Cheng Xinghua of Shanghai Chest Hospital: Precision Localization Brings Clarity to Surgery

Without navigation, you would get lost while driving and wander at various intersections.
By the same token, if the precise location of the lesion cannot be identified, the surgeon operates in a fog. Therefore, surgeons also require a navigation system to map out a route and guide the precise resection of the lesion.
This isMedical Navigationsignificance.
In clinical practice,Cheng Xinghua, Associate Chief Physician at Shanghai Chest Hospital, Shanghai Jiao Tong University School of MedicineIt has been found that many lung cancer patients with small nodules require preoperative localization. The localization process is quite painful, as it involves inserting a thin needle into the patient's lungs. The patient must lie still for an extended period. Although local anesthesia is administered, the patient remains conscious, which can be very distressing and often causes significant fear among patients.
As a physician, Cheng Xinghua aims to change this situation.
He hopesThe final product is not merely about positioning; it is multidimensional, human-centric, emotionally resonant, and inclusive of all lives.He stated, “The purpose of integrating medicine and engineering is to benefit more patients.” This process resembles a vessel into which one pours their knowledge, observations, thoughts, and even a part of their soul.
Starting with positioning, but going beyond it
With the widespread adoption of lung cancer screening, patients with varying clinical conditions require different surgical approaches.
Cheng Xinghua stated that among patients eligible for surgery, physicians further stratify cases to develop more precise surgical plans, thereby delivering more personalized treatment. Taking early-stage lung cancer as an example, lesion- or nodule-centered limited lung resection has become a prominent surgical approach in the current management of early-stage disease.
“Perhaps 60% to 70% of the patients at our hospital require surgery for early-stage lung cancer,” Cheng Xinghua told VCBeat. “While such procedures minimize patient trauma, they entail an increase in surgical steps.”
The additional surgical steps areLung Nodule Localization。
In the past, localization of pulmonary nodules was primarily achieved by placing markers via CT-guided interventional puncture, which required patients to remain conscious during the procedure. Regarding the interventional puncture technique itself, Cheng Xinghua stated, “The puncture procedure is relatively time-consuming and involves a certain learning curve. Most surgeons lack relevant experience, making it relatively difficult for them to perform the puncture independently.”
Moreover, interventional puncture procedures require hospitals to be equipped with a CT scanner, which also occupies valuable hospital equipment and resources.
Therefore, Cheng Xinghua’s initial concept was to explore the possibility of transferring preoperative imaging data into the operating room to guide needle placement and localization, thereby sparing patients from undergoing multiple punctures in the CT suite. “By using a head-mounted wearable device, physicians can project virtual information onto the patient’s body, enabling a pain-free localization process while the patient is under general anesthesia.”
Guided by this approach, Cheng Xinghua initiated the development of related projects in 2018. In the same year, the project received support from the Shanghai Municipal Science and Technology Commission’s “Science and Technology Innovation Action Plan” and completed its first proof-of-concept clinical trial. Cheng Xinghua was also invited to present on “New Technologies” at the American Association for Thoracic Surgery.
Cheng Xinghua shared:Intraoperative Digital Surgical System。
This system offers two major advantages: first, it provides real-time guidance to surgeons for positioning and needle insertion paths during interventional and minimally invasive procedures, while also recording the surgical process; second, it generates precise, real-time digital localization through digitization, making spatial awareness more tangible for surgeons and facilitating clearer decision-making.
And this is underpinned byDigital Surgical Ecosystem, Mixed Reality, Artificial Intelligence, and Digital TwinsCore technologies such as medical navigation. Taking artificial intelligence as an example, multi-channel physiological data are acquired to calibrate organ motion and morphology under normal physiological conditions. AI is then employed to automatically segment and reconstruct whole-organ models of the human body, perform pathological analysis of lesions in specific organs, and proactively avoid blood vessels and nerves based on the target organ and surgical procedure, thereby assisting surgeons in selecting the safest surgical approach.
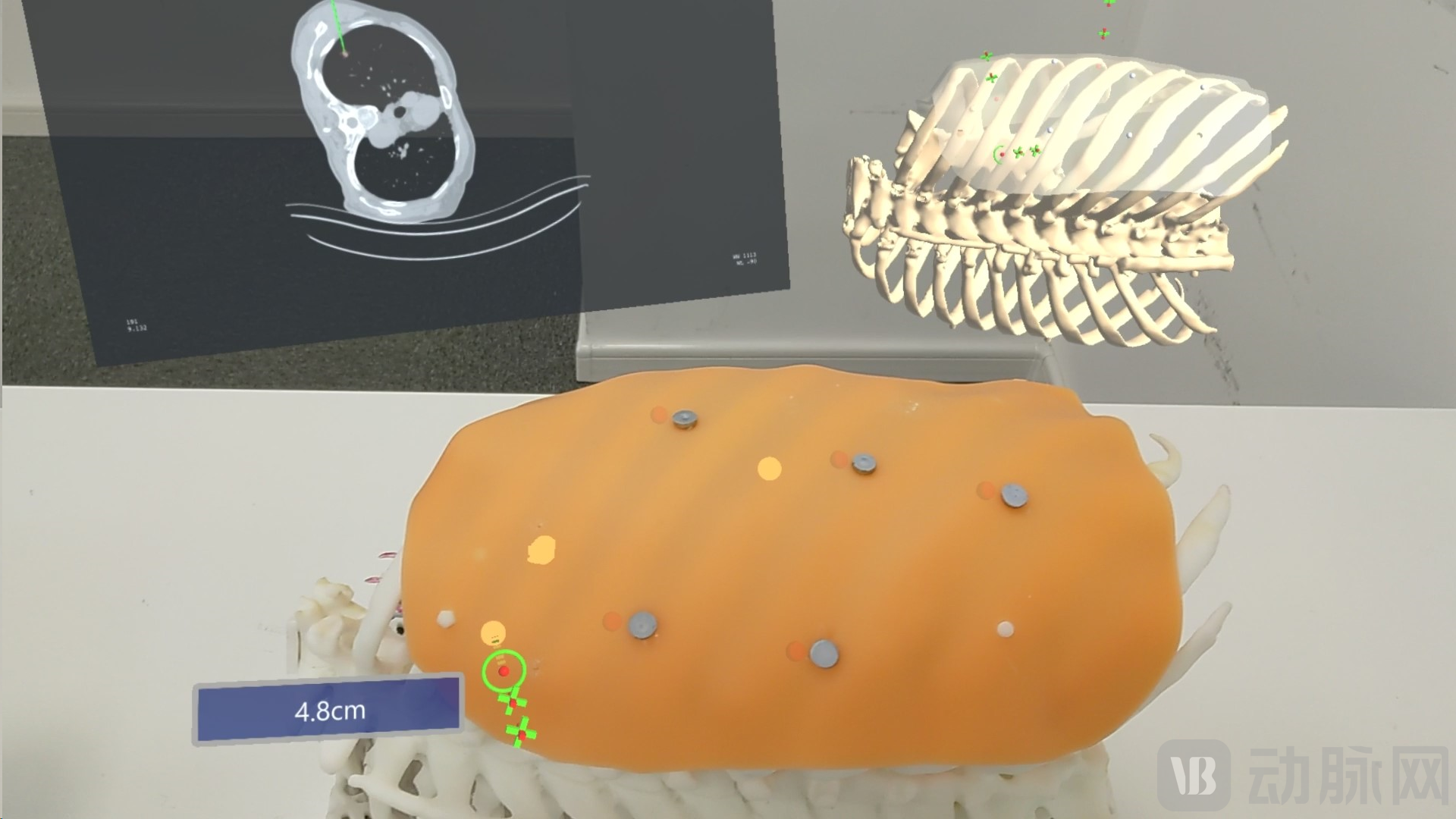
Schematic diagram of the model; image provided by the interviewee.
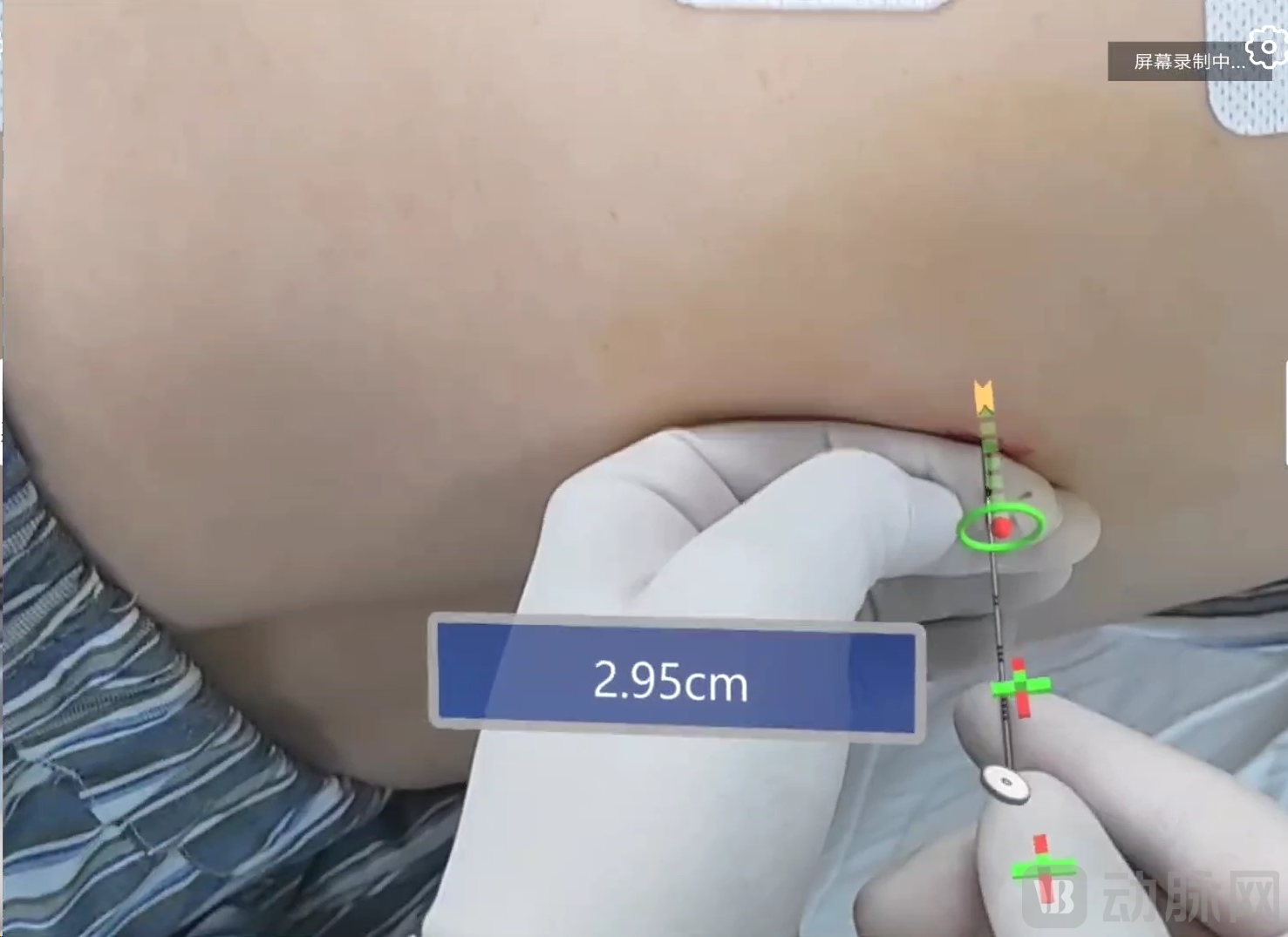
Intraoperative screenshot, provided by the interviewee
Cheng Xinghua revealed that the intraoperative digital surgery system has already completedNearly 50 casesInterventional Localization Case. “It can reduce the puncture time to within 3–5 minutes, significantly alleviating patient pain—the interventional procedure can be completed with only 1–2 CT scans.”
After four years of research and development, Cheng Xinghua’s collaborative team was established in 2022.Zhenmiaojing Medical Technology Co., Ltd., this is currently the world's first mixed reality digital surgery company dedicated to thoracic and pulmonary interventional and minimally invasive techniques.
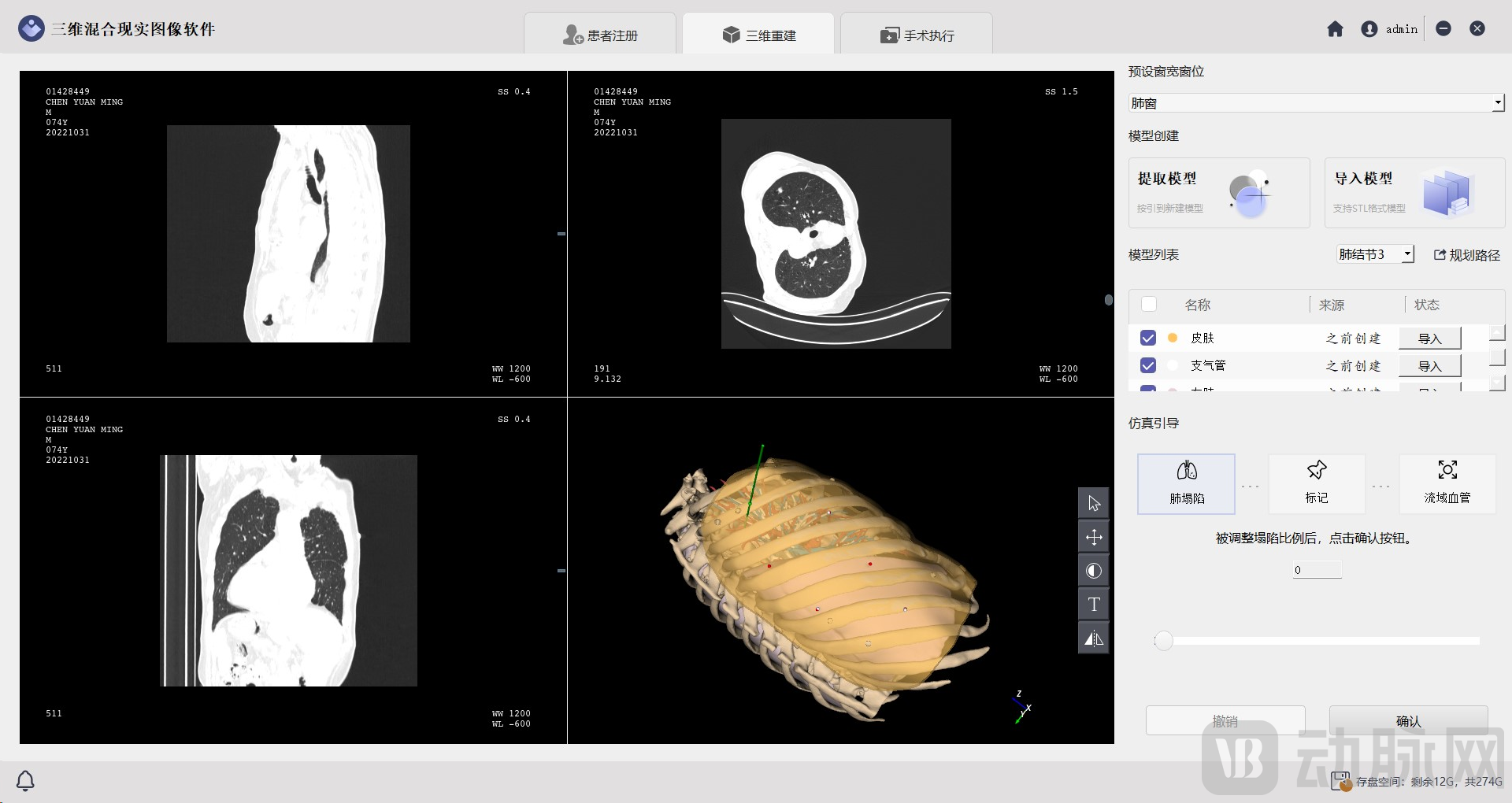
“Golden Eye” Local Model for Rapid Reconstruction and Surgical Planning, Image Provided by Interviewee
In 2023, the next-generation product under Zhenmiaojing Medical"Golden Eye"Obtained Class II medical device registration certificate and production license. In the future, Jinjing will not only perform functions such as nodule localization, puncture biopsy, and tumor ablation, but also be applied to multiple clinical scenarios including endoscopic surgery, open surgery, and reconstructive repair surgery.
Integration of Medicine and Engineering Must Be Based in Hospitals
Physician innovation is a cycle—discovering insights in clinical practice and returning them to clinical application.
“Actionable original innovation,Innovation must be driven by clinical needs..” Cheng Xinghua introduced the process of innovation and translation to Orange Fruit Bureau: After doctors identify key points of clinical needs and propose ideas for improvement, engineers then carry out the engineering implementation.
This requires a translational team, specifically one that integrates medicine and engineering.
“The core of medical-engineering integration must beHigh Alignment of Goals and Adequate Allocation of Resources.” When discussing the key factors for success in medical-engineering integration, Cheng Xinghua stated.
From Cheng Xinghua’s team, you may gain a more tangible sense of this. “We all recognize the value of this field, are willing to engage in deep thinking, and are proactive in addressing challenges as they arise,” said Cheng Xinghua.Every team member demonstrates exceptional execution and efficiency.“We need a team that can make five corrections a day, not one that makes five corrections a year. Thus, within a single day, we were able to rapidly improve the product with just two personnel.” Under such highly efficient collaboration, Cheng Xinghua’s team completed the animal experimental validation of the initial prototype within two years.
It can be said that Cheng Xinghua’s increasingly precise understanding of the integration of medicine and engineering has been driving the entire team forward. As the person at the forefront, he is more concerned with how to establish a rapid and effective communication mechanism.
To enable engineers to rapidly refine product details, Cheng Xinghua specifically secured an unused office space within a hospital for the engineering team to work on-site. “Whenever I have free time, I go to this office to communicate and collaborate with the team.” In Cheng Xinghua’s view, medical-engineering integration should not be confined to university laboratories or corporate offices.Must be kept in the hospital., which facilitates continuous follow-up by physicians and allows for timely modifications.
The product needs to be more down-to-earth.
How to Determine Whether an Achievement Can Be Commercialized and Accepted by the Market?
Cheng Xinghua’s response to VCBeat’s “Orange Bureau” focused on the business model. “After identifying clinical needs, we still need to find a business model that ensures returns for all participants.”
As one of the earliest teams in China to adopt digital procedures in the field of interventional medicine, for Professor Cheng Xinghua’s team,The product’s business model remains a shoe that has yet to drop.“We have not yet determined whether to position our digital product under the information technology channel or the medical device regulatory pathway,” Cheng Xinghua revealed. Currently, the team is actively engaging in discussions with colleagues from hospital IT departments and medical affairs offices to further solidify the clinical application of the product.
On the other hand, Cheng Xinghua’s team isMake the product as down-to-earth as possible.“Our top priority at present is to reduce product costs, improve efficiency, and enhance the integration of our products with existing surgical procedures,” said Cheng Xinghua. He explained that the team’s specific approach involves customizing commercially available products and integrating them with software systems developed in-house, thereby achieving improved performance and cost reduction.
In fact, the “grounded” approach mentioned by Cheng Xinghua refers to the rapid application of the product in existing surgical systems. To this end, the team hasHaving established a strategic direction toward digitalization and intelligence, we aim to leverage digital means to enhance product efficiency and reduce input costs, ultimately benefiting patients.