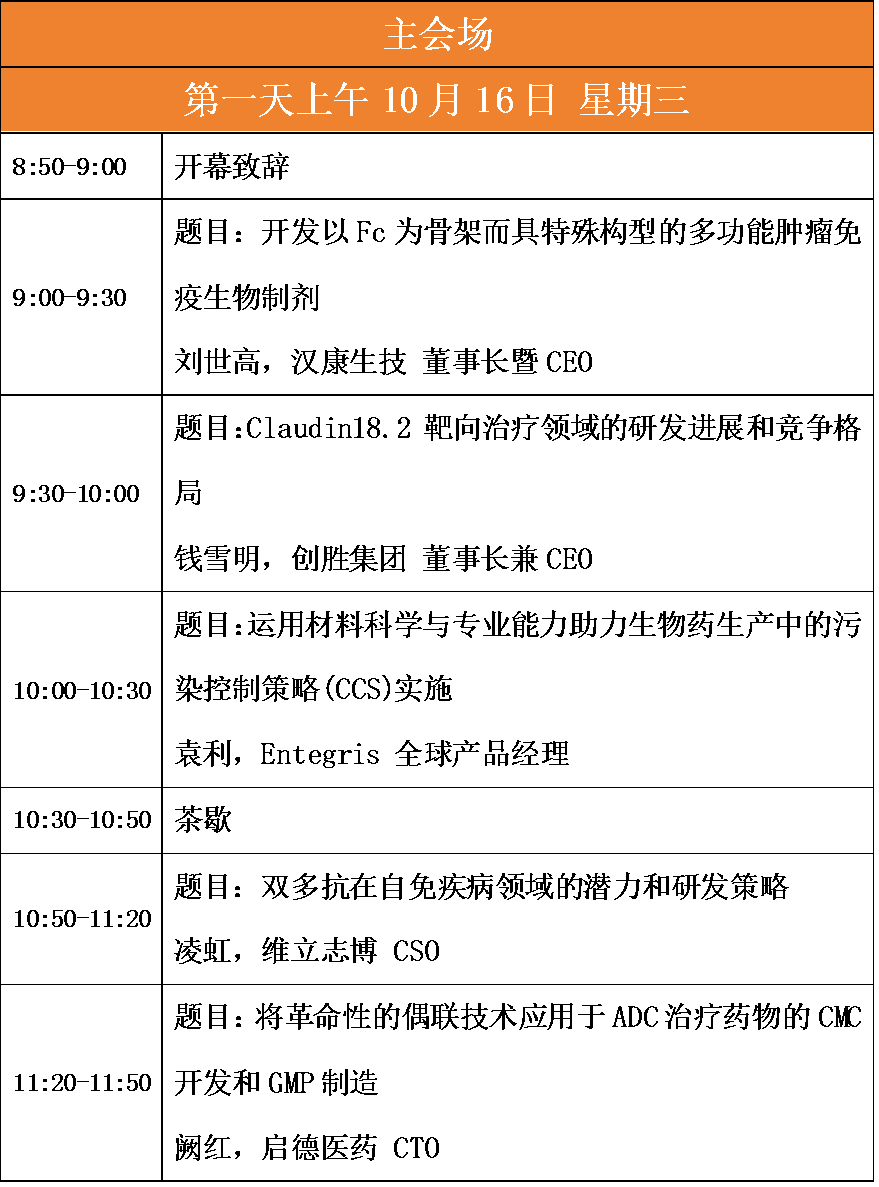
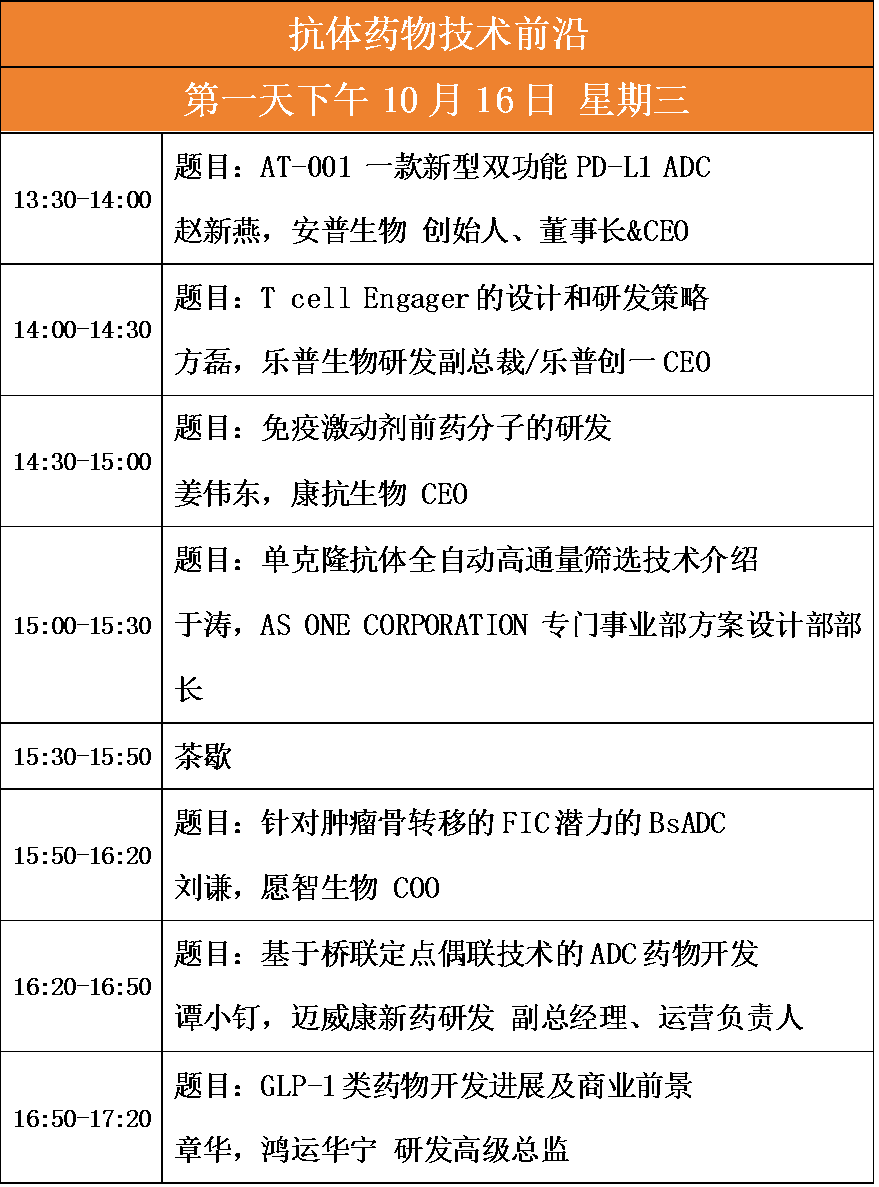
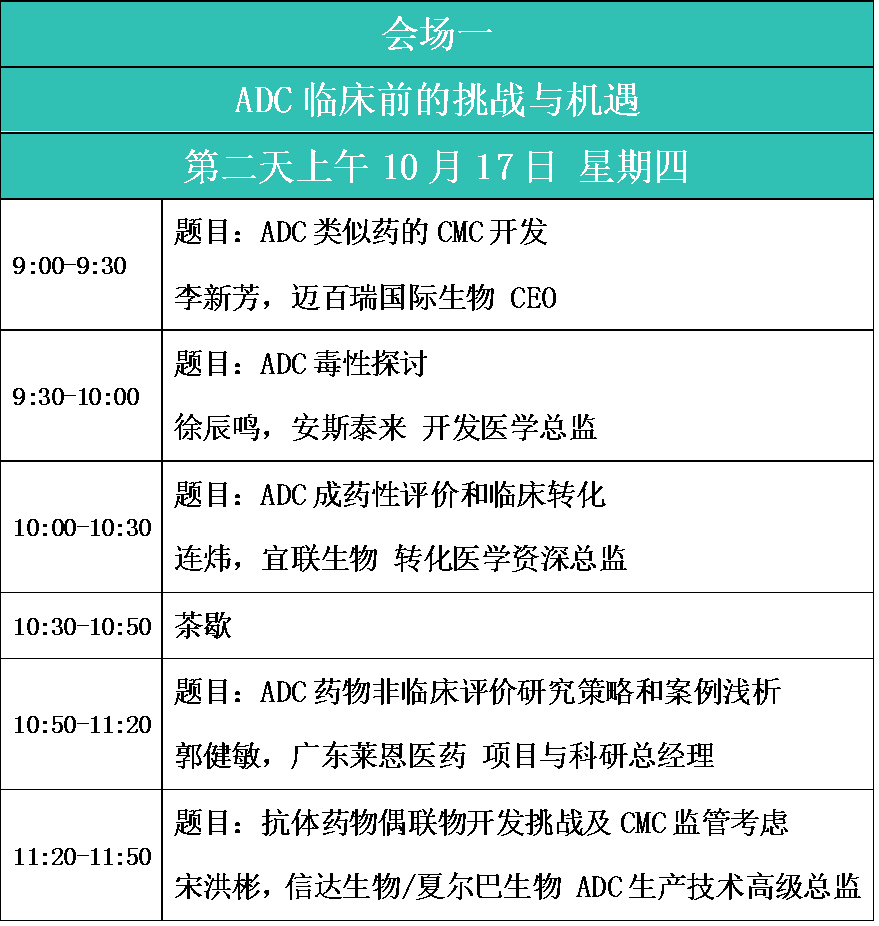
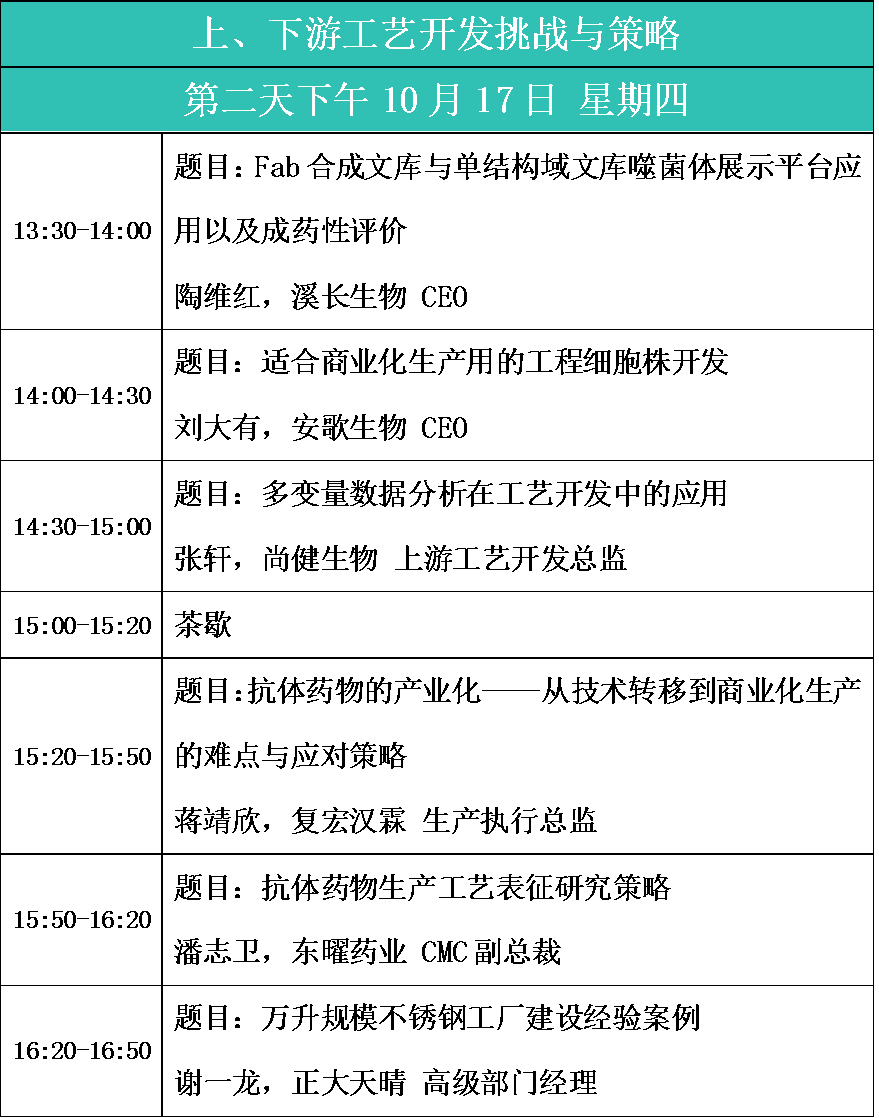
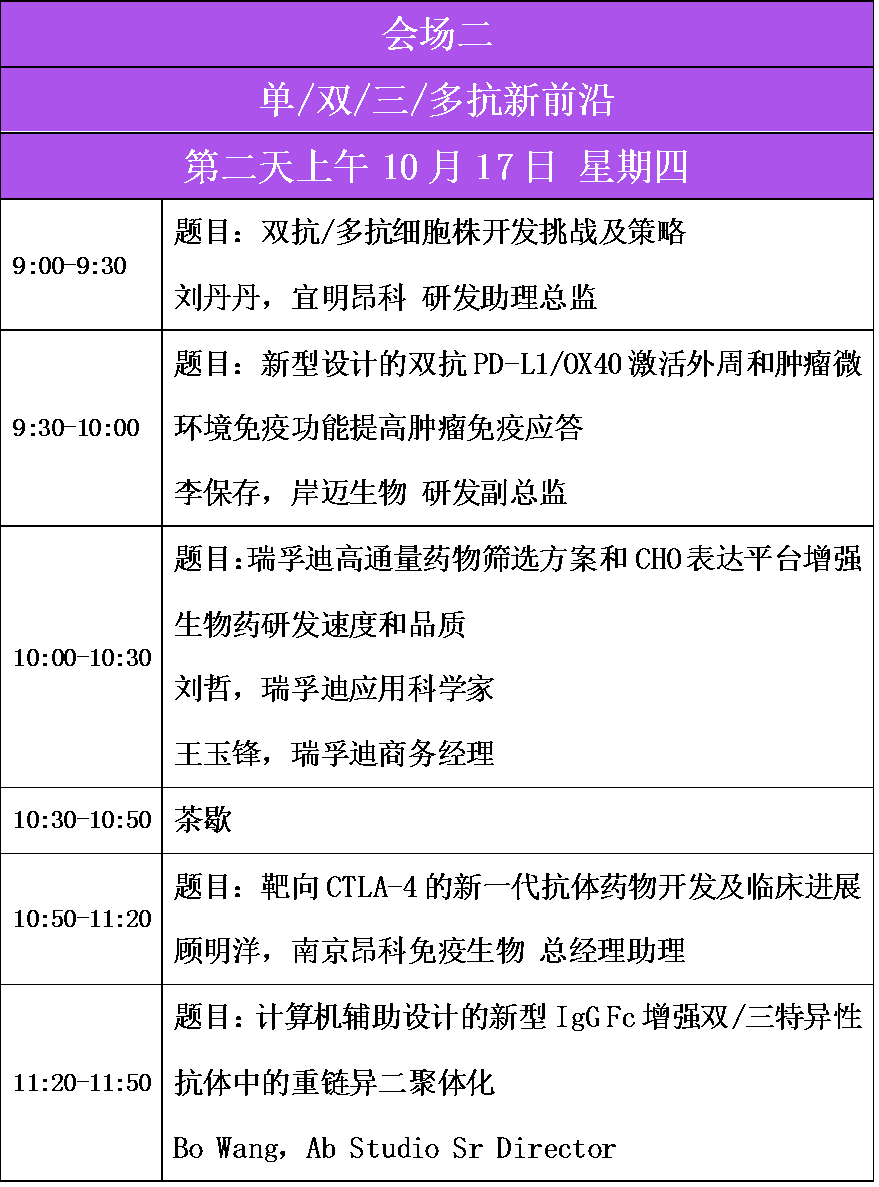
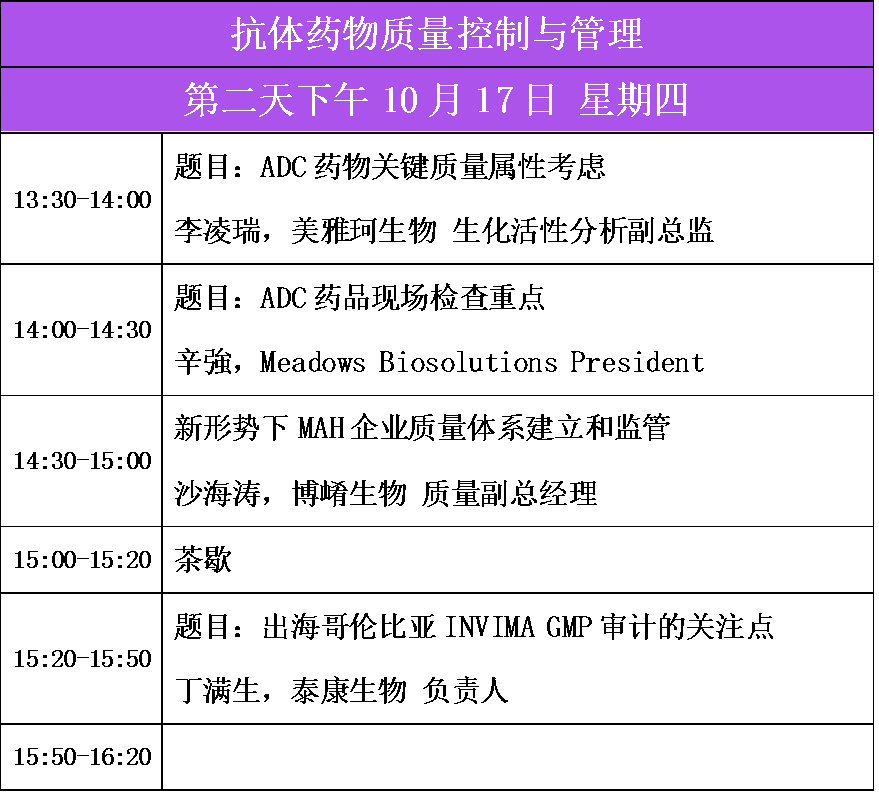
Trial UpdateIDeate-Lung01 is a global, multicenter, randomized, open-label Phase II study to evaluate the safety and efficacy of ifinatamab deruxtecan in patients with ES-SCLC. The study is divided into two parts: in the first part (dose optimization), patients had previously received at least one line of platinum-based chemotherapy and up to three lines of treatment. In the second part (dose expansion), patients had previously received at least two lines of systemic therapy.In ES-SCLC patients treated with ifinatamab deruxtecan at doses of 12 mg/kg (n=42) and 8 mg/kg (n=46), the ORR assessed by BICR was 54.8% (95% CI: 38.7-70.2) and 26.1% (95% CI: 14.3-41.1), respectively. In the 12 mg/kg group, 23 PRs were observed, while in the 8 mg/kg group, 1 CR and 11 PRs were observed. The mDoR for the 12 mg/kg and 8 mg/kg dose groups were 4.2 months (95% CI: 3.5-7.0) and 7.9 months (95% CI: 4.1-NE), respectively, and the DCR was 90.5% (95% CI: 77.4-97.3) and 80.4% (95% CI: 66.1-90.6), respectively. The mPFS for the 12 mg/kg and 8 mg/kg dose groups were 5.5 months (95% CI: 4.2-6.7) and 4.2 months (95% CI: 2.8-5.6), respectively, and the mOS was 11.8 months (95% CI: 8.9-15.3) and 9.4 months (95% CI: 7.8-15.9), respectively. As of the data cutoff on April 25, 2024, the median follow-up time was 15.3 months (95% CI: 13.6-16.2) for the 12 mg/kg group and 14.6 months (95% CI: 13.4-16.5) for the 8 mg/kg group. In the subgroup of patients with brain target lesions at baseline, assessed by central nervous system (CNS) BICR, intracranial ORRs of 50.0% (95% CI: 18.7-81.3) and 66.7% (95% CI: 22.3-95.7) were observed in the 12 mg/kg (n=10) and 8 mg/kg (n=6) dose groups, respectively. In these patients, two intracranial CRs were observed in each dose group. Three and two intracranial PRs were observed in the 12 mg/kg and 8 mg/kg dose groups, respectively, along with five and two SD cases.The safety profile observed in IDeate-Lung01 was consistent with the safety profile of ifinatamab deruxtecan observed in previous trials, with no new safety signals identified. In the 12 mg/kg (n=42) and 8 mg/kg (n=46) dose groups, 50.0% and 43.5% of patients experienced treatment-emergent adverse events (TEAEs) of Grade 3 or higher, respectively. The most common treatment-related TEAEs (>20% of the total population) across both doses included nausea (50.0% and 28.3%), decreased appetite (42.9% and 17.4%), anemia (35.7% and 13.0%), neutropenia (33.3% and 10.9%), leukopenia (21.4% and 4.3%), and fatigue (21.4% and 13.0%). Five (11.9%) and four (8.7%) cases of interstitial lung disease (ILD)/pneumonia were adjudicated as treatment-related by the independent adjudication committee in the 12 mg/kg and 8 mg/kg groups, respectively. Most ILD events (four in the 12 mg/kg group and three in the 8 mg/kg group) were low-grade (Grade 1 or 2). There was one Grade 3 (12 mg/kg) and one Grade 5 (8 mg/kg) ILD event. As of the data cutoff date of April 25, 2024, no ILD events were pending adjudication. Treatment discontinuation due to adverse events occurred in 16.7% and 6.5% of patients in the 12 mg/kg and 8 mg/kg dose groups, respectively.In the IDeate-Lung01 trial, patients receiving ifinatamab deruxtecan were treated with a median of two prior lines of therapy in both dose groups, including the majority (76.1%) who had previously received immunotherapy. The median treatment duration was 4.7 months (range: 0.03–15.2) in the 12 mg/kg dose group and 3.5 months (range: 0.03–13.9) in the 8 mg/kg dose group.Lurbinectedin: Jazz EMERGE 402 Trial UpdateLurbinectedin monotherapy has been approved in many countries, including the United States and Canada, for the treatment of 2L (United States) or 3L/metastatic (Canada) SCLC after progression following platinum-based chemotherapy. Jazz EMERGE 402 is a Phase 4 clinical study based on real-world data, evaluating the real-world efficacy and safety of lurbinectedin in patients with ES-SCLC.As of January 2, 2024, a total of 171 patients had received at least one cycle of lurbinectedin treatment; among them, 13 (8%) were still undergoing treatment, and 158 (92%) had discontinued treatment, with disease progression being the most common reason (104 cases [66%]). The median (range) age was 67 years (29-89 years); 37 patients (22%) had an ECOG score ≥2; 35 patients (20%) had CNS metastases. Baseline characteristics of patients with a chemotherapy-free interval (CTFI) of less than 90 days versus 90 days or more were generally similar. Lurbinectedin monotherapy was administered to 92 patients (54%) as second-line treatment (2L), and to 59 patients (35%) as third-line treatment. The median (range) number of cycles of lurbinectedin was 4 (1-31), with a duration of exposure of 105 days (21-694 days). In 2L patients assessed by RECIST v1.1, the objective response rate (ORR) in the overall population was 26.1%; ORRs for patients with CTFI <90 days and CTFI ≥90 days were 22.7% and 32.4%, respectively. In the overall population, the median progression-free survival (mPFS) and median overall survival (mOS) for 2L were 3.5 months and 7.6 months, respectively; for patients with CTFI ≥90 days, mPFS and mOS were 4.0 months and 11.9 months, respectively. Similar ORR and mPFS were observed between patients evaluated by RECIST and non-RECIST criteria. Treatment-emergent adverse events (TEAEs) occurred in 64 patients (37%); notable adverse events of interest included grade 3 or higher anemia (4.1%), neutropenia (6.5%), and thrombocytopenia (5.9%).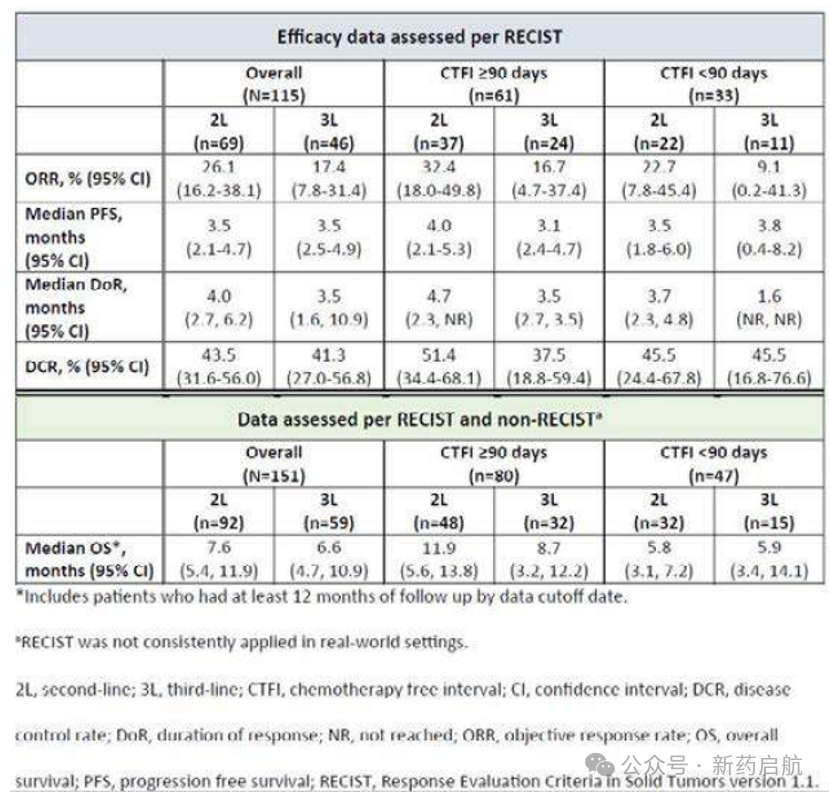 Chemotherapy-free interval (CTFI) refers to the time interval between the completion of first-line chemotherapy and disease recurrence. This indicator is particularly important in lung cancer treatment as it helps doctors evaluate the patient's response to prior chemotherapy and determine subsequent treatment strategies. For instance, a longer CTFI suggests that the patient responded well to first-line chemotherapy and may benefit from receiving a similar regimen again. Conversely, a shorter CTFI may indicate that the patient was not sensitive to the previous chemotherapy regimen, necessitating consideration of alternative treatments. In the treatment of small cell lung cancer (SCLC), CTFI is often used to assess whether a patient is suitable for re-administration of the first-line treatment regimen. According to the guidelines of the National Comprehensive Cancer Network (NCCN), patients with a CTFI ≥ 180 days can be considered for re-challenging with the first-line treatment regimen. In some studies, patients with a CTFI ≥ 90 days are also deemed eligible for re-administration of the first-line treatment. Lurbinectedin, as a new treatment option, has demonstrated promising efficacy and acceptable safety in second-line treatment of SCLC, especially in patients with a longer CTFI.To promote communication and innovation in the antibody industry,October 16-17, 2024The 7th Golden Autumn October Antibody Industry Development ConferenceAs scheduled. The conference aims to provide researchers with an interactive platform, which will help promote the further development of the antibody industry.
Chemotherapy-free interval (CTFI) refers to the time interval between the completion of first-line chemotherapy and disease recurrence. This indicator is particularly important in lung cancer treatment as it helps doctors evaluate the patient's response to prior chemotherapy and determine subsequent treatment strategies. For instance, a longer CTFI suggests that the patient responded well to first-line chemotherapy and may benefit from receiving a similar regimen again. Conversely, a shorter CTFI may indicate that the patient was not sensitive to the previous chemotherapy regimen, necessitating consideration of alternative treatments. In the treatment of small cell lung cancer (SCLC), CTFI is often used to assess whether a patient is suitable for re-administration of the first-line treatment regimen. According to the guidelines of the National Comprehensive Cancer Network (NCCN), patients with a CTFI ≥ 180 days can be considered for re-challenging with the first-line treatment regimen. In some studies, patients with a CTFI ≥ 90 days are also deemed eligible for re-administration of the first-line treatment. Lurbinectedin, as a new treatment option, has demonstrated promising efficacy and acceptable safety in second-line treatment of SCLC, especially in patients with a longer CTFI.To promote communication and innovation in the antibody industry,October 16-17, 2024The 7th Golden Autumn October Antibody Industry Development ConferenceAs scheduled. The conference aims to provide researchers with an interactive platform, which will help promote the further development of the antibody industry.Time:October 16-17, 2024
Location: Shanghai(Hotel Directional Notice)
Scale:600-800 people
Organizer:Biopharmaceutical Circle, Antibody Circle
Speech Support:Entegris, Rui Fu Di, AS ONE CORPORATION
Conference Fee:Free FREE!(Only charge100YuanRegistration deposit (including participation in learning sessions, tea breaks, and conference materials; the deposit is non-refundable), first come, first served, registration will close once full.!
Registration Method:Scan the QR code below or click "Read Original" at the bottom of the article → Fill out the form → Registration successful (Volunteer registration,Undertake certain work, please consider carefully, no deposit required.)!
After the organizing committee receives the registration information, they will conduct an initial screening based on the provided details and further communicate with registrants for confirmation to extend precise invitations. Those who pass the strict review process will ultimately have the opportunity to join the conference WeChat group.
More guests are being invited.
Scan the WeChat QR code to add the editor of Antibody Circle.Those who meet the requirements can join the Antibody Circle WeChat group!Please indicate: Name + Research Direction!All articles reproduced in this official account are intended to convey more information, with the source and author clearly stated. Media or individuals who do not wish to be reprinted may contact us (cbplib@163.com), and we will immediately delete the content. All articles represent the views of the author and do not represent the position of this website.