VOYXACT® Approved: First APRIL-Targeted Therapy for IgA Nephropathy

Otsuka
Drug Developer
Recently, Otsuka Pharmaceutical announced that its anti-APRIL monoclonal antibody, sibeprenlimab (brand name: VOYXACT®), has been officially approved by the National Medical Products Administration (NMPA) of China for the treatment of adult patients with primary IgA nephropathy.
As the first therapy selectively targeting APRIL (A Proliferation-Inducing Ligand), sibeprenlimab intervenes in disease progression at its source by blocking a key step in the generation of pathogenic IgA.
The product previously received accelerated approval from the U.S. FDA in November 2025, becoming the first approved APRIL-targeted therapy globally. Its once-monthly subcutaneous injection regimen is poised to shift IgA nephropathy treatment from "symptomatic control" into a new era of precise, etiology-targeted therapy focused on "source blockade."
40% of Patients Progress to Dialysis within 20 Years; Long-standing Gap in Etiologic Treatment for IgA Nephropathy
IgA nephropathy (IgAN) is the most common primary glomerular disease worldwide and a major cause of chronic kidney disease and end-stage kidney disease (ESKD).
Its pathogenesis is closely related to immune abnormalities—galactose-deficient IgA1 (Gd-IgA1) produced in patients can form immune complexes and deposit in the glomeruli, continuously triggering inflammatory responses and renal damage, ultimately leading to progressive decline in renal function.
The disease burden cannot be ignored. According to Frost & Sullivan data, there are currently approximately 4 to 5 million patients with IgA nephropathy in China, with over 100,000 new confirmed cases annually. As the disease predominantly affects young and middle-aged adults aged 20 to 40, the resulting medical and social burdens are particularly significant. Meanwhile, IgA nephropathy has an insidious onset; early-stage patients often present only with microscopic hematuria or mild proteinuria, and some patients already exhibit significant renal impairment at the time of diagnosis.
Despite the continuous improvement in disease understanding, IgA nephropathy has long lacked etiologic treatments. Over the past few decades, clinical management has primarily relied on regimens such as renin-angiotensin system (RAS) inhibitors, glucocorticoids, and immunosuppressants to control proteinuria and slow the progression of renal function decline.
However, these treatments primarily target the downstream manifestations during disease progression, making it difficult to directly intervene in the core immune mechanisms driving disease onset and progression. Meanwhile, long-term use of glucocorticoids and immunosuppressants may also pose safety risks such as infection and metabolic abnormalities. Prognostic data show that even with current standard treatment, approximately 20% to 40% of patients will still progress to end-stage renal disease within 20 years after diagnosis, requiring dialysis or kidney transplantation.
Persistent unmet clinical needs are driving intensified research and development of innovative drugs for IgA nephropathy. In recent years, as key pathogenic mechanisms—including the complement pathway, the endothelin pathway, and the APRIL/BAFF axis—have been progressively elucidated, the treatment of IgA nephropathy has begun to shift from supportive care to mechanism-directed therapy.
From a market perspective, according to data from Frost & Sullivan, the global market for IgA nephropathy therapeutic drugs is projected to grow from USD 567 million in 2020 to USD 1.196 billion in 2025, while the Chinese market is projected to grow from USD 37 million to USD 109 million, with a compound annual growth rate (CAGR) of 24.6%. Against this backdrop, the approval and market launch of sibeprenlimab, which targets the APRIL pathway, provides patients with a new option for precision therapy.
The First APRIL-Targeted Therapy: Blocking the Quadruple Hit at Its Source
To understand the innovative value of sibeprenlimab, it is first necessary to revisit the core pathogenic mechanisms of IgA nephropathy.
The pathogenesis of IgA nephropathy is commonly explained by the classic "Four-hit hypothesis." Briefly, patients continuously produce abnormal galactose-deficient IgA1, which further forms immune complexes that deposit in the glomeruli, triggering inflammatory responses and kidney injury.
In this process, APRIL is considered a key driver in the pathogenesis and progression of the disease. Studies have found that APRIL levels are significantly elevated in patients with IgA nephropathy, promoting B-cell maturation and plasma cell survival, thereby continuously driving the production of pathogenic Gd-IgA1. Consequently, APRIL has gradually emerged as an important target for the development of innovative therapies for IgA nephropathy.
Sibeprenlimab targets this critical step. As a humanized IgG2 monoclonal antibody, sibeprenlimab selectively binds to and neutralizes APRIL, blocking its interaction with receptors, thereby reducing the formation of pathogenic Gd-IgA1 and immune complexes, and intervening in the key pathogenic pathway of the disease.
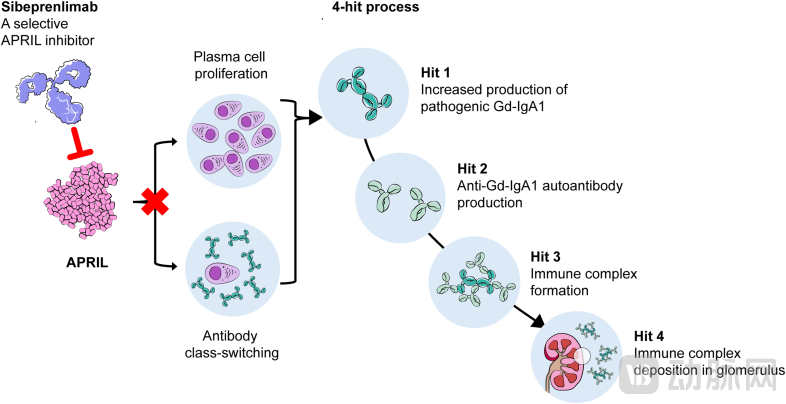
Mechanism of Action of Sibeprenlimab
(Ref:Evaluating Sibeprenlimab in IgA Nephropathy - Rationale and Baseline Data from the VISIONARY Trial,
doi:10.1016/j.ekir.2025.09.031)
This mechanistic innovation translates directly into multiple clinical advantages. Traditional RAS inhibitors (ACEIs/ARBs) and corticosteroids primarily act on downstream pathways, indirectly reducing proteinuria through blood pressure lowering and anti-inflammatory effects; however, they fail to halt the persistent production of Gd-IgA1, often leading to disease relapse upon discontinuation or dose reduction.
Sibeprenlimab blocks the pathogenic pathway upstream, targeting the core pathogenic mechanism of disease development rather than merely controlling superficial symptoms. Meanwhile, unlike broad-spectrum immunosuppressants that indiscriminately suppress the entire immune system, sibeprenlimab specifically targets the cytokine APRIL without directly depleting B cells. This approach inhibits the production of pathogenic IgA while preserving the body's normal immune defense capabilities, thereby offering a wider safety window.
In terms of medication experience, sibeprenlimab is administered via subcutaneous injection once every four weeks, allowing for self-administration by patients or administration by caregivers, thereby eliminating the need for frequent hospital visits—a significant improvement in treatment adherence for patients with chronic kidney disease who require lifelong management.
From the perspective of disease mechanisms, the approval of sibeprenlimab marks the first time that IgA nephropathy treatment has truly entered an era of "precision targeting and source blockade."
51.2% Reduction in Proteinuria: Significant Efficacy in Chinese Cohort
The approval of sibeprenlimab was based on the VISIONARY study, one of the largest global Phase III double-blind, placebo-controlled trials in the field of IgA nephropathy to date. The study enrolled 510 patients from 31 countries worldwide, including 102 patients from mainland China, and aimed to evaluate the efficacy and safety of sibeprenlimab administered as a 400 mg subcutaneous injection once monthly for 24 months.
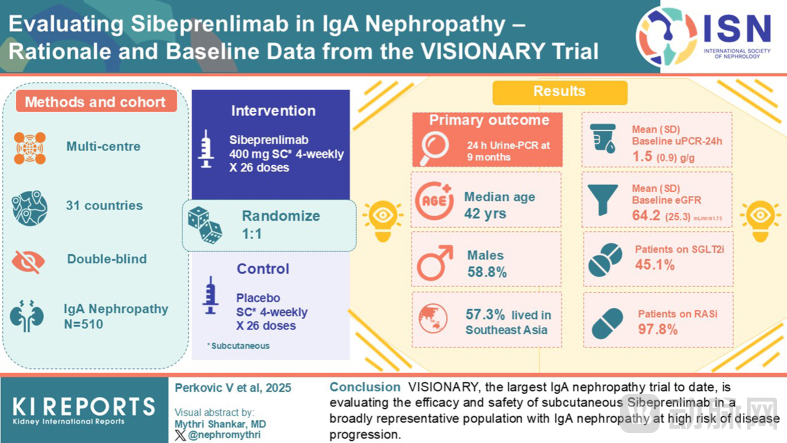
VISIONARY Study Design Overview Diagram
In terms of proteinuria control, the VISIONARY study showed that sibeprenlimab treatment for 9 months resulted in a significant 51.2% reduction in UPCR-24h compared with the placebo group, with the reduction further expanding to 54.3% at 12 months.
Compared with proteinuria remission, long-term renal function protection is the core metric for delaying uremia. The 12-month eGFR analysis showed that the mean change from baseline in the sibeprenlimab group was +0.7 mL/min/1.73m², whereas the placebo group experienced a decline of −4.8 mL/min/1.73m², resulting in a treatment effect difference of 5.5 mL/min/1.73m² between the two groups. This indicates that while effectively reducing proteinuria, sibeprenlimab demonstrates positive signals in stabilizing renal function—a benefit particularly critical for IgA nephropathy, a chronic disease characterized by progressive renal function decline.
In terms of safety, the incidence of TEAEs in the sibeprenlimab treatment group was 76.3%, lower than the 84.5% observed in the placebo group; the incidence of serious adverse events was only 3.9%, with no deaths reported. The overall tolerability was favorable, and no new safety signals were identified. This profile, balancing efficacy and tolerability, makes it more aligned with the needs of chronic disease management for IgA nephropathy, which requires lifelong care.
Data from the Chinese cohort are even more compelling. The interim analysis of the Chinese subgroup presented at WCN 2026 showed that, at 9 months of treatment, the placebo-adjusted reduction in uPCR-24h among Chinese patients was approximately 62%, highly consistent with the results from the global primary cohort, and representing the most favorable uPCR reduction data reported to date in Phase III clinical studies of IgA nephropathy patients in China.
Sibeprenlimab Accelerates Global Rollout as IgA Nephropathy Advances Toward Multi-Mechanism Therapy
With positive results from pivotal Phase III studies, sibeprenlimab has accelerated its global registration and commercialization, gradually transitioning from an investigational product to the global market.
Sibeprenlimab was initially developed by the US biotechnology company Visterra. In July 2018, Otsuka Pharmaceutical completed the acquisition of Visterra for approximately $430 million, incorporating multiple innovative renal disease pipelines, including sibeprenlimab, into its own R&D system and continuing to advance its global clinical development and registration.
As a global pharmaceutical company headquartered in Japan, Otsuka has long focused on therapeutic areas including neuropsychiatry, kidney diseases, and oncology, adhering to an innovation-driven R&D strategy guided by unmet clinical needs. Following years of clinical development, sibeprenlimab received accelerated approval from the FDA in November 2025, becoming the first approved APRIL-targeted therapy globally. In June 2026, it further received conditional marketing approval from China's NMPA, marking it as the first biologic agent approved in China for the treatment of IgA nephropathy and signifying the formal entry of this innovative mechanism into clinical application.
The launch of sibeprenlimab has further enriched the therapeutic options for IgA nephropathy. In recent years, as research into the disease's pathogenesis has deepened, innovative drug development has gradually shifted from traditional supportive care to mechanism-oriented therapy. Following the sequential approval of innovative therapies targeting gut mucosal immunity, the endothelin pathway, and the complement pathway, the addition of APRIL-targeted therapy has helped establish a multifaceted treatment landscape for IgA nephropathy characterized by parallel mechanistic approaches.

Innovative Therapeutic Agents for IgA Nephropathy Approved in China and Their Primary Mechanisms of Action
For patients with IgA nephropathy, clinical treatment over the past few decades has primarily focused on reducing proteinuria and slowing the decline of renal function. The approval of sibeprenlimab not only adds a new treatment option with a clearly defined mechanism of action but also further validates the clinical value of the APRIL pathway as a therapeutic target for IgA nephropathy.
In the future, the complete 24-month data from the VISIONARY study and additional real-world evidence will be released sequentially, potentially further validating its clinical benefits in long-term renal function preservation. Meanwhile, the continuous launch of drugs with novel mechanisms of action is expected to drive IgA nephropathy treatment toward greater precision and personalization.