China's Domestic Pharma Companies Heavily Invest in the Gout and Hyperuricemia Market—A $10B+ Blue Ocean Awaiting Breakthrough Therapies After a Decade Without New Drug Approvals

Innovent
High-end Biologics Developer

Evopoint Biosciences
Biological New Drug Developer

ApicHope
Innovative Biopharmaceutical R&D Developer
When it comes to metabolic diseases, diabetes is the first condition that comes to mind. Pharmaceutical companies, medical device manufacturers, and investment institutions have poured substantial resources into this area, giving rise to a wave of innovations ranging from GLP-1 medications and continuous glucose monitoring (CGM) devices to various digital therapeutics for diabetes management. Indeed, as the most prevalent metabolic disease globally, diabetes warrants such significant investment. However, hyperuricemia and gout, the second most common metabolic disorders, have seen no new drug approvals in the past decade.
According to Frost & Sullivan data, the global number of patients with hyperuricemia and gout exceeded 1.1 billion in 2020, with China’s patient population surpassing 200 million. These figures are projected to reach 1.13 billion globally and 260 million in China by 2024, respectively. Hyperuricemia and gout are increasingly poised to join the “Three Highs” (hypertension, hyperglycemia, and hyperlipidemia) to form the “Four Highs.”
As the global patient population continues to grow, the market size for corresponding medications will also expand. Currently, gout cannot be completely cured; after the acute phase, long-term pharmacological intervention is required to inhibit uric acid production or promote its excretion, thereby lowering serum uric acid levels. However, the treatment needs of hundreds of millions of patients remain largely unmet.
The latest domestic gout medication, febuxostat, was approved for market launch in 2013, a decade ago. Moreover, nearly all currently available gout medications suffer from side effects and suboptimal efficacy.
According to the "Chinese Guidelines for the Diagnosis and Treatment of Hyperuricemia and Gout," the current first-line therapeutic agents for recurrent acute/chronic gout are xanthine oxidase inhibitors (XOIs) and urate transporter 1 (URAT1) inhibitors. Representative drugs in the former category include allopurinol, febuxostat, and topiroxostat, while those in the latter category include probenecid, benzbromarone, lesinurad, and dotinurad.
XOI drugs have long been plagued by suboptimal efficacy, with approximately 40%–60% of patients failing to achieve adequate control of uric acid levels after medication, alongside safety concerns. As early as 2017, the FDA issued a safety warning regarding febuxostat. Subsequently, in 2019, the FDA mandated the addition of a boxed warning to the drug’s labeling, highlighting an increased risk of cardiovascular death, as well as risks of gout flares, hepatotoxicity, and severe cutaneous allergic reactions.
The side effects of URAT1 inhibitors have also drawn significant criticism. For instance, probenecid increases the risk of kidney stones and renal disease; Sanofi’s benzbromarone carries severe hepatotoxicity, with reported cases of death. Consequently, the drug was withdrawn from the French market in 2003, followed by most European countries except Germany, while the FDA has never approved benzbromarone for marketing in the United States. Although lesinurad received FDA approval in 2015, its marketing authorization was revoked in 2019 due to nephrotoxicity.

Marketed Gout Medications; Data Sourced from Public Information and GF Securities Development Research Center
In the domestic market, febuxostat, allopurinol, and benzbromarone remain the primary medications for gout patients, with the most recent approval of febuxostat dating back a decade. On the global stage, apart from dotinurad, which was approved in 2020, no new agents have been introduced in either the xanthine oxidase inhibitor (XOI) or urate transporter 1 (URAT1) inhibitor classes for many years. Even dotinurad is currently available only in the Japanese market, with limited visibility, and its safety profile still requires further study and observation.
In addition to the above two common classes of drugs, there is another class of uricase agents that lower serum uric acid levels by degrading uric acid. However, these drugs are prone to inducing antibody formation during use, which limits their therapeutic efficacy in the treatment of hyperuricemia. Furthermore, this category currently lacksProductApproved for marketing in China.
Over the past two decades, improvements in living standards, changes in dietary patterns, excessive intake of high-purine foods, and disordered lifestyles have led to a continuous increase in the incidence of hyperuricemia and gout. Existing medications each present distinct efficacy and safety concerns, creating an urgent need for gout therapeutics that offer both guaranteed efficacy and safety for patients with hyperuricemia and gout.
Although the market size is not as large as that of diabetes, the long-standing unmet clinical needs of hundreds of millions of patients will create a new blue-ocean market. Any entity that achieves breakthroughs in safety and efficacy will surely be embraced by the market.
At the 2023 American College of Rheumatology (ACR) Annual Meeting held on November 10, Arthrosi Therapeutics, in which ApicHope holds a stake, announced the latest research progress on its gout treatment drug, creating a ripple on the water’s surface that had remained undisturbed for many years.
Although the current ACR guidelines for gout management recommend a target serum uric acid (SU) level of <6 mg/dL, which must be maintained for 3 to 6 months to effectively prevent gout flares, there has long been controversy surrounding the optimal SU threshold. The latest research presented at this year’s ACR conference suggests that an SU level of <3.9 mg/dL may represent the optimal target for gout treatment.
This data analysis pooled approximately 6,183 study participants, with a median age of 65 years and a median serum uric acid (SU) level of 8.6 mg/dL. Participants were randomly assigned to receive either febuxostat or allopurinol treatment; 71% of patients achieved SU levels <6 mg/dL at 3 months, and this proportion increased over time. The group with SU levels ≥10 mg/dL consistently exhibited the highest rate of gout flares, with the shortest interval between secondary recurrences being only 3 months.
Within the first year of treatment, no significant differences were observed among groups, except for the group with sulfonylurea (SU) doses ≥10 mg/dL. However, when focusing on the period between 12 and 72 months, the incidence rate significantly increased even in the group receiving SU doses of 4.0–5.9 mg/dL compared to the group receiving ≤3.9 mg/dL.
In other words, to achieve long-term therapeutic efficacy, serum uric acid (SU) levels must be maintained at ≤3.9 mg/dL, which imposes higher requirements on gout medications.
Although existing URAT1-targeting drugs have many limitations, 90% of hyperuricemia cases are currently caused by impaired renal urate excretion. URAT1 inhibitors can promote the excretion of uric acid from the body and reduce serum uric acid levels by inhibiting urate reabsorption.
Therefore, the value of URAT1 remains significant. Despite the tumultuous development histories of earlier agents such as benzbromarone and lesinurad, subsequent developers have continued to pursue the URAT1 pathway, focusing their breakthrough efforts on ensuring safety.
A study on the URAT1 inhibitor AR882 was presented at the ACR conference, aiming to evaluate the safety and efficacy of AR882 versus placebo in patients with gout.
This was a global, multicenter, randomized, double-blind, 12-week, placebo-controlled Phase 2b clinical trial that enrolled 140 gout patients aged 18–75 years, with an estimated glomerular filtration rate (eGFR) >30 mL/min/1.73 m² and a mean baseline serum uric acid (SU) level of 8.6 (±1.3) mg/dL. Participants were randomly assigned in a 1:1:1 ratio to three groups: AR882 50 mg, AR882 75 mg, and placebo. Blood samples were collected every two weeks over a 12-week follow-up period to monitor SU levels and treatment safety.
Patients enrolled in the study also had common comorbidities, such as hypertension, hyperlipidemia, chronic kidney disease, arthritis, diabetes, and cardiovascular disease. The final results showed that, in the intention-to-treat population, 82% and 73% of patients in the 75 mg group achieved serum uric acid (SU) levels <6 mg/dL and <5 mg/dL, respectively; in the 50 mg group, the corresponding proportions were 71% and 45%. In the per-protocol population, the rates in the 75 mg group increased to 89% and 82%, while those in the 50 mg group were 78% and 50%.
Furthermore, patients with an eGFR of 60–89 mL/min/1.73 m² exhibited a treatment response rate similar to that of patients with an eGFR >90 mL/min/1.73 m², and significantly higher than that of patients with an eGFR <60 mL/min/1.73 m². More importantly, no serious adverse events occurred in the treatment group; the incidence of gout flares was approximately 30%, comparable to that in the placebo group. Mild to moderate adverse events observed in the study included diarrhea, headache, and upper respiratory tract infections, none of which led to discontinuation from the trial.
In a 12-week study, AR882 demonstrated favorable safety and efficacy compared with existing medications, breaking the constraint of URAT1 inhibitor-related safety concerns.
In addition to URAT1, the ACR also announced the latest research progress on uricase drugs.
For patients with refractory gout, serum uric acid (SU) levels remain difficult to maintain below 6 mg/dL despite regular treatment, leading to a series of severe symptoms. Currently, novel uricase-based therapies are effective for such patients, but the formation of anti-drug antibodies remains a concern. SEL-212 consists of co-administration of rapamycin (SEL-110) and pegylated uricase (a highly immunogenic enzyme, SEL-037). It has the potential to reduce the formation of anti-drug antibodies, allowing for convenient once-monthly dosing while improving the efficacy and tolerability of uricase therapy.
Study Presented at the ACR Meeting Evaluates the Safety and Efficacy of SEL-212 in Treating Refractory Gout in Adults
This study was a placebo-controlled, double-blind, randomized clinical trial. The US cohort (D1) enrolled 112 patients (96% male, 66% aged ≥50 years), and the global cohort (D2) enrolled 153 patients (97% male, 72% aged ≥50 years). Inclusion criteria were ≥3 gout flares within 18 months, presence of one or more tophi, or a current diagnosis of gouty arthritis with serum uric acid (SU) not normalized despite no use of xanthine oxidase inhibitors, along with no prior treatment with pegylated uricase.
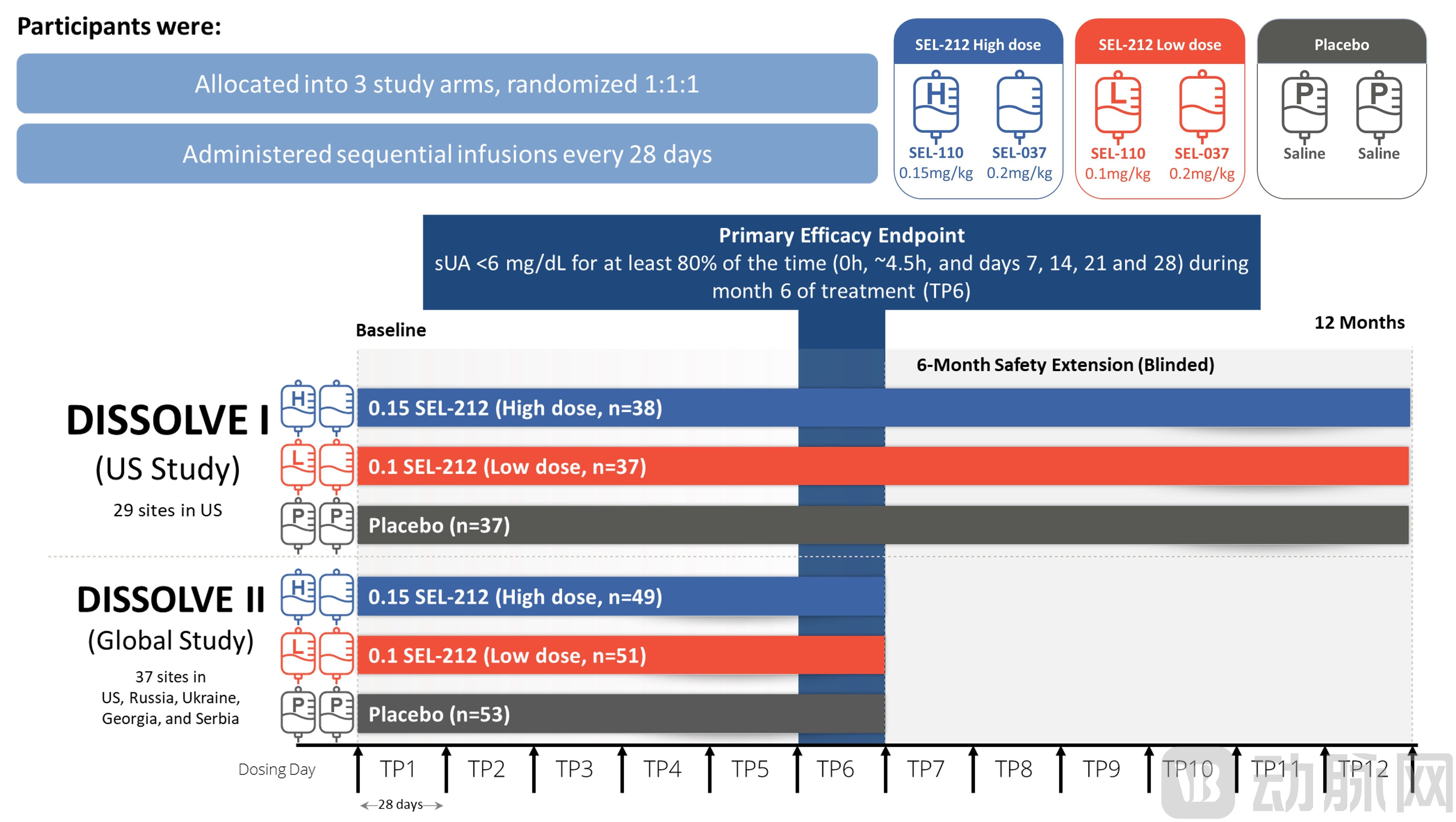
SEL-212 Study Design, Image Source: ACR
The results showed that the response rates in all treatment groups were significantly higher than that in the placebo group (p≤0.0008). In the US cohort and the global cohort, the response rates for the high-dose groups were 56% and 46%, respectively, while those for the low-dose groups were 48% and 40%, respectively. Among patients aged over 50 years, the response rates for the high-dose groups in the two cohorts were 65% and 47%, respectively, and those for the low-dose groups were 47% and 44%, respectively (p≤0.0026 vs. placebo). Notably, infusion reactions occurred in 3.4% and 4.5% of patients in the high-dose and low-dose groups, respectively, with incidences comparable to that in the placebo group.
Compared with the placebo group, once-monthly SEL-212 treatment demonstrated statistically significant improvements in response rates and serum uric acid reduction, while maintaining a favorable safety profile. It may provide a new therapeutic option for patients with refractory gout beyond xanthine oxidase inhibitors (XOIs) and URAT1 inhibitors.
Safety concerns have long been the Sword of Damocles hanging over gout medications. Research presented at the ACR suggests that pharmaceutical companies may have taken the most critical step forward.
Faced with huge market demand, domestic pharmaceutical companies are naturally not absent; many Chinese enterprises, including Hengrui, ApicHope, and Yifang Biopharma, have made their layouts.

Progress of Domestic Gout Drug Development, Data Sourced from Public Information and the CDE
Although URAT1 inhibitors first emerged in the 1970s, safety concerns have long overshadowed this star therapeutic target. Following the FDA approval of AstraZeneca’s lesinurad in 2015, more than 10 companies in China entered the field. However, subsequent studies indicated that safety issues remained unresolved, with monotherapy regimens demonstrating nephrotoxicity. Consequently, R&D efforts have shifted toward combination therapies.
Hengrui Medicine’s SHR4640 follows this approach. SHR4640 has been approved to conduct multiple clinical studies. Its Phase III clinical trial as monotherapy for the treatment of primary gout with hyperuricemia was already underway in 2019, yet the clinical results have not been disclosed. Subsequently, a Phase II clinical trial combining SHR4640 with febuxostat was initiated in 2022.
On one hand, followers of the lesinurad pathway face challenges; on the other, benzbromarone is experiencing a turnaround. Studies have revealed that the hepatotoxicity of benzbromarone is caused by p-benzoquinone generated through arylation oxidation at the carbon adjacent to the benzofuran ring. Avoiding the formation of p-benzoquinone is expected to resolve its safety concerns.
In 2019, Fuji Yakuhin, a Japanese pharmaceutical company, released clinical data on dotinurad. Dotinurad was developed by modifying the ring structure adjacent to the benzene ring of benzbromarone, thereby reducing hepatotoxicity. Clinical data showed that after two weeks of treatment with an initial dose of 0.5 mg, patients’ serum uric acid (SU) levels decreased significantly. After 10 weeks, with a maintenance dose of 2 mg, 80%–90% of patients achieved SU levels below 6 mg/dL. By the study endpoints at 34 or 58 weeks, 90% of patients had their SU levels reduced to below 6 mg/dL. The overall efficacy was comparable to that of benzbromarone, and no serious adverse reactions were observed.
In 2020, Eisai acquired the exclusive rights to develop and market dotinurad in China. The drug is currently in Phase III clinical trials. The promising performance of this new drug has once again made URAT1 a hot topic, prompting domestic followers to jump on the bandwagon.
Evopoint Biosciences’ XNW3009 has adopted the same mechanism as dotinurad, achieving uric acid-lowering efficacy at low doses. The drug has completed Phase II clinical trials and is poised to enter Phase III. Phase II data showed that in the 0.5 mg dose group, over 72% of subjects achieved serum uric acid levels ≤360 μmol/L after each administration, compared with 51.9% of subjects in the control group receiving 50 mg of benzbromarone.
Overall, the clinical data for XNW3009 demonstrated efficacy comparable to dotinurad. The 0.5 mg dose group showed a significantly greater reduction in serum uric acid levels than the benzbromarone 50 mg dose group. XNW3009 exhibited good safety and tolerability, with no apparent hepatotoxic or nephrotoxic adverse effects. Furthermore, it displayed favorable pharmacokinetic and pharmacodynamic profiles in clinical pharmacology studies.
Furthermore, Arthrosi, an affiliate of ApicHope, has completed its End-of-Phase 2 (EOP2) meeting with the U.S. Food and Drug Administration (FDA) regarding the innovative drug AR882. The FDA’s written feedback supports Arthrosi in advancing the global Phase III clinical trials of AR882 as planned. Results from the global Phase IIb clinical trial, presented at the American College of Rheumatology (ACR) Annual Meeting, demonstrated favorable efficacy and safety profiles while overcoming the high hepatorenal toxicity associated with previous therapies, thereby offering potential for differentiated competition. In addition to these recent breakthrough clinical findings, ApicHope stated that it will present additional pharmacokinetic and pharmacodynamic data at subsequent conferences.
In addition to URAT1 inhibitors, Innovent Bio licensed Tigulixostat (IBI-128) from LG Chem for RMB 660 million in late 2022. Tigulixostat is a drug developed based on xanthine oxidase inhibitors (XOIs). It demonstrated favorable efficacy in lowering serum uric acid levels and a good safety profile in Phase 2 clinical trials. Compared with the placebo group and febuxostat, all dose groups of Tigulixostat achieved the primary endpoint of serum uric acid levels below 5 mg/dL at the third month of treatment. LG Chem initiated international multicenter Phase 3 clinical trials for Tigulixostat in late 2022.
It is evident that domestic pharmaceutical companies have established a robust pipeline of gout medications, with many candidates reaching late-stage clinical trials. Several new drugs are expected to gain approval in the coming years. However, from another perspective, the current strategy of Chinese pharmaceutical firms remains predominantly follow-on. Although dotinurad has not yet raised safety concerns, any emerging issues could lead to delays in R&D progress similar to those experienced by SHR4640. With hundreds of millions of gout patients in China urgently awaiting safe and effective new therapies, the company that truly meets their needs will be the one to unlock this blue-ocean market.