Attenuated CD3 Bispecific Antibody Etentamig: Strong Efficacy and Enhanced Safety Profile Supported by MONVISO Trial Data

AbbVie
Innovative Drug Developer

BCMA-Targeted Therapies (CAR-T, ADCs, Bispecific Antibodies) Are Rapidly Entering First-Line Treatment for Multiple Myeloma (MM). This Raises a New Question: What Should Be the Next Target After BCMA-Targeted Therapy Fails? More Importantly—Is There Still Room for Further Development of the BCMA Target Itself?
《Bispecific Antibody Enters Phase III Trials: Roche Poised to Storm Johnson & Johnson’s Core Territory!》In the article, we learn about RocheFcRH5 TCE Bispecific Antibody inDemonstrated promising efficacy in patients who had failed BCMA-targeted therapy, positioning it as a potential candidate treatment for BCMA resistance; furthermore,AbbVie’s etentamig (ABBV-383) provided a different answer with data from the MONVISO study: when administered immediately after BCMA CAR-T failure, the overall response rate (ORR) remained at 64%; furthermore, prophylactic administration of tocilizumab reduced the incidence of cytokine release syndrome (CRS) to 0%.
etentamigMolecular Design: Bispecific BCMA, Low-Affinity CD3, Silent Fc
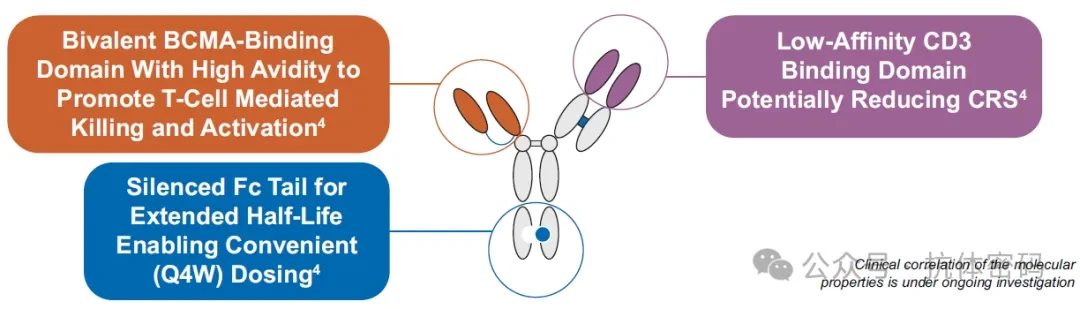
Etentamig is a BCMA×CD3 bispecific T-cell engager, with a molecular architecture featuring three characteristics that distinguish it from existing BCMA bispecific antibodies.
1) Bispecific BCMA: Unlike the monovalent BCMA-binding mode of most BCMA×CD3 bispecific antibodies, etentamig adopts a bivalent design that theoretically provides higher antigen-binding avidity, enabling effective binding even to tumor cells with low BCMA expression. This is particularly critical for patients who have undergone BCMA-targeted therapy—as will be discussed below, downregulation of BCMA expression is a common phenomenon following CAR-T cell therapy failure.
2)Low-affinity CD3: Reducing CD3-binding affinity is a validated strategy for mitigating cytokine release syndrome (CRS), as demonstrated by molecules such as teclistamab. Etentamig intentionally features lowered CD3 affinity, with the design objective of reducing the risk of systemic T-cell hyperactivation while maintaining T-cell-mediated cytotoxic activity.
3) Silent Fc: Elimination of Fc effector functions aims to extend the half-life, thereby enabling once-monthly (Q4W) dosing from the initiation of therapy. The clinical significance of this feature should not be overlooked—currently approved BCMA bispecific antibodies generally require weekly or biweekly administration; a monthly formulation represents a substantial improvement in patient convenience and accessibility in community clinics.
AbbVie has preliminarily validated this design in the combined Phase 1/1b data: ORR 66%, Grade 3/4 infection rate 23%, and CRS rate 30% (Grade 1: 26%, Grade 2: 4%, with no Grade ≥3 events). Notably, these combined data were derived from Arm A, which utilized a single step-up dose (SUD).
MONVISO Study Design: Four-Arm Parallel Design. MONVISO (NCT05650632) is a multicenter, open-label Phase 1b study with four parallel cohorts. 1) Arm A: ≥3 prior lines of therapy, BCMA-naïve, 1 step-up dose (SUD) → 60 mg Q4W, primarily for dose confirmation; 2) Arm B: Prior exposure to BCMA-directed CAR-T or ADC, no SUD, direct administration of 60 mg; 3) Arm C: ≥2 prior lines of therapy, 1 SUD → 60 mg Q4W, outpatient setting, primarily to assess outpatient feasibility; 4) Arm D: 1–3 prior lines of therapy (community setting), 1 SUD → 60 mg Q4W, outpatient setting,Primarily used to confirm community accessibility
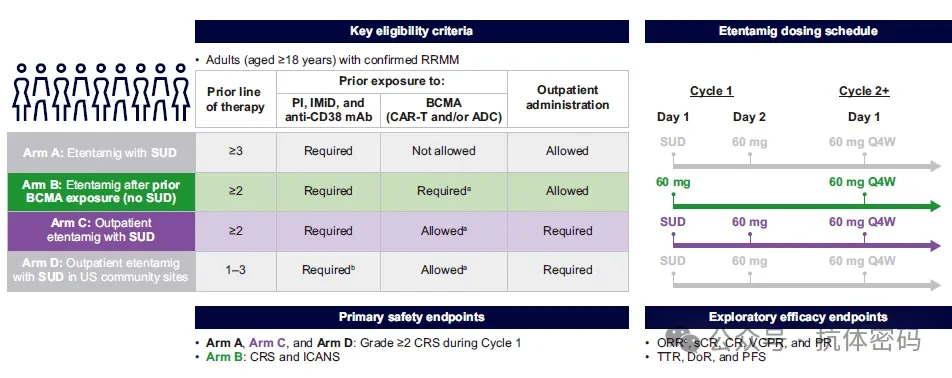
Arm B (Post-BCMA Cohort) and Arm C (Outpatient Cohort)This was the highlight announced at this year’s EHA. Arm B did not permit step-up dosing (SUD), initiating directly at 60 mg; therefore, cytokine release syndrome (CRS) was expected to be relatively high, but this also provided a baseline control for subsequent SUD optimization and tocilizumab prophylaxis strategies.
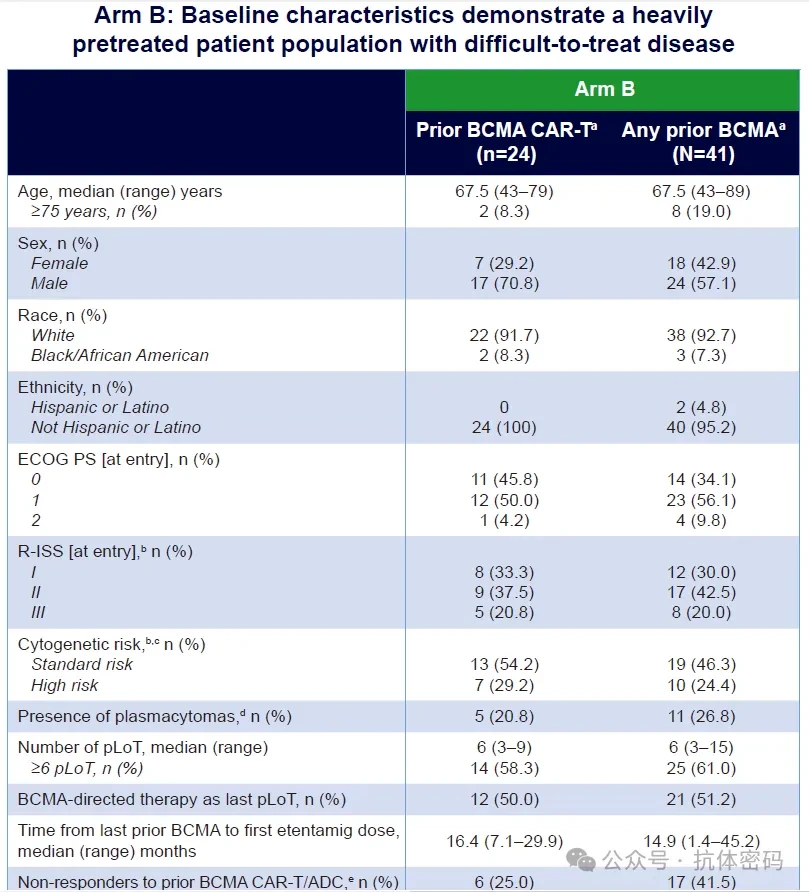
Arm B Baseline: Previously received an average of 6 lines of therapy; 60% were non-responders to BCMA-targeted therapy
Arm B enrolled a total of 42 patients, of whom 41 had a history of BCMA-targeted therapy (24 received CAR-T cell therapy and 17 received ADC therapy). The median number of prior lines of therapy was 6 (range: 3–15), with 61.0% of patients having received ≥6 prior lines of therapy; 41.5% were refractory to prior BCMA-targeted therapy (failed to achieve a response of PR or better); the median time from the last BCMA-targeted therapy to the first dose of etentamig was 14.9 months. BCMA-targeted therapy was the most recent prior line of treatment for 51.2% of patients. High-risk cytogenetics were present in 24.4% of patients, and 20.0% had R-ISS stage III disease.
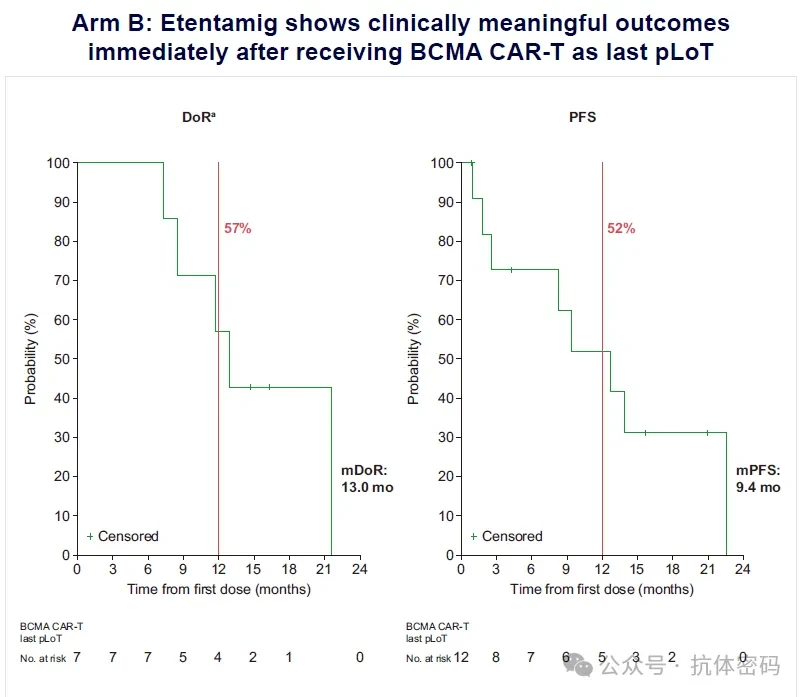
Efficacy of Arm B: Immediate administration following BCMA CAR-T failure, with an ORR of 64%.Efficacy data are presented stratified by prior BCMA exposure background: 1) Any prior BCMA exposure (n=37): ORR 64%, ≥VGPR rate 43%, ≥CR rate 22%; 2) Prior BCMA CAR-T therapy (n=23): ORR 48%, ≥CR rate 26%; 3) BCMA CAR-T as last-line therapy (n=11): ORR64%, ≥CR rate46%—This is the subgroup most worthy of attention.The median time to first response was 1.0 month (range: 0.7–4.6), consistent with the typical onset of action for TCE.
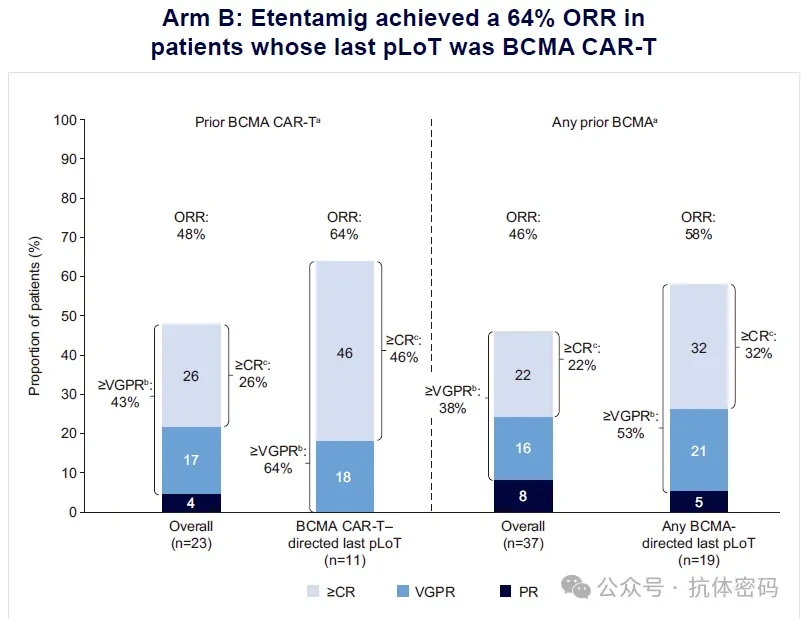
In the subgroup receiving BCMA CAR-T as last-line therapy, the median duration of response (DOR) was 13.0 months, and the median progression-free survival (PFS) was 12.7 months. At the data cutoff, 5 patients (11.9%) were still receiving study treatment.
Here are several noteworthy signals:
1)After BCMA CAR-T FailureImmediatelyUse of etentamig (i.e., last-line therapy being BCMA CAR-T) resulted in a higher ORR than that in the overall BCMA CAR-T–pretreated population (64% vs 48%).. Possible explanations include: a short washout period between late-line BCMA CAR-T therapy and etentamig, with tumor cells retaining some level of BCMA expression; or patients who experienced CAR-T expansion failure ("non-engrafters") still having a favorable window for response to subsequent T-cell engagers. The specific mechanisms require validation through larger sample sizes and biomarker analyses.
2) Even in the 41.5% of patients who did not respond to prior BCMA-directed therapy, etentamig was still able to induce remission, indicating that the mechanism of resistance to BCMA-targeted therapy is not simply "BCMA target depletion." The avidity advantage of bivalent BCMA design may play a role in this.
3) The median PFS was approximately 13 months; in patients who had received ≥6 prior lines of therapy, this figure provides a valuable time window for planning subsequent lines of treatment.
Arm B Safety: CRS Baseline Without SUD
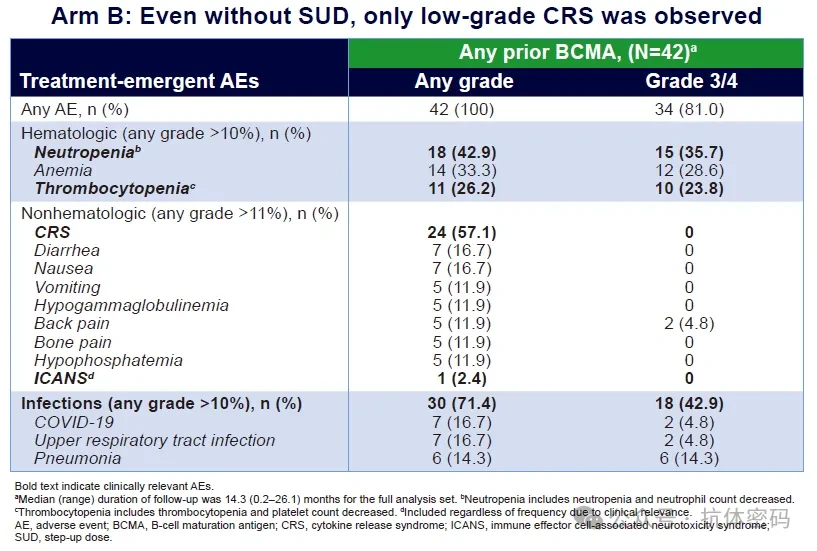
Even under the "worst-case" scenario without steroid use, all CRS events were limited to grades 1–2. The grade 3/4 infection rate of 42.9% falls within the expected range for patients with late-stage relapsed/refractory multiple myeloma (RRMM). Compared with the pivotal studies of approved BCMA-directed bispecific antibodies, this safety profile is within a reasonable range.
- CRS: 57.1% (all Grade 1–2, no Grade ≥3 events)
- Infection: 71.4% (all grades), 42.9% (grades 3/4)
- Grade 3/4 cytopenia: neutropenia 35.7%, anemia 28.6%, thrombocytopenia 23.8%
- ICANS (Immune Effector Cell-Associated Neurotoxicity Syndrome): 1 case (2.4%), Grade 2
- Discontinuation due to AE: 2 cases (pneumonia, immune effector cell-associated HLH-like syndrome)
- Fatal AEs: 3 cases (HLH-like syndrome, sepsis, pneumonia)
Arm C Outpatient Cohort: Tocilizumab Prophylaxis Achieved 0% CRS
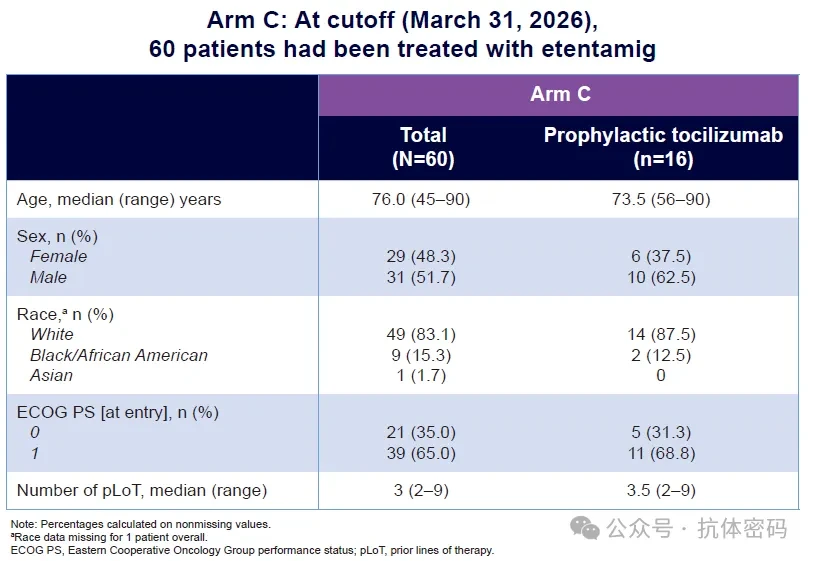
If the data from Arm B demonstrated the “upper limit” of etentamig’s safety profile, then the outpatient administration data from Arm C revealed its optimized real-world potential. Arm C enrolled 60 patients, with a median age of 76 years (range: 45–90), who received a single dose of SUD plus modified dexamethasone premedication in an outpatient setting:
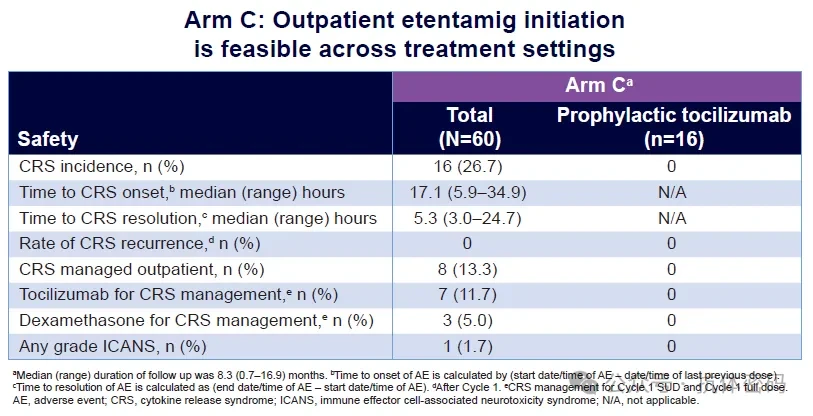
Overall CRS rate: 26.7% (all Grade 1–2); Median time to CRS onset: 17.1 hours post-SUD; Median time to CRS resolution: 5.3 hours; CRS recurrence after C1: 0%; Outpatient management of CRS: 13.3% (8 cases); ICANS: 1.7% (1 case, Grade 2)
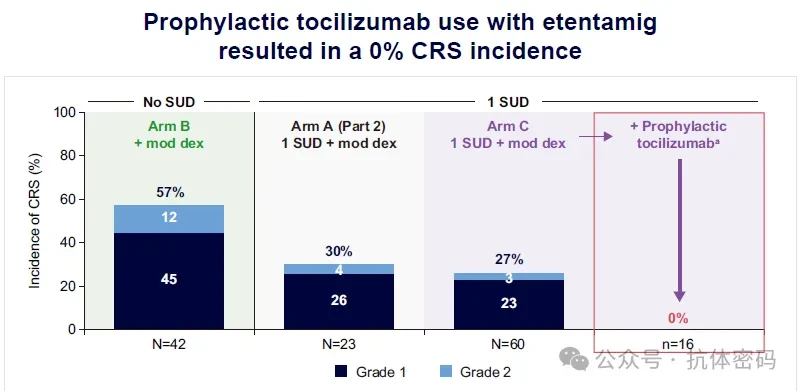
More importantly,Tocilizumab Prophylaxis Subgroup(n=16): Among patients receiving prophylactic tocilizumab, the incidence of CRS was0%, the incidence of ICANS was also 0%.
The quality of these results must be evaluated within the context of clinical practice: a median age of 76 years, entirely outpatient administration, and a median CRS resolution time of only 5.3 hours—these figures collectively underscore the feasibility of deploying etentamig in community clinic settings. One of the major barriers to the widespread adoption of BCMA bispecific antibodies is the reliance on inpatient resources for CRS management. The 0% CRS prophylaxis regimen and the rapid resolution profile of CRS directly address this critical challenge.
The CRS rate declined from 57% in Arm B (no SUD) to 30% in Arm A (1 SUD), then to 27% in Arm C (1 SUD + modified dex), and finally to 0% in Arm C + tocilizumab; this downward trend itself constitutes a comprehensive validation of the CRS mitigation strategy.
Clinical Positioning and Future Directions
The current positioning of Etentamig in the MM field encompasses two dimensions:
1) InPost-BCMA SequencingDimension: A 64% overall response rate (ORR) in the heavily pretreated BCMA CAR-T subgroup suggests that etentamig has the potential to fill the therapeutic gap following BCMA CAR-T failure. This data forms an interesting parallel with cevostamab (FcRH5×CD3), which demonstrated a 43.9% ORR in the CAMMA 2 trial among patients who had failed prior BCMA CAR-T therapy. The two targets, BCMA and FcRH5, appear to have distinct efficacy niches in the post-BCMA CAR-T setting, making subsequent head-to-head comparisons or sequential study designs critical.
InAccessibilityDimensions: Q4W formulation + 0% CRS prophylaxis regimen + outpatient management. This combination addresses the three core bottlenecks in promoting bispecific antibodies from academic centers to community clinics: dosing frequency, CRS management burden, and inpatient resource requirements. AbbVie has announced the expansion of the Q4W + 1 SUD regimen to all clinical trials of etentamig in multiple myeloma (MM) and amyloidosis.
Two Questions to Be AnsweredFirst, the sample size of the last-line subgroup receiving BCMA CAR-T therapy in Arm B was only 11 patients; the observed 64% overall response rate (ORR) needs to be validated in larger prospective cohorts. Second, regarding the long-term impact of tocilizumab prophylaxis—specifically, whether it might impair the anti-tumor immune memory mediated by T-cell engagers—Johnson & Johnson’s research has already provided an answer: it essentially has no such effect.Has Johnson & Johnson Found the Key to Mitigating CRS Risk with TCE Bispecific Antibodies?》。
Summary
Key data for Etentamig in MONVISO can be summarized into three points:
1) Post-BCMA CAR-T Window: Immediate use after BCMA CAR-T failure, with an ORR of 64% and a median PFS of 12.7 months. The BCMA target remains druggable after CAR-T failure, and the bivalent BCMA design may be a key factor.
2) A Realistic Path to 0% CRS: 1 SUD + tocilizumab prophylaxis = 0% CRS rate. Median time to response of 5.3 hours and zero relapses support the feasibility of outpatient administration.
3)Convenience Basis of Monthly Formulations: The silent Fc tail design enables Q4W as the initial regimen, aligning with the follow-up rhythm of community clinics and reducing the burden on patients and the healthcare system.

Click "Pharmadex" below”, follow for more exciting content
Disclaimer
The WeChat Official Account push rules have been changed yet again. If you don’t click"Like"Or not set to"Starred"Otherwise, we might just fade into the vast sea of literature~ Click here to stay updated with the latest news from Pharmadule! ???