INL1 (Trientine Hydrochloride) Shows Promise in Filling Treatment Gap for Heart Failure with Reduced Ejection Fraction, Says MedPage Today
Following the release of Innolife’s new heart failure drug INL1 (trientine hydrochloride) at the 2023 European Society of Cardiology Heart Failure Congress (ESC-HF 2023), where it was recognized as one of the “Top 10 Most Anticipated Breakthrough Studies of 2023.”
On the morning of October 9 (U.S. local time), at Massachusetts General Hospital, Harvard University, Professor James L. Januzzi, a Council Member of the American College of Cardiology, presented the analysis results of INL1 (trientine hydrochloride) in patients with heart failure with severely reduced ejection fraction during the “Focus on Key Clinical Science” session of the Plenary Session at the 2023 Heart Failure Society of America (HFSA 2023) Annual Meeting. The presentation drew significant attention from the international medical community, prompting the prominent U.S. medical publication Medical News Today to feature a cover article on the findings.
The article commented: “This drug has demonstrated favorable safety and promising therapeutic prospects in patients with heart failure with reduced ejection fraction, holding the potential to reverse cardiac remodeling. In particular, it addresses an unmet therapeutic need, as the application of existing medications is often limited by their tendency to cause hypotension.”

HFA 2023 Cleveland, USA
The 2023 Annual Meeting of the Heart Failure Society of America (HFSA) was recently held in Cleveland, USA, where the results of the TRACER-HF study analysis in patients with heart failure with severely reduced ejection fraction were released. The use of a lower dose of INL1 (trientine hydrochloride) demonstrated favorable safety and promising therapeutic prospects for patients with heart failure with severely reduced ejection fraction.
In the full analysis set, the twice-daily 300 mg dose significantly improved NT-proBNP levels compared with placebo at weeks 4 and 8 (geometric least squares mean ratios: 0.82 vs. 1.03, P=0.05; and 0.79 vs. 1.02, P=0.03). However, as previously reported, the study did not demonstrate a benefit on the primary endpoint at week 12 (P=0.99).
“The 12-week duration of this study coincided precisely with the peak of the COVID-19 pandemic in China, by which time most patients had already been enrolled. The pandemic affected follow-up for these patients and may have influenced the assessment of differences in efficacy at the 12-week follow-up,” noted Professor James L. Januzzi of Massachusetts General Hospital and Harvard Medical School.

Professor James L. Januzzi, Massachusetts General Hospital, Harvard University
At the Heart Failure Society of America (HFSA) meeting, Professor James L. Januzzi presented an analysis of the interaction between left ventricular ejection fraction (LVEF) and the significance of treatment efficacy. Among 101 patients with an LVEF of 30% or lower, the reduction in the primary endpoint, NT-proBNP levels, showed statistically significant differences at all three follow-up time points, including at 12 weeks.
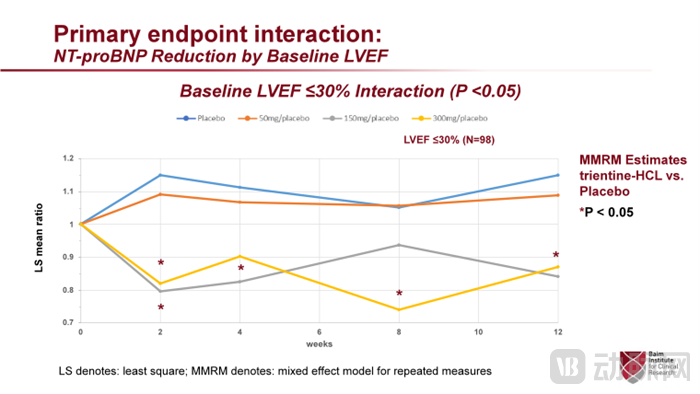
Primary Endpoint: Significant Reduction in NT-proBNP Levels
High-dose trientine hydrochloride has been used as an oral copper chelator for the treatment of Wilson’s disease (hepatolenticular degeneration) for over 40 years. Wilson’s disease is a rare genetic disorder that causes copper accumulation in organs. However, at low doses, trientine hydrochloride (INL1) can act as a copper carrier to restore normal intracellular copper levels.
Professor James L. Januzzi pointed out that copper plays a critical role in the myocardium, such as serving as a cofactor for ATP generation and calcium channels. He stated, “Although clinical copper deficiency is quite rare, it has been confirmed to be associated with an increased risk of non-ischemic cardiomyopathy. Even under normal circulating copper concentrations, intracellular copper depletion is linked to myocardial remodeling and reduced ejection fraction. Conversely, experimental restoration of normal intracellular copper levels can reverse this process and improve ejection fraction.”
"In fact, what was truly striking in the Phase IIa trial was the reversal of left ventricular remodeling," he told the attendees. A significant trend toward improvement was observed in the population with a baseline LVEF of 30% or lower, whereas such trends were not seen in those with higher LVEF.

Secondary Endpoint: Left Ventricular Ejection Fraction (LVEF) Showed a Clear Trend Toward Improvement
In patients with severely reduced ejection fraction, the left ventricular ejection fraction (LVEF) improved by 3.4% in the 50-mg dose group, by 5.6% in the 150-mg dose group, and by 6.3% in the 300-mg dose group, compared with 3.1% in the placebo group. The mean absolute changes from baseline in left ventricular end-systolic volume and left ventricular end-diastolic volume showed similar trends; there were notable differences between the 300-mg dose group and the placebo group for both measures (-15.3 vs. +5.5 mL and -5.7 vs. +20.0 mL, respectively), although these trends were not statistically significant (P=0.19 and P=0.13).
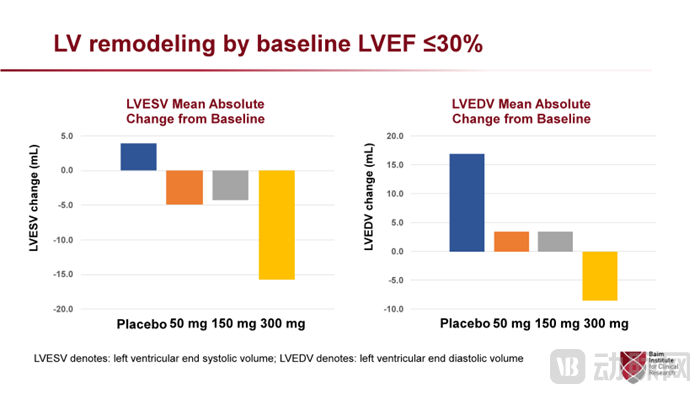
Secondary Endpoints: LVESV (Left Ventricular End-Systolic Volume) and LVEDV (Left Ventricular End-Diastolic Volume)Demonstrated an improvement trend consistent with LVEF
The highest-dose group also demonstrated a significant improvement in quality of life within 12 weeks, with the Kansas City Cardiomyopathy Questionnaire score increasing by an average of 11 points (P=0.009 vs. baseline), whereas the placebo group lost 0.9 points over the same period. Professor James L. Januzzi noted that the improvement in six-minute walk distance was consistent.
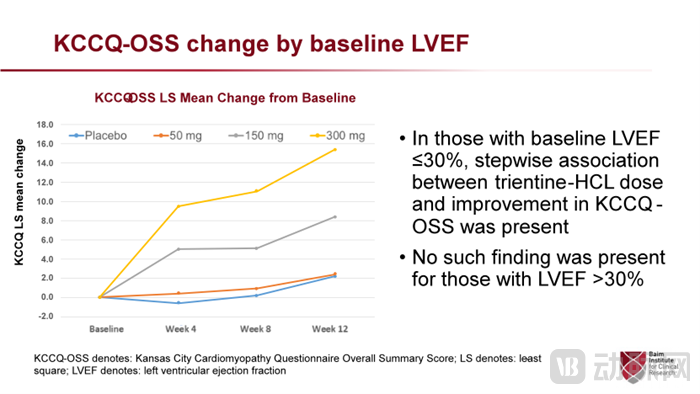
Significant Improvement in the Total Score of the Kansas City Cardiomyopathy Questionnaire
This study enrolled 190 patients (mean age 57.3 years, 20% female) in North America and China who were classified as New York Heart Association (NYHA) functional class II or III, had a left ventricular ejection fraction (LVEF) of 40% or lower, elevated NT-proBNP levels, and were receiving stable optimal medical therapy including diuretics. They were randomly assigned to receive placebo or trientine hydrochloride at doses of 300 mg, 150 mg, or 50 mg twice daily. The majority of recruitment occurred in China, with 90% of total participants being Asian. The study was initiated in December 2019, then suspended from April 2020 to January 2021 due to the COVID-19 pandemic; thereafter, recruitment efforts shifted focus to China.
Among the 101 patients with an LVEF of ≤30% and the 89 patients with an LVEF of 31–40%, there were no significant differences in other baseline characteristics. Furthermore, the utilization rates of guideline-recommended heart failure medications were high, including beta-blockers in over 90% of patients, ACEIs/ARBs/ARNIs in 98% (with sacubitril/valsartan [Entresto] used by 83%), and SGLT2 inhibitors in 44%. Professor James L. Januzzi stated, “This is directly relevant to our selection of a novel therapeutic regimen for patients with severely reduced ejection fraction.” Additionally, “in the study, trientine hydrochloride (INL1) did not affect blood pressure or heart rate.”
Conference chair Harriette Van Spall, MD, MPH, Professor at McMaster University’s Hamilton campus, noted that trientine hydrochloride (INL1) has a long-standing history of favorable safety at higher doses for Wilson’s disease, and these study results herald highly promising therapeutic prospects for this drug.
Regarding unmet clinical needs, Professor Harriette Van Spall concluded: “This study provides important information for the conduct of the Phase III clinical trial of INL1 (trientine hydrochloride). If its efficacy is further confirmed in the Phase III clinical trial, this drug will fill the treatment gap for patients with heart failure with reduced ejection fraction and severely reduced ejection fraction, as existing medications often cause symptomatic hypotension, a side effect that limits their clinical application.”
Study on INL1 (Cuprizone Hydrochloride) Reversing Myocardial Remodeling in Patients with Heart Failure. This study is a global, multicenter clinical trial led by Professor James Louis Januzzi of Harvard University in the United States. Cuprizone Hydrochloride (INL1) is a first-in-class innovative drug independently developed by Innolife, based on the theory of regenerative signal regulation and core target validation. It can target the hypoxia-inducible factor (HIF-1) pathway. The discoverer of the HIF-1 target was awarded the Nobel Prize in Physiology or Medicine in 2019.
A company registered in Beijing, with Harvard University in the United States,In a collaborative effort, institutions including the National Center for Cardiovascular Diseases of the Chinese Academy of Medical Sciences have achieved a breakthrough in the therapeutic regulation of cardiac regeneration signaling, making “molecular bypass” and “myocardial regeneration” possible. Selected by the European Society of Cardiology as one of the “Top 10 Most Watched Breakthrough Studies of 2023,” this research holds the promise of redefining the standard of care for heart failure.
Reference: Crystal Phend, Contributing Editor at MedPage Today, a leading U.S. medical news outlet, October 10, 2023,《Copper-Boosting Agent Promising for Low Ejection Fraction Heart Failure— Early-phase study analysis suggests potential for remodeling》。