In the clinical treatment of relapsed/refractory multiple myeloma (RR/MM), a variety of therapeutic agents are available, ranging from small molecules to monoclonal antibodies, bispecific antibodies, antibody-drug conjugates (ADCs), and CAR-T cell therapies. Among large-molecule therapeutics, the primary targets are BCMA, GPRC5D, and CD38. The development of BCMA-targeted therapies is relatively mature, with three bispecific antibodies, one ADC, and four CAR-T therapies currently approved for market launch. As a leader in the field of multiple myeloma (MM), Johnson & Johnson has covered the entire spectrum of MM treatment—from first-line to last-line therapy—and has developed bispecific antibody combination regimens as well as trivalent T-cell engagers (TCEs), achieving favorable efficacy. Roche, as the leading player in the bispecific antibody space, has a relatively limited portfolio in MM, with only an FcRH5-targeting TCE.CevostamabIn clinical practice,Cevostamab’s preclinical data were disclosed long ago, but its clinical development has progressed relatively slowly, with Phase III trials only commencing this year.
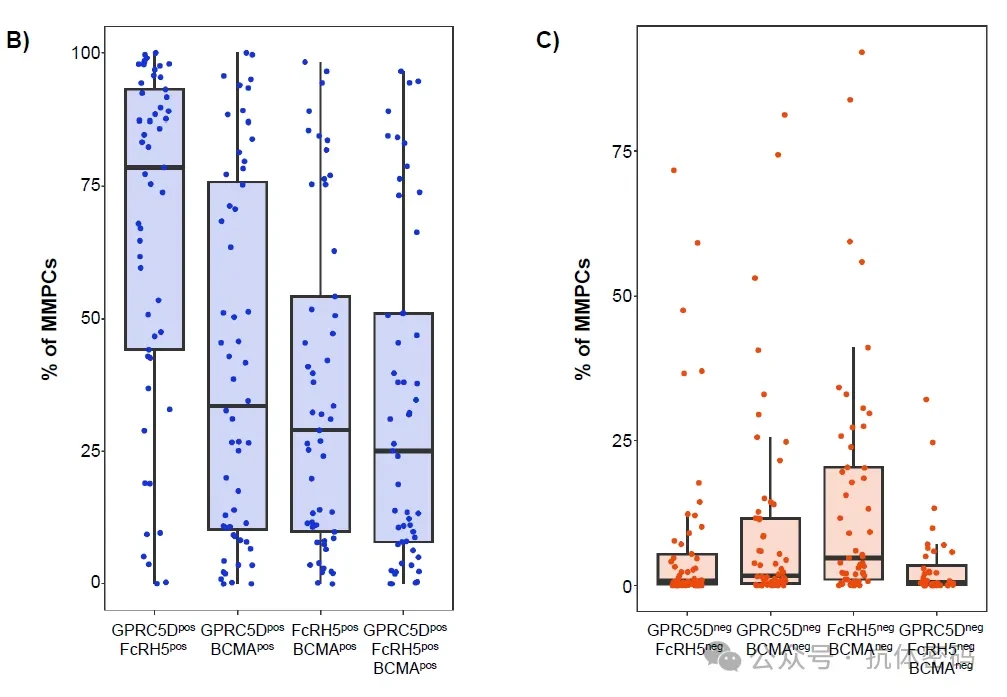
FcRH5 is a relatively novel multiple myeloma (MM) target: it is specifically expressed in the B-cell lineage, and its expression on MM cells is independent of BCMA status—making it independently valuable in post-BCMA line therapies. Previous Roche studies evaluated the baseline expression of GPRC5D, FcRH5, and BCMA on MM plasma cells (MMPCs). In terms of positivity rates (left panel),GPRC5D (median 95.7%) and FcRH5 (88.1%) were extremely high, significantly superior to BCMA (45.6%).Regarding receptor density (right panel), the expression level of GPRC5D (median 20,612 MESF) far exceeded that of FcRH5 (512) and BCMA (259).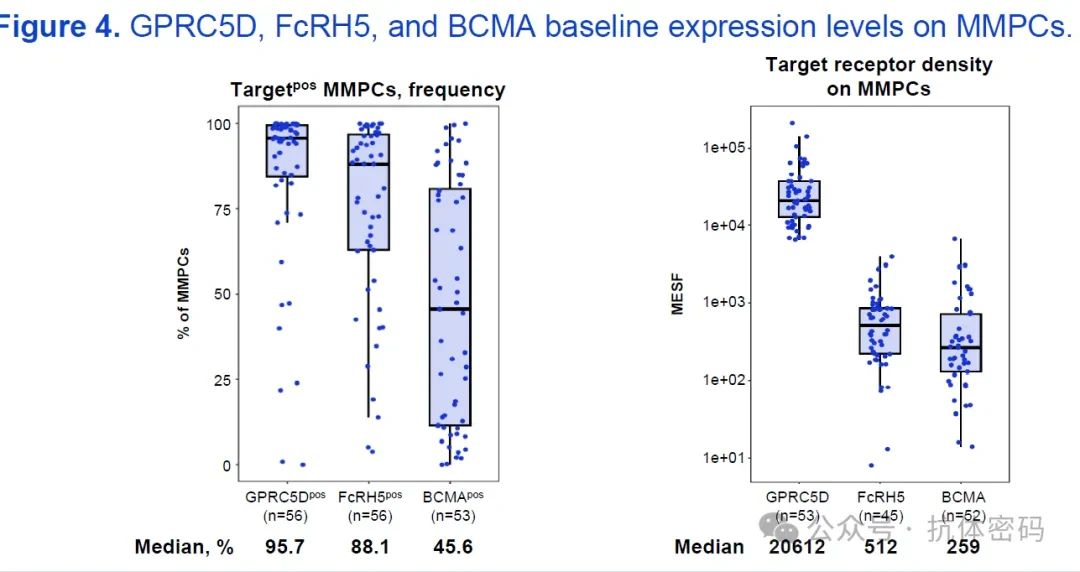
In terms of target expression,GPRC5D⁺FcRH5⁺ (~80%) and GPRC5D⁺BCMA⁺ (~60%) MMPCs account for a relatively high proportion, while the proportion of FcRH5⁺BCMA⁺ is relatively low (~50%).。Proportion of Double-Negative Cells:FcRH5⁻BCMA⁻MMPCs accounted for the highest proportion (~20%), with the remainder being double-negative (e.g., GPRC5D⁻FcRH5⁻,GPRC5D⁻BCMA⁻) Extremely low proportion (<10%).
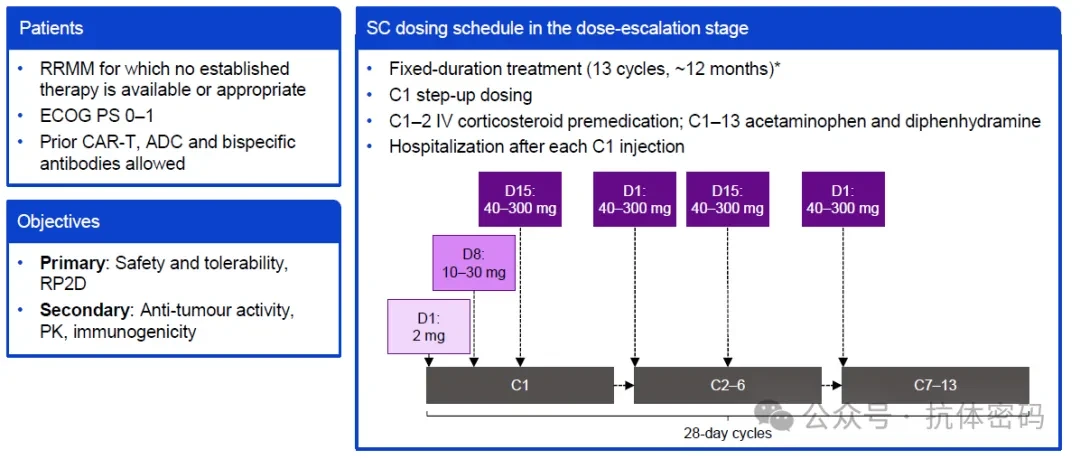
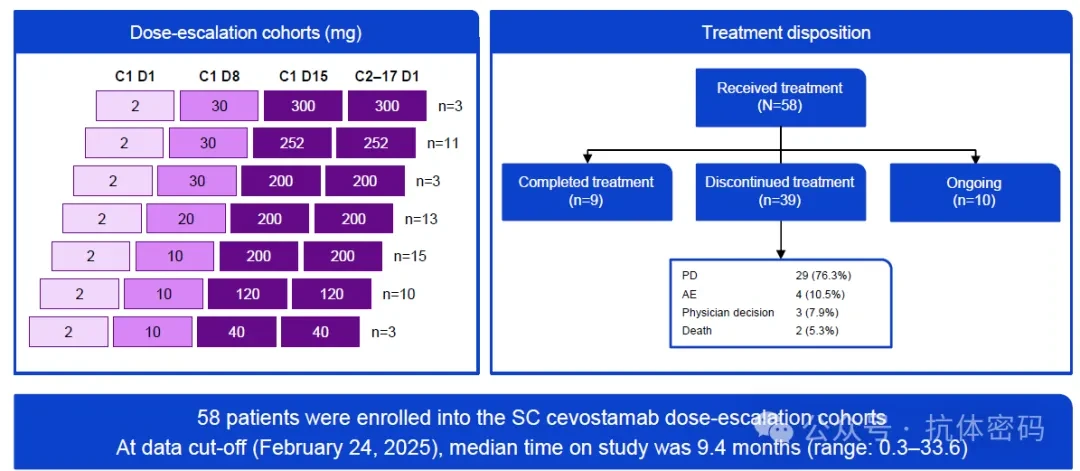
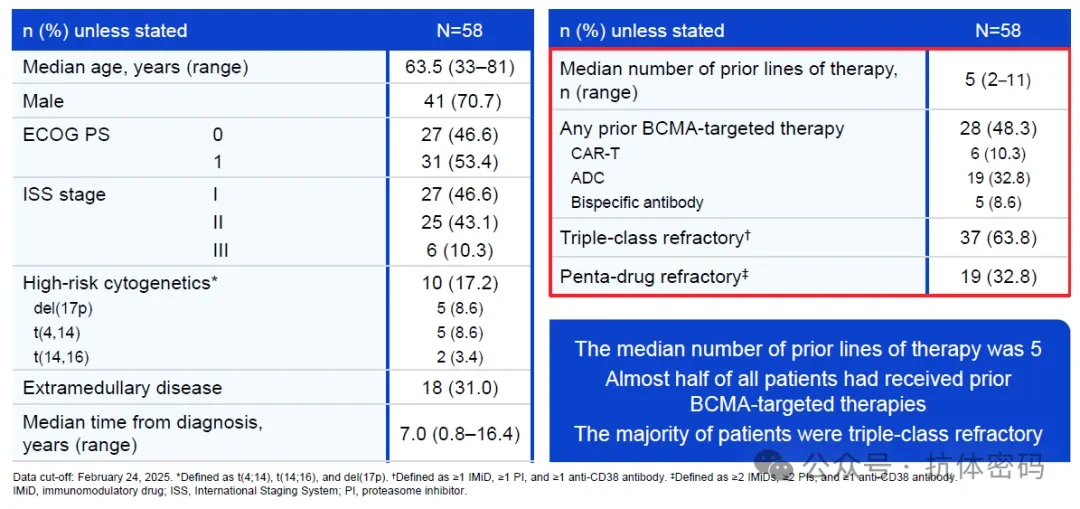
At last year's ASH meeting, Roche announcedClinical Data of Cevostamab,CAMMA 3 is a Phase Ib study targeting patients with relapsed/refractory multiple myeloma (RRMM) who have no standard treatment options, an ECOG performance status of 0-1, and prior exposure to CAR-T therapy, antibody-drug conjugates (ADCs), and bispecific antibodies is permitted.The subcutaneous (SC) dosing regimen employs a fixed course of 13 cycles (approximately 12 months). Cycle 1 (C1) utilizes a three-step dose escalation to mitigate the risk of cytokine release syndrome (CRS): 2 mg on Day 1 (D1), 10–30 mg on D8, and 40–300 mg (target dose) on D15. From Cycle 2 (C2) onward, the target dose is administered once per cycle. Intravenous (IV) corticosteroids are given as premedication prior to injections in C1–C2, while acetaminophen and diphenhydramine are administered throughout the treatment course. Hospitalization for observation is required after each injection in C1.Patient Characteristics: Heavily pretreated, with nearly half having previously received BCMA-targeted therapy. Among the 58 patients, the median age was 63.5 years, and the median number of prior lines of therapy was 5 (range, 2–11).
- 63.8% were classified as Class III refractory(triple-class refractory, refractory to IMiDs, PIs, and anti-CD38 monoclonal antibodies)
- 32.8% were refractory to five drugs(penta-drug refractory)
- 48.3% had previously received BCMA-targeted therapy(CAR-T 10.3%, ADC 32.8%, bispecific antibodies 8.6%)
Efficacy: ORR 52% and MRD negativity rate 80% in BCMA-naïve patients
Efficacy analysis was based on 52 evaluable patients, pooled across all patients receiving a target dose of ≥120 mg.The ORR and VGPR+ rate in BCMA-naïve patients were both 52.0%., forming a clear stratification compared to BCMA-exposed patients (ORR 25.0%)—the disparity primarily stems from the proportion of patients achieving deep responses of VGPR or better (52.0% vs. 8.3%).
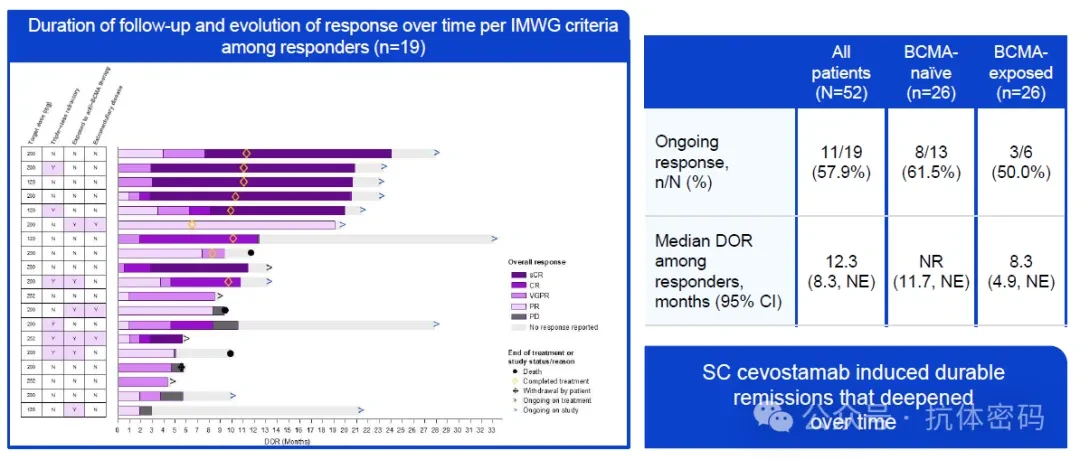
Among 10 evaluable patients with CR+ for MRD,8 cases (80%) achieved MRD negativity at the 10⁻⁵ level. Achieving MRD negativity typically requires a deep response, and this proportion holds clinical significance in later-line multiple myeloma.Duration of Response: Response deepened over time; median DOR not reached in BCMA-naïve patients
Among the 19 responders, 57.9% maintained remission (as of the data cutoff). Stratified median duration of response (DOR): 12.3 months for all responders (95% CI: 8.3–NE), 8.3 months for BCMA-exposed patients (95% CI: 4.9–NE), and median DOR not reached for BCMA-naïve patients (95% CI: 11.7–NE).
The trend of deepening response over time is also well-documented: multiple patients upgraded from PR/VGPR to CR/sCR during subsequent follow-up after initial response.
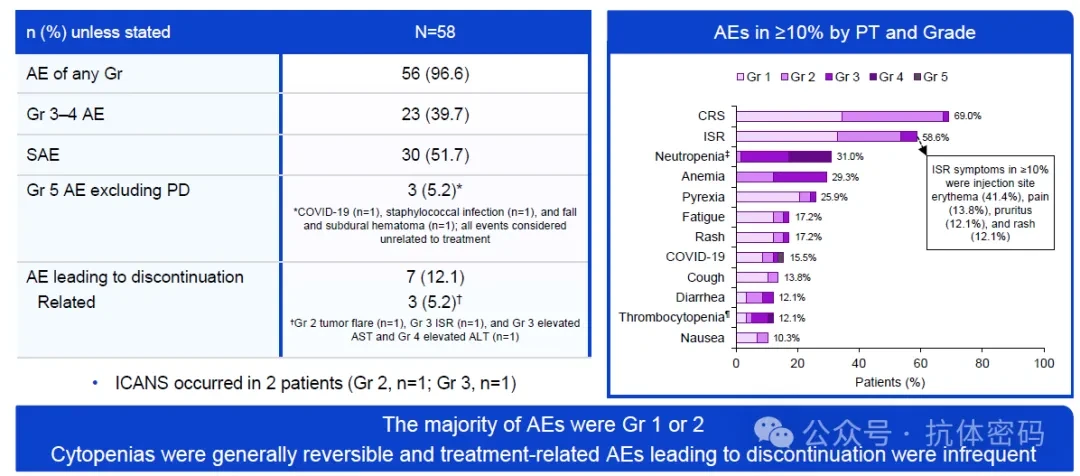
Safety: AEs were predominantly Grade 1–2, CRS was manageable, and ISR was the trade-off for subcutaneous administration.
Among AEs with an incidence rate ≥10%,Injection site reactions (ISR) had the highest incidence, at 69.0%.—These are the main adverse events newly observed with subcutaneous (SC) administration compared to intravenous (IV) administration. Injection site reactions (ISRs) were predominantly characterized by erythema (41.4%), pain (13.8%), pruritus (12.1%), and rash (12.1%), the vast majority of which were low-grade. The incidence of cytokine release syndrome (CRS) was 58.6%, neutropenia 31.0%, anemia 25.9%, and thrombocytopenia 29.3%; these events were primarily Grade 1–2 in severity, and cytopenias were reversible.CRS Management: All cases occurred in C1, with complete resolution
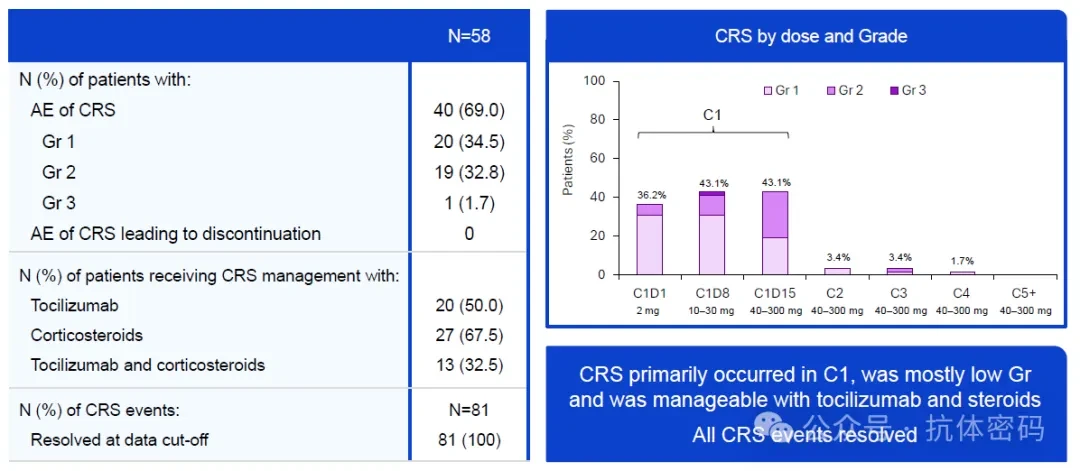
Cytokine release syndrome (CRS) is the most closely monitored safety event associated with T-cell-engaging bispecific antibodies and represents one of the core design objectives of the CAMMA three-step dose-escalation regimen.
All 81 CRS events resolved completely (100%). In terms of distribution, CRS primarily occurred during the step-up dosing phase of Cycle 1, with incidence rates of 43.1% on both C1D8 (10–30 mg) and C1D15 (40–300 mg). From Cycle 2 onwards, the incidence of CRS rapidly decreased to approximately 3%.No cases of CRS led to discontinuation.
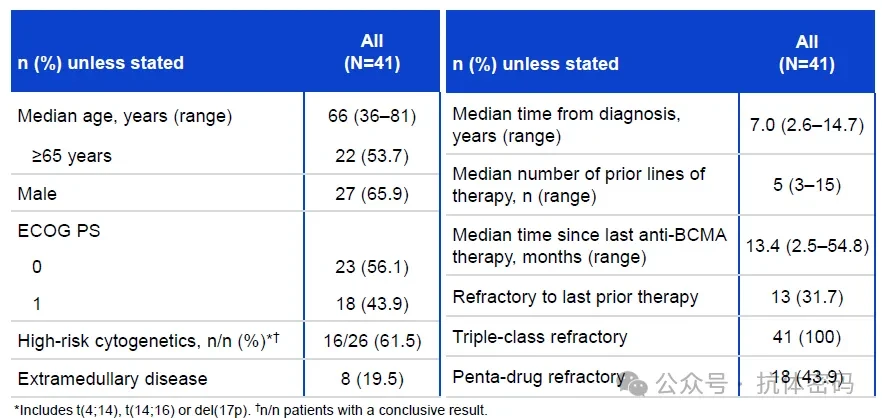
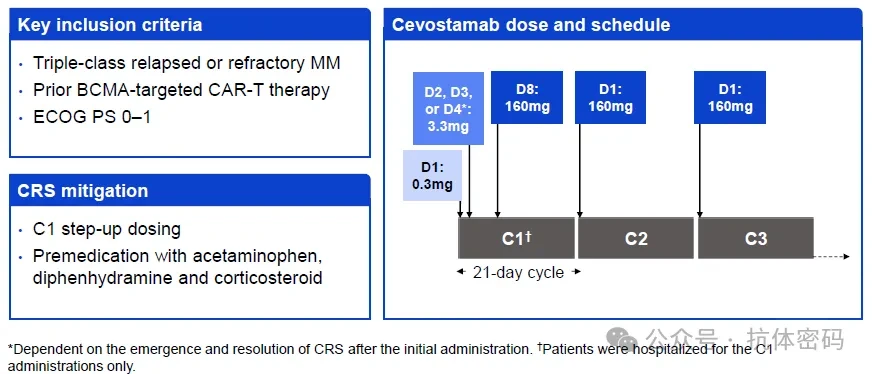
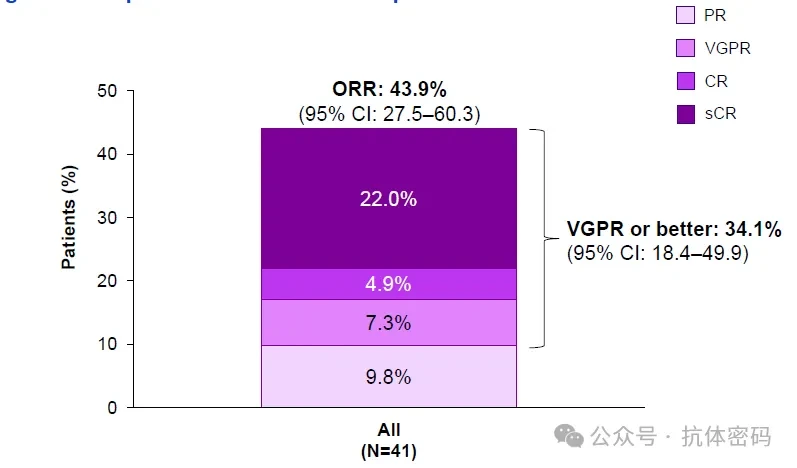
At this year's EHA Congress,Roche's latest clinical (CAMMA 2) Results demonstrateCevostamab inDemonstrated favorable efficacy in patients with triple-refractory disease (refractory to three drug classes: proteasome inhibitors, immunomodulatory agents, and CD38 monoclonal antibodies) and prior BCMA CAR-T failure, achieving a response rate of ≥VGPR of 34.1% and an overall response rate (ORR) of 43.9%.
CAMMA 2 enrolled 41 patients with relapsed/refractory multiple myeloma (RRMM) who had received BCMA-targeted CAR-T therapy, representing a highly challenging patient population. The patients had previously received an average ofPreviously treated with five lines of therapy, 100% triple-refractory, and over 60% with high-risk cytogenetic abnormalities.
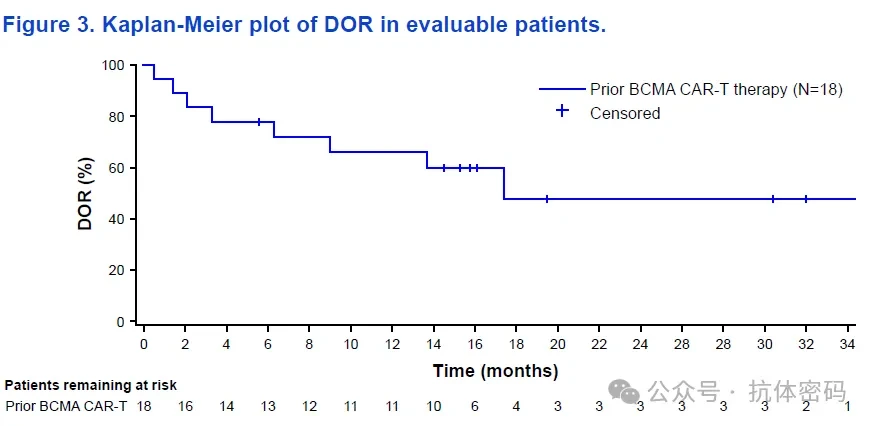
The study employed a step-up dosing regimen (C1 D1: 0.3 mg → D2–4: 3.3 mg → D8: 160 mg), followed by maintenance of the target dose of 160 mg every 3 weeks until disease progression or unacceptable toxicity.Efficacy: Among evaluable patients, cevostamab monotherapy achieved an objective response rate (ORR) of 43.9% (95% CI: 27.5–60.3), with a rate of very good partial response (VGPR) or better of 34.1%.Monotherapy after BCMA CAR-T failure has historically demonstrated an objective response rate (ORR) of less than 20%. Although an ORR of 43.9% does not reach the level of first-line therapy, it represents a significant signal of activity in this heavily refractory population.. Furthermore, the 34.1% rate of very good partial response (VGPR) or better indicates that the depth of response was not limited to partial response (PR) alone, with a certain proportion of patients achieving deeper responses.Median Duration of Response (DOR) was 17.4 months(95% CI: 9.0–not estimable); at the data cutoff, 44.4% (8/18) of responders remained in ongoing response. The 15-month DOR rate was 59.8% (95% CI: 36.7–83.0).
A median DOR of 17.4 months is a competitive figure for single-agent therapy in late-stage RRMM, especially considering that all patients were triple-refractory and had failed prior BCMA CAR-T therapy.
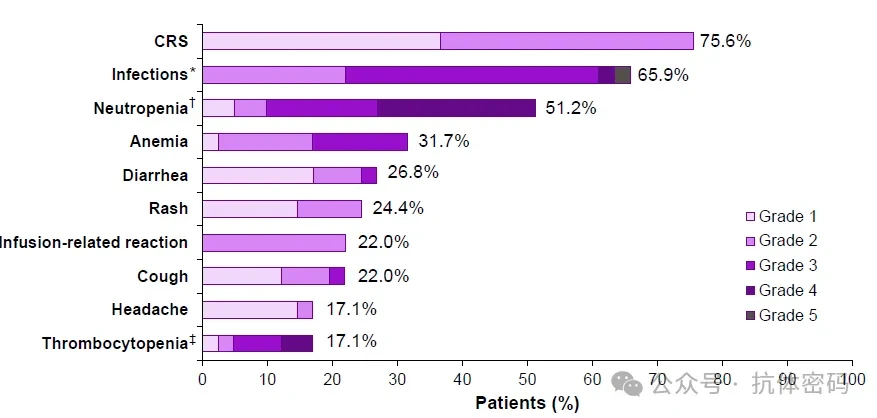
Safety: All CRS cases were grade 1–2, with infection and cytopenia being the most common:CRS: All events were Grade 1-2, with 76.9% of CRS events occurring within 24 hours after the end of infusion.51.6% of CRS events were managed with tocilizumab, and 51.6% were managed with corticosteroids; all events had resolved by the data cutoff date.Only one patient discontinued cevostamab due to an AE (Grade 5 MDS, determined to be unrelated to cevostamab). Both Grade 5 AEs (pneumonitis and MDS) were determined to be unrelated to cevostamab.Antigen Expression Profile: High FcRH5 Expression, Low BCMA Expression
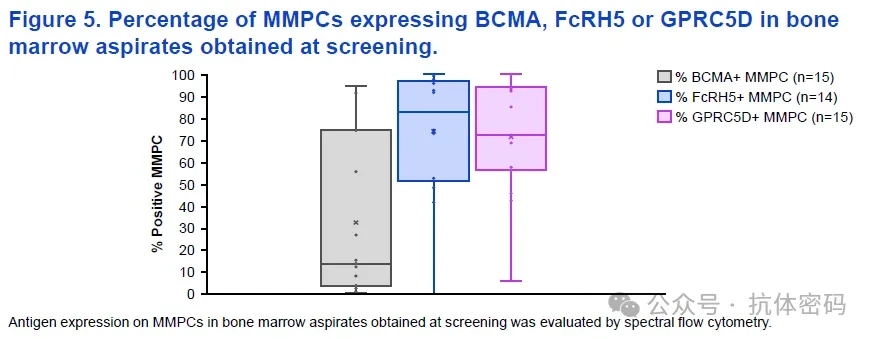
The researchers used spectral flow cytometry to detect the antigen expression of MM plasma cells (MMPC) in baseline bone marrow aspiration samples from 15 patients.1) Following treatment with BCMA CAR-T or BCMA ADCs, BCMA expression on tumor cells is significantly downregulated, which explains the limited efficacy of retreatment with BCMA-targeted agents after failure of initial BCMA-targeted therapy; 2) FcRH5 remains highly expressed in tumor cells from the vast majority of patients, providing broad target coverage for cevostamab; 3) GPRC5D is also highly expressed, which explains why GPRC5D×CD3 bispecific antibodies (such as talquetamab) represent a rational subsequent option after failure of BCMA CAR-T therapy.
 Current Landscape of Later-Line Therapies for RRMM: Bispecific antibodies targeting BCMA and GPRC5D represent the most accessible options following CAR-T cell therapy failure. Johnson & Johnson is the undisputed leader in this field, with a portfolio encompassing not only bispecific antibodies but also bispecific antibody-based combination therapies and trispecific antibodies. As a pioneer in the bispecific antibody space, Roche has opted to target novel antigens rather than engage in direct competition with Johnson & Johnson.FcRH5 and developed TCE bispecific antibodyCevostamab。In clinical practice, Cevostamab atThe ORR and VGPR+ rate in BCMA-naïve patients were both 52.0% (≥120 mg), and in monotherapy, among patients who have developed resistance after receiving BCMA CAR-T therapy,The ORR still reached 43.9%, and34.1% of patients achievedResponse of VGPR or better, which demonstratescevostamabHolds considerable potential as a later-line treatment.Additionally,FcRH5 remains highly expressed after BCMA-targeted therapy, providing direct evidence for the positioning of cevostamab in BCMA-independent targeting strategies.Of course, Roche’s ambitions are not limited to late-stage therapies,CAMMA 1 Arm B (Data of cevostamab + pom-dex in BCMA treatment-naïve patients), with the high-dose group achieving a CR rate of 60% for cevostamab,VGPR+ Achieved76.0%, which also proves itsPotential application scenarios may cover both BCMA treatment-naïve and BCMA pre-treated populations.
Current Landscape of Later-Line Therapies for RRMM: Bispecific antibodies targeting BCMA and GPRC5D represent the most accessible options following CAR-T cell therapy failure. Johnson & Johnson is the undisputed leader in this field, with a portfolio encompassing not only bispecific antibodies but also bispecific antibody-based combination therapies and trispecific antibodies. As a pioneer in the bispecific antibody space, Roche has opted to target novel antigens rather than engage in direct competition with Johnson & Johnson.FcRH5 and developed TCE bispecific antibodyCevostamab。In clinical practice, Cevostamab atThe ORR and VGPR+ rate in BCMA-naïve patients were both 52.0% (≥120 mg), and in monotherapy, among patients who have developed resistance after receiving BCMA CAR-T therapy,The ORR still reached 43.9%, and34.1% of patients achievedResponse of VGPR or better, which demonstratescevostamabHolds considerable potential as a later-line treatment.Additionally,FcRH5 remains highly expressed after BCMA-targeted therapy, providing direct evidence for the positioning of cevostamab in BCMA-independent targeting strategies.Of course, Roche’s ambitions are not limited to late-stage therapies,CAMMA 1 Arm B (Data of cevostamab + pom-dex in BCMA treatment-naïve patients), with the high-dose group achieving a CR rate of 60% for cevostamab,VGPR+ Achieved76.0%, which also proves itsPotential application scenarios may cover both BCMA treatment-naïve and BCMA pre-treated populations.
PharmaDJ Media Business CooperationMedia Relations | News &Press ReleaseManager Zhang: 18600036371 (WeChat ID same as phone number)Click "Pharmadl" below”, for more exciting content
“Yao Du” Official Account: This article was reposted from another WeChat official account platform, primarily for the purpose of sharing industry-related knowledge and disseminating the latest information. The copyrights of all images and articles belong to their original authors. If there is any infringement, please inform us promptly, and we will remove the relevant content within 24 hours.The WeChat Official Account’s push notification rules have changed yet again. If you don’t click"Watching"Or not set to"Starred", we might just fade into the vast sea of articles~ Click here to stay updated with the latest news from Pharmadule! ???