Sac-TMT and Dato-DXd Advance in EGFR-Mutant NSCLC: Clinical Updates on NDAs and Phase III Initiations

Kelun-Biotech
Innovative Drug Developer

AstraZeneca
Biopharmaceutical Manufacturer

Daiichi-Sankyo
Pharmaceutical R&D Developer
2024Year10Month31Day, Kelun-BiotechTROP2 ADCLukansatuzumab (sac-TMT) Awarded the third itemNDA, used to treatEGFRTyrosine Kinase Inhibitor(EGFR-TKI)Progression after treatmentEGFRMutant locally advanced or metastatic non-small cell lung cancer(NSCLC)Patient. Previously,sac-TMTTreatment AcceptanceEGFR-TKIAnd failed to treat locally advanced or metastatic with platinum-based chemotherapyEGFRMutationNSCLCPatient'sNDAObtainedNMPAAccepted.
2024Year11Month1Day, AstraZeneca/Daiichi-Sankyo has initiatedTROP2 ADC Dato-DXd With or Without OsimertinibvsClinical Application of Platinum-based Doublet ChemotherapyIIIPhase Trial, Treatment for Osimertinib ResistanceEGFRMutation Non-SquamousNSCLC Patient.
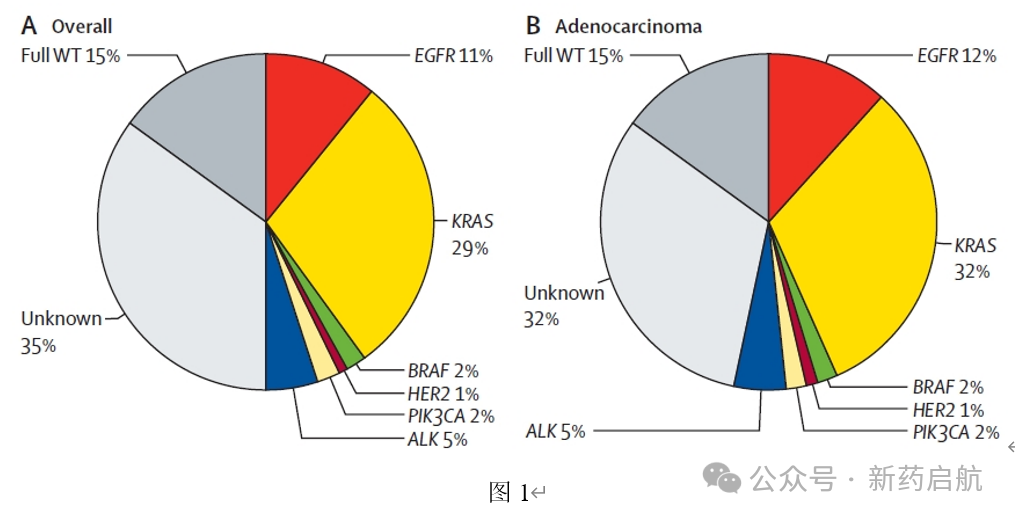
EGFRMutation isNSCLCThe most common driver gene mutations in China (Fig.1), mainly present in lung adenocarcinoma, accounting for approximately the entireNSCLCPatient's10%-20%, the proportion is higher among Asian patients, and in China this proportion can reach40%-50%。
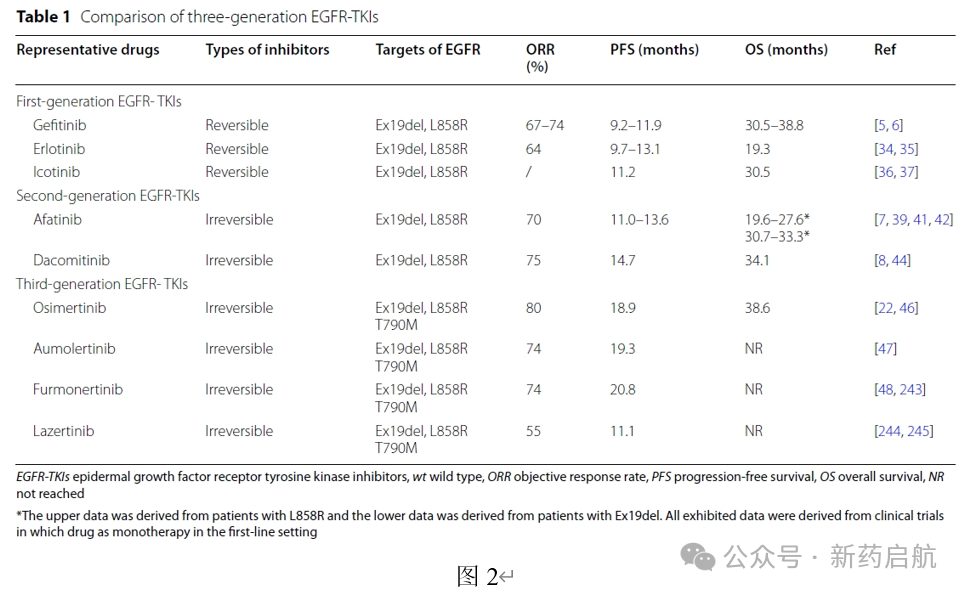
EGFRMutatedNSCLCThe first-line treatment of choice for patients isEGFR-TKI, among which the third generationEGFR-TKIOsimertinib (Osimertinib)ORRFor80%,PFS 18.9Months,OS 38.6Months (Fig.2)。
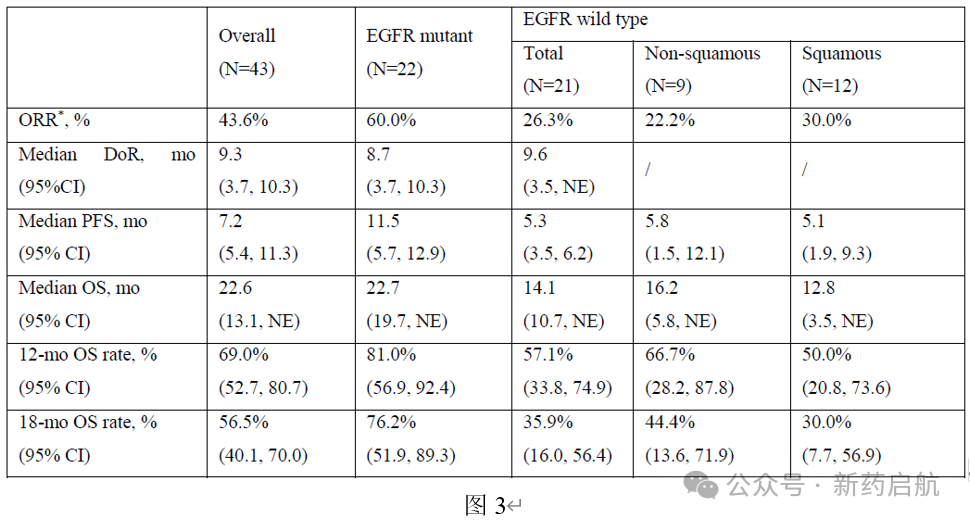
Treatment options are limited after osimertinib resistance, and immune checkpoint inhibitors (ICI) The efficacy and safety in drug-resistant populations are not ideal. ClinicallyIIThe data from the period indicates (Fig.3), Kelun-Biotechsac-TMTIn previously treated advanced NSCLC Overall in patientsORRFor43.6%, among whichEGFRMutated patients (TKIDrug resistance,50%At least one chemotherapy failure)ORRFor60.0%,EGFRWild-type patientsORRFor26.3%。EGFRMutant PatientsmPFSFor11.5Months,mOSFor22.7Months.
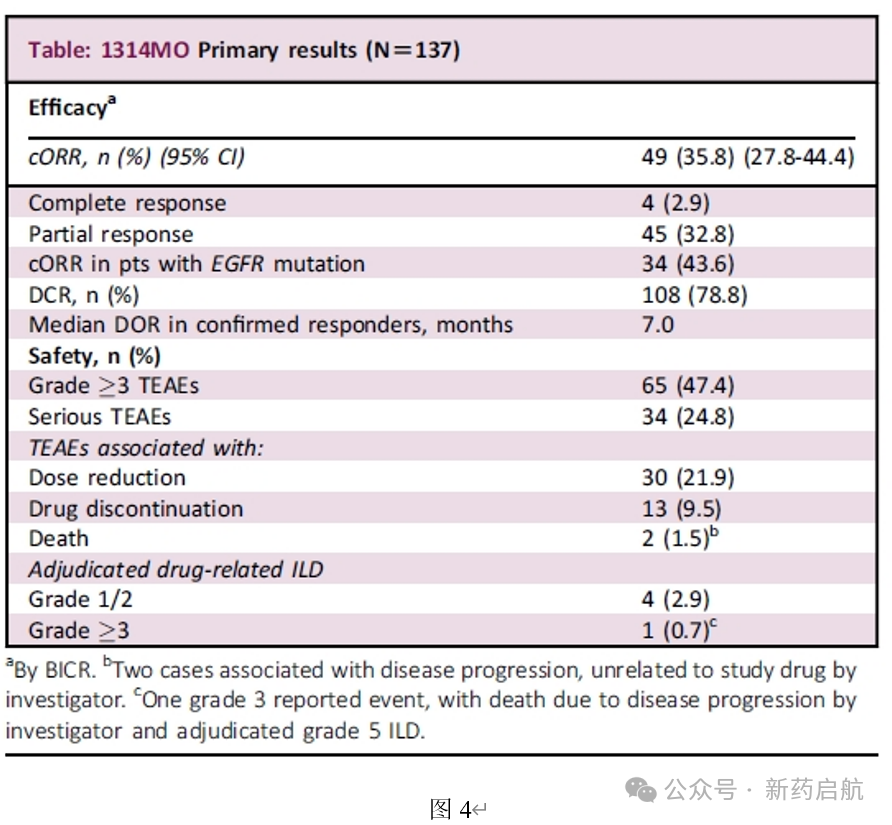
Dato-DXdIn targetable gene mutations(Actionable genomic alterations , AGA)TheNSCLCOnORRFor35.8%, among whichEGFRMutant population (accounting for the entireAGAPopulation56.9%) ofORRFor43.6%(Figure4)。
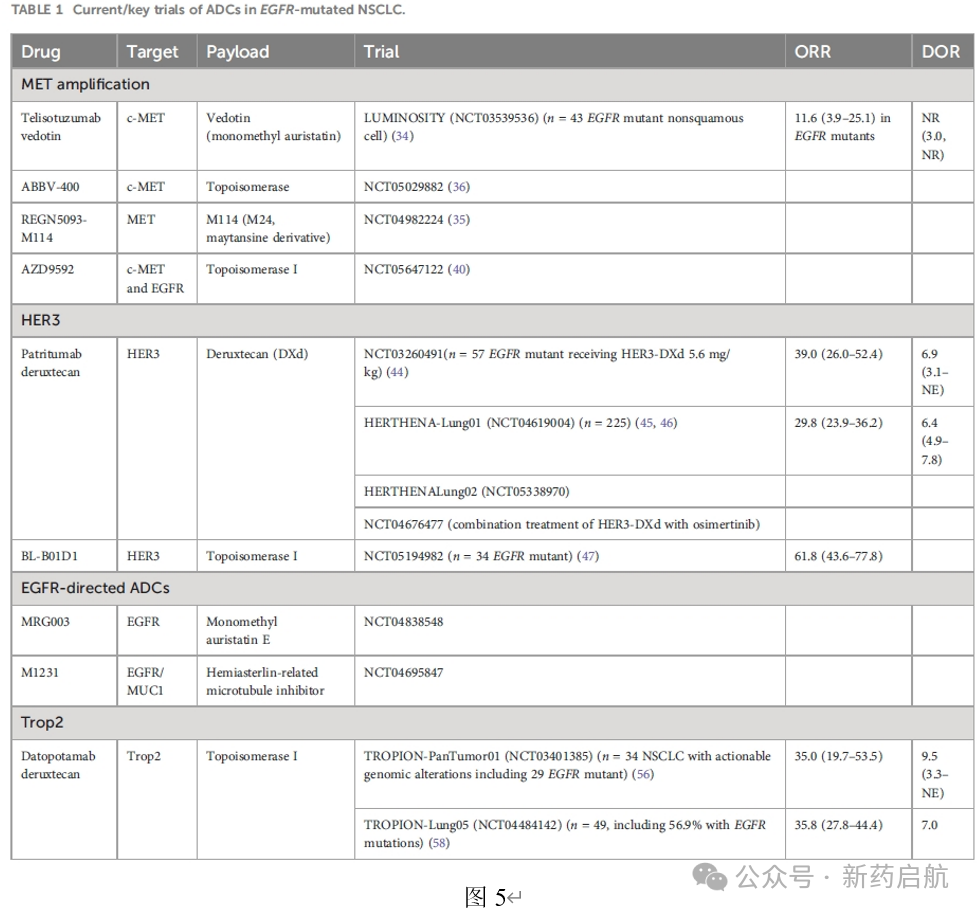
OthersADCInEGFRMutatedNSCLCClinical efficacy data in patients are shown in the figure.5As shown, where Baili TianhengEGFR/HER3Bispecific AntibodyADC BL-B01D1TheORRUp to61.8%. Daiichi-Sankyo'sHER3 ADC HER3-DXd ORRIn30%-40%, while the Yilian not included in the figureHER3 ADC YL202At dose escalationORRFor39.4%。
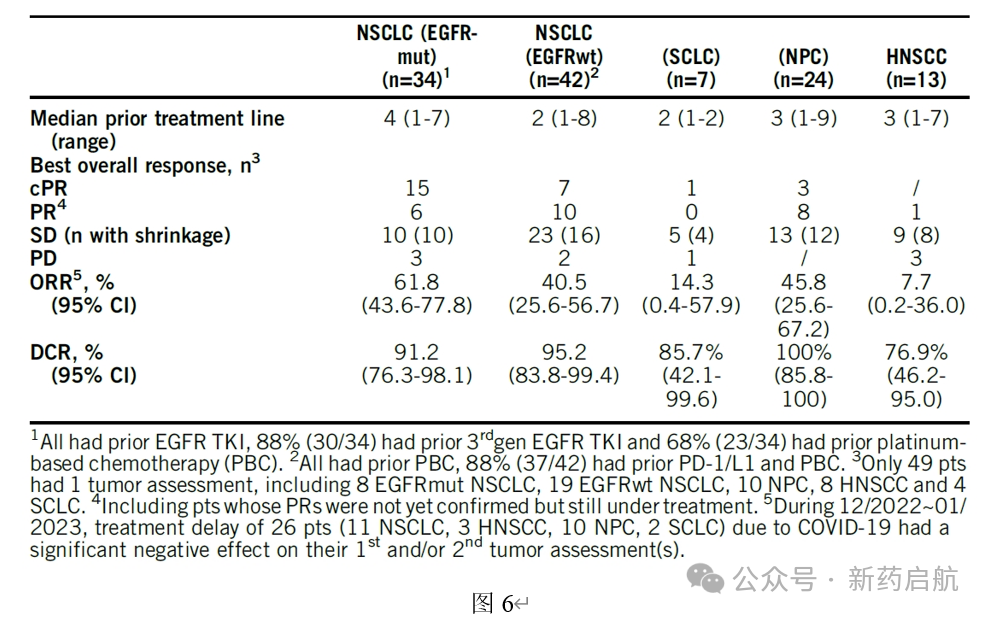
Besides inEGFRMutatedNSCLCA high response rate was observed among patients,BL-B01D1InEGFRWild-typeNSCLCIn patientsORRHas also been achieved40.5%(Figure6)。
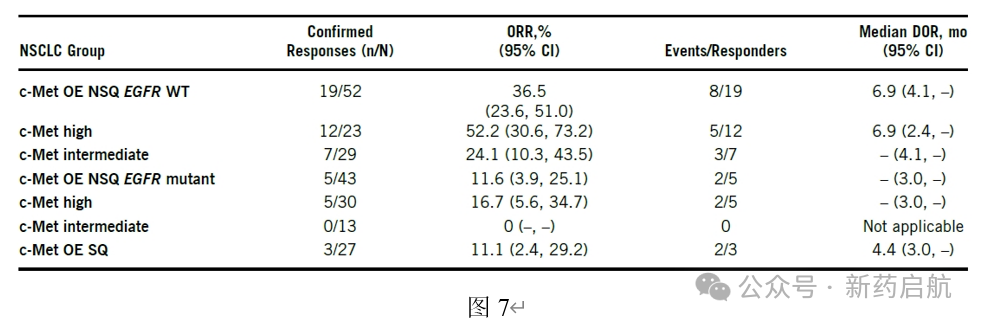
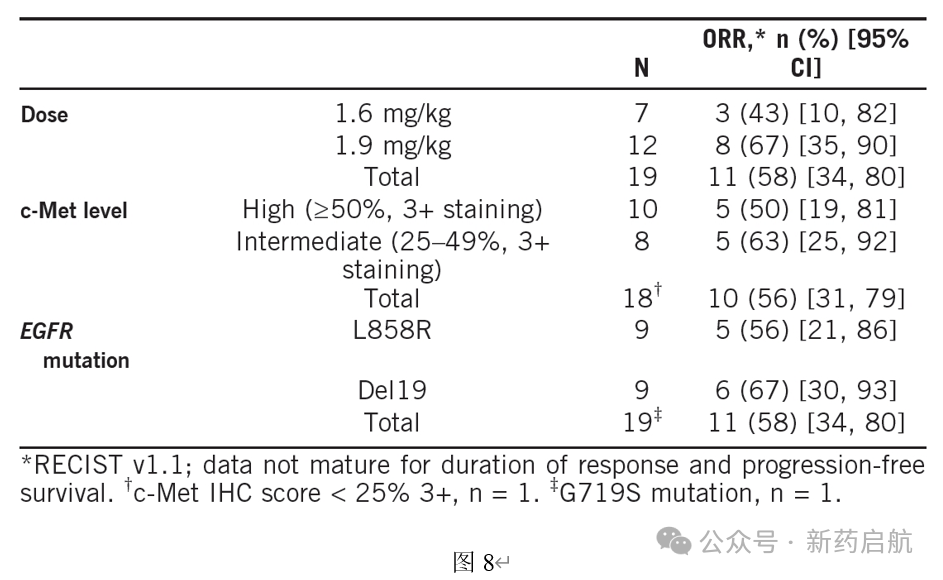
AbbVie'sc-Met ADC Teliso-VAs of2024Year9Moon PhaseFDASubmitBLAApplication, for the treatment of previously treated locally advanced or metastaticEGFRWild-type and c-MetProtein Overexpression in Non-SquamousNSCLCPatient.Teliso-VMonotherapy inEGFRMutation,c-MetHigh-expression non-squamousNSCLCIn patientsORROnly for11.6%`, much lower than`EGFRWild-type patients36.5%(Figure7). InTeliso-VCombined with Osimertinib in the Treatment of Osimertinib ResistanceEGFRMutation,c-MetHigh expressionNSCLCPatient'sphase 1/1bIn the trial,Teliso-V+ osimertinib TheORRFor58%(Figure8)。
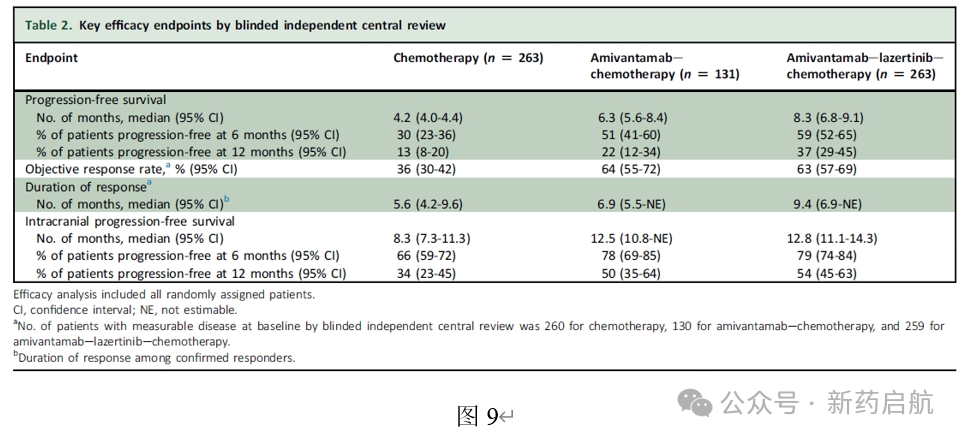
ADCIn addition to the intense competition, it will also face strong competition from other types of drugs. Johnson & JohnsonEGFR/c-MetBispecific AntibodyAmivantamabTheMARIPOSA-2Research shows (Figure9), for osimertinib resistanceEGFRMutationNSCLCPatient,Amivantamab+Chemotherapy (Carboplatin)+Pemetrexed),Amivantamab+Chemotherapy+ Lazertinib(Johnson & Johnson Third GenerationEGFR-TKI) ofORRRespectively64%And63%, superior to chemotherapy alone36%。PFSAndDORAlsoAmivantamab+Chemotherapy+LazertinibOptimal,Amivantamab+Chemotherapy comes second. Do the above data suggest thatEGFR/c-Met ADCWill it also achieve good efficacy in this population?