Anthos Therapeutics Submits IPO Prospectus Following Early Termination of Phase 2 Trial for Abelacimab Due to Overwhelming Efficacy

Anthos Therapeutics
Antibody Drug Developer
On September 18, 2023, biotechnology company Anthos Therapeutics (“Anthos”) announced that regarding abelacimabAZALEA-TIMI 71 Clinical TrialThe Phase 2 study met its primary endpoint.
This study was conducted in 1,287 patients with atrial fibrillation at moderate to high risk. Compared with patients receiving the standard-of-care drug rivaroxaban, those treated with abelacimab had a significantly lower composite endpoint of major bleeding and clinically relevant non-major bleeding, demonstrating an “overwhelming advantage” in efficacy; consequently, the trial was terminated early upon the recommendation of the Data Monitoring Committee. The study showed that150 mg of abelacimab can almost completely inhibit coagulation factor XI.
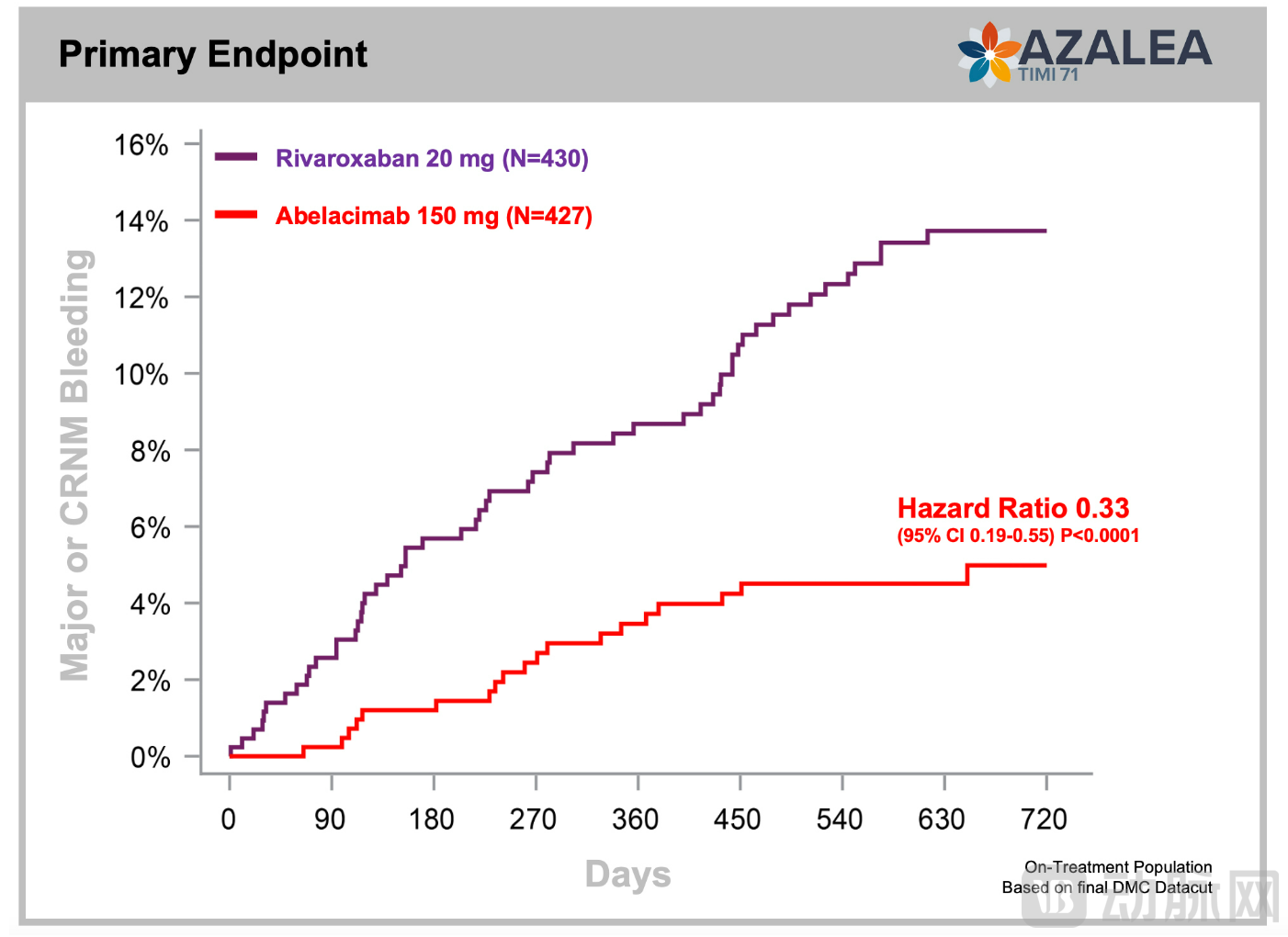
AZALEA-TIMI 71 Study Results (Image source: Anthos Therapeutics official website)
Abelacimab is a novel, highly selective, fully human monoclonal antibody. By binding to the catalytic domain of coagulation factor XI, abelacimab locks it in an inactive precursor conformation (zymogen state), preventing its activation by coagulation factor XIIa or thrombin. Consequently, abelacimab exhibits dual activity targeting both coagulation factor XI and its activated form, factor XIa, thereby reducing the risk of thrombosis while preserving physiological hemostasis through a decoupled coagulation mechanism.
Trial results demonstrated that Abelacimab not only possesses the ability to prevent thrombosis but also exhibits superior safety and tolerability.
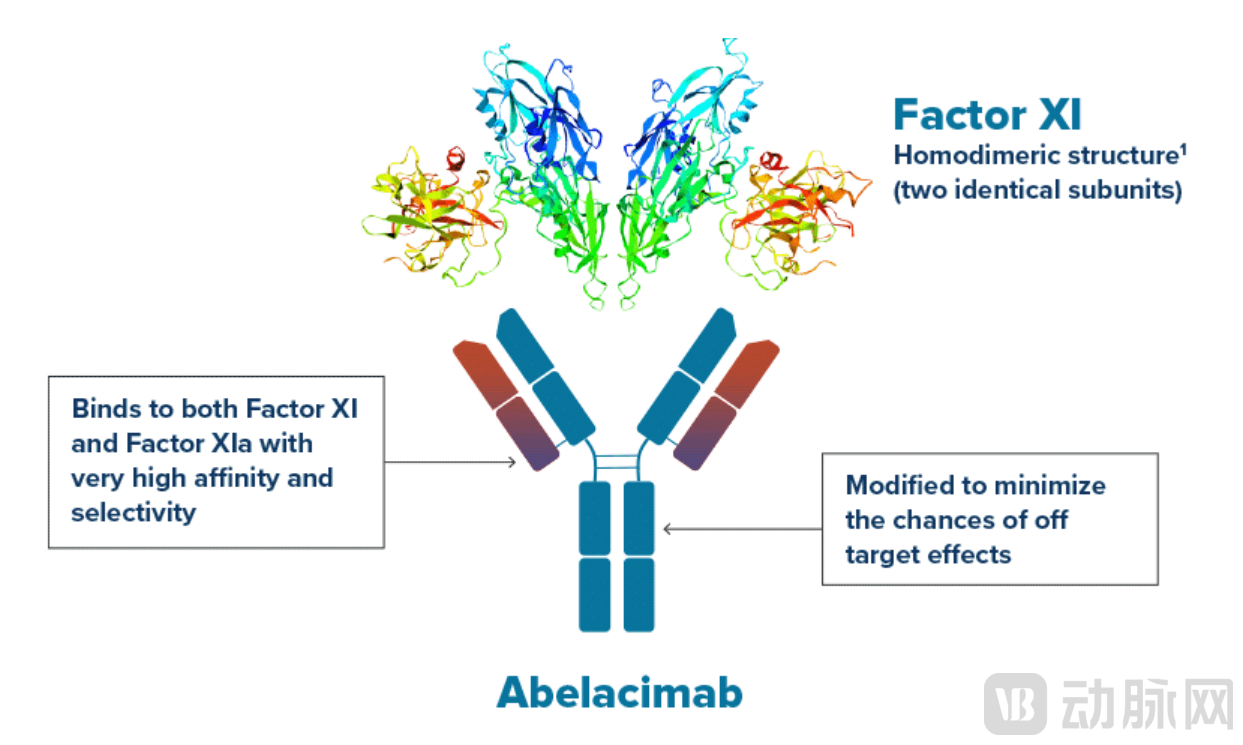
Schematic Diagram of the Mechanism of Action of Abelacimab (Image source: Anthos Therapeutics official website)
Currently, Anthos Therapeutics has initiated an extension study of AZALEA-TIMI 71, which will allow subjects originally assigned to rivaroxaban to switch to abelacimab treatment. Furthermore,The company is conducting research on cancer-associated thrombosis and has completed two Phase III trials: ASTER (a comparative trial of abelacimab versus apixaban) and MAGNOLIA (a comparative trial of abelacimab versus dalteparin).。
Anthos Therapeutics is a biopharmaceutical company based in Massachusetts, USA, dedicated to developing next-generation targeted therapies for patients with cardiovascular diseases. Unlike other startups, Anthos was established through a collaboration between Blackstone Life Sciences (a portfolio company of The Blackstone Group) and Novartis, creating a dual-support model leveraging both capital and resources.
Under the cooperation agreement, Blackstone Life Sciences provided $250 million in funding to Anthos Therapeutics and assumed responsibility for overseeing the development of new products. Novartis licensed Anthos Therapeutics to continue the research and development of MAA868 (the predecessor of abelacimab), an antibody therapy targeting coagulation factors XI and XIa, while also holding a minority equity stake in Anthos Therapeutics.
Prior to authorization, Novartis’s preclinical studies on MAA868 demonstrated that non-human primates treated with MAA868 exhibited sustained anticoagulant activity, with no signs of bleeding observed. In the first-in-human trial, Novartis reported that MAA868 was well tolerated, with its activity lasting for at least four weeks.
Due to the high costs and substantial risk of failure associated with cardiovascular drug development, biotechnology startups and large pharmaceutical companies face financial challenges at various stages. Blackstone’s investment model is designed to address these financial constraints through venture capital. Building on this approach, Anthos optimizes traditional operational models by combining the agility of small biotech firms with the strength of large pharmaceutical companies. It integrates senior leadership with development and manufacturing activities—executed through external partners—to ensure quality across drug development, production, regulatory compliance, and commercialization. This model organically aligns products, cash flow, and value creation to meet the shared needs of Anthos, its partners, and investors, achieving a win-win outcome.
Cardiovascular and metabolic diseases remain the “number one killer” threatening human health.
Thrombotic diseases are a subset of cardiovascular diseases, involving two pathological processes: thrombosis and thromboembolism. They can affect arteries or veins, leading to a range of conditions such as ischemic heart disease, ischemic stroke, peripheral artery disease, and venous thromboembolism.According to data released by the International Society on Thrombosis and Haemostasis, globally every4Among them1Deaths from diseases associated with arterial thromboembolic events (such as ischemic heart disease or stroke), with incidence rates in the past 20 Sharp Mid-Year Surge 。
Similarly, venous thromboembolism (VTE) also constitutes a substantial health burden. Data released by the Expert Committee of World Thrombosis Day show that there are nearly 10 million cases of VTE globally each year, affecting both developed and developing countries, and claiming more than 800,000 lives annually in the United States and Europe alone.
The National Comprehensive Cancer Network (NCCN) stated in the 2021 Version 2 of its Guidelines for Cancer-Associated Venous Thromboembolic Disease that cancer patients have a 5- to 7-fold increased risk of developing VTE, making it the second leading cause of death among cancer patients, surpassed only by cancer itself.
John Glasspool, CEO of Anthos Therapeutics, believes that the mortality risk associated with this disease is partly due to the widespread underuse, underdosing, and premature discontinuation of anticoagulants. He pointed out that “approximately 45% of individuals at risk of thrombosis are not receiving appropriate treatment or are experiencing suboptimal therapeutic outcomes, primarily due to concerns about bleeding risks.”
Although some clinical controlled studies have shown that the risk of bleeding is reduced in specific patient groups using direct oral anticoagulants (DOACs), the high annual bleeding rate of 2% to 5% remains clinically significant. Furthermore, new data on atrial fibrillation presented at the 2021 International Society on Thrombosis and Haemostasis (ISTH) Congress indicated that the rate of major bleeding in real-world practice is nearly twice that observed in clinical trials.
The fundamental issue is that all traditional anticoagulants, including direct oral anticoagulants (DOACs), affect both physiological hemostasis and pathological thrombus formation, placing physicians in a difficult position when making treatment decisions. Patients are often frail, elderly, and may have multiple comorbidities; therefore, each treatment requires careful balancing of two risks: the potential risk of life-threatening pathological thromboembolic events and the adverse effects of drug-induced major bleeding.
Therefore,Ideal anticoagulant drugs should possess dual functions: effectively preventing coagulation without interfering with the normal hemostatic process.For many years, vitamin K antagonists (VKAs) such as warfarin were the traditionally available oral anticoagulants; however, their pharmacokinetic properties and mechanism of action result in a narrow therapeutic window, necessitating frequent dynamic monitoring and posing a significant risk of bleeding.
Rivaroxaban, a relatively new oral anticoagulant approved for marketing in 2008, does not require regular monitoring of coagulation parameters and has a reduced dosing frequency of once daily, thereby effectively improving medication adherence; however, it still carries a risk of bleeding. Research published in JAMA (The Journal of the American Medical Association) indicates that rivaroxaban is associated with a higher risk of bleeding compared to apixaban (Eliquis), another novel oral anticoagulant.
In comparison, vitamin K antagonists (VKAs) such as warfarin exert their effects by inhibiting vitamin K epoxide reductase, ultimately impairing the carboxylation of coagulation factors II, VII, IX, and X. In contrast, rivaroxaban and apixaban, which are commonly used therapeutic agents, function by directly or indirectly inactivating coagulation factor Xa and thrombin.Abelacimab, which had its clinical trial terminated early, targets coagulation factor XI, making it currently the only factor XI inhibitor used for the prevention and treatment of arterial and venous thromboembolism.
According to Anthos, the inspiration for developing this drug came from clinical observations of hemophilia patients. Hemophilia is a bleeding disorder caused by a deficiency of specific clotting factors in the blood. It is classified into types A, B, and C based on the deficient factor: type A and type B result from deficiencies in clotting factor VIII and IX, respectively, while type C is caused by a deficiency in clotting factor XI. Clinical findings have shown that patients with hemophilia C exhibit milder bleeding tendencies and have a lower risk of thromboembolism compared to the general population.
Therefore, researchers hypothesize that coagulation factor XI may play a key role in thrombosis while having a minimal impact on hemostasis, making artificial inhibition of factor XI a promising ideal anticoagulant therapy. Current drugs targeting factor XI include monoclonal antibodies, small-molecule drugs, and antisense oligonucleotides; abelacimab is one such monoclonal antibody agent.
Furthermore, abelacimab requires only once-monthly administration and is associated with a reduced risk of bleeding. Meanwhile, its in vivo metabolic pathway lessens the burden on the liver and kidneys, making it more favorable for patients with related conditions.
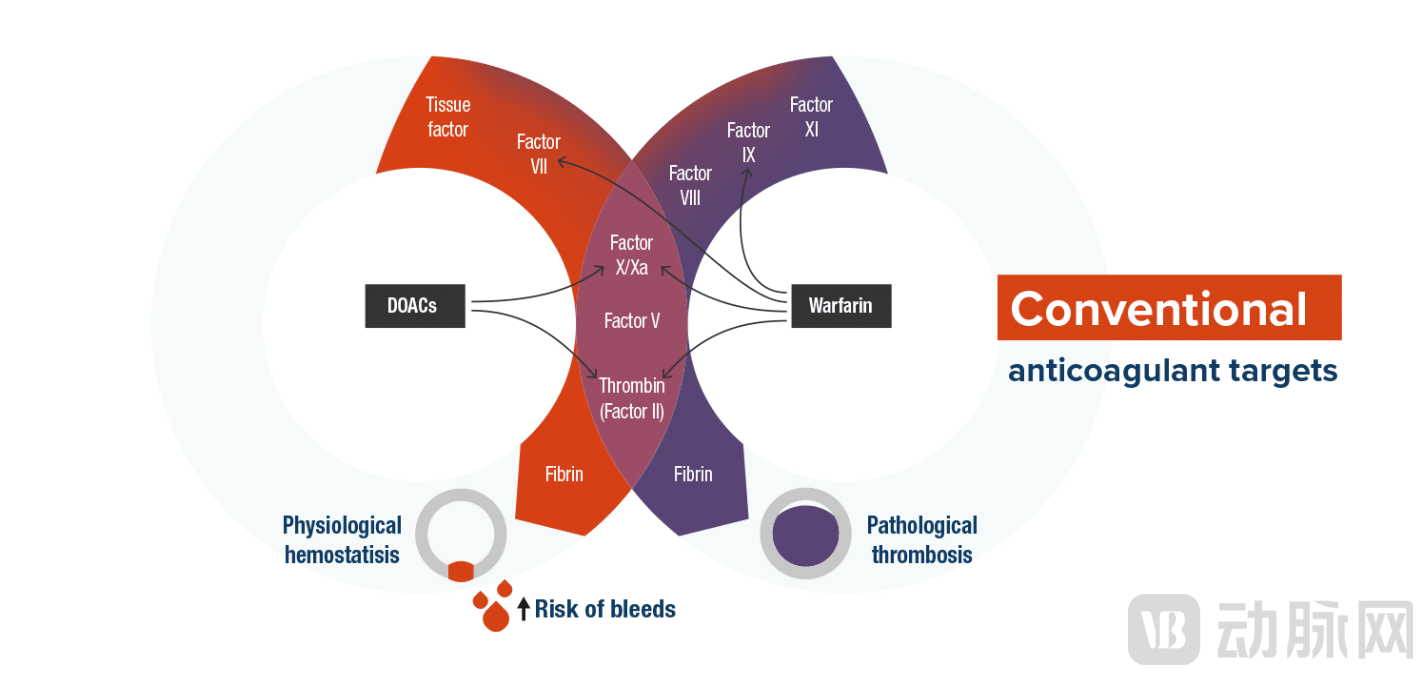
Schematic Diagram of the Mechanism of Action of Traditional Anticoagulants (Image source: Anthos Therapeutics official website)
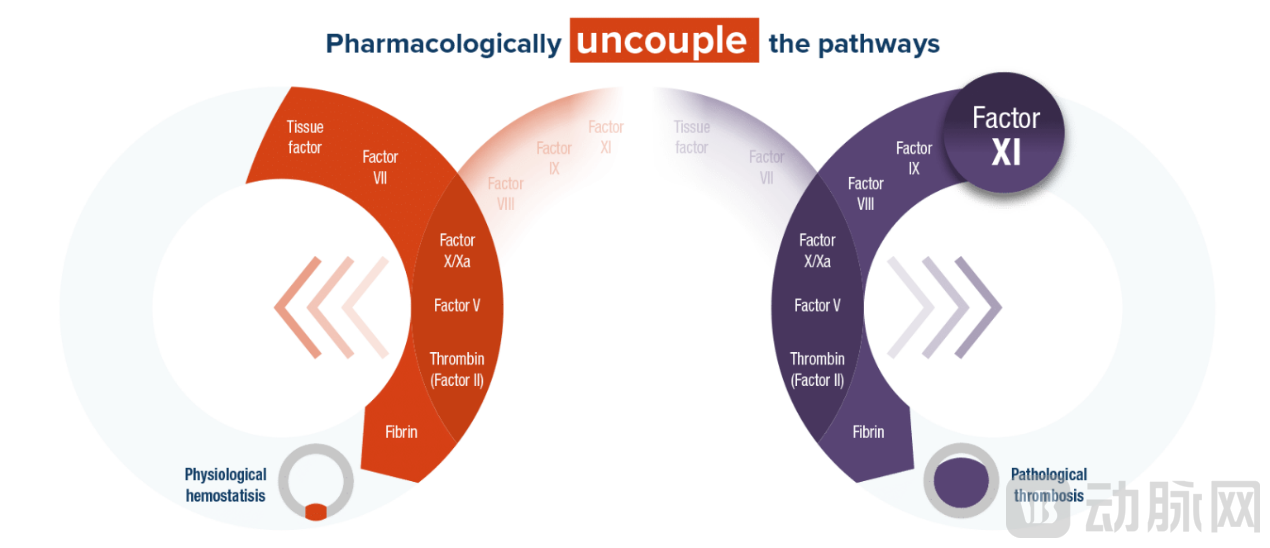
Factor XI Schematic Diagram of Mechanism of Action (Image source: Anthos Therapeutics official website)
On July 11, 2022, the FDA granted Fast Track designation to Abelacimab for the treatment of cancer-associated thrombosis (CAT). Previously, Anthos Therapeutics had completed two Phase III clinical trials: MAGNOLIA (a comparative trial of Abelacimab versus dalteparin) and ASTER (a comparative trial of Abelacimab versus apixaban).
The MAGNOLIA trial enrolled patients with gastrointestinal (GI) or genitourinary (GU) cancers for whom direct oral anticoagulants (DOACs) were not recommended. In the MAGNOLIA trial, patients in the first group received an intravenous infusion of 150 mg abelacimab on Day 1, followed by monthly subcutaneous injections for up to 6 months; patients in the second group received daily subcutaneous injections of dalteparin at a dose of 200 IU/kg/day for the first month, followed by 150 IU/kg/day for up to 6 months, to evaluate the effects of abelacimab on recurrent venous thromboembolism (VTE) and bleeding in patients with cancer-associated VTE. The results showed thatAbelacimab reduces the risk of VTE recurrence and bleeding in patients with GI/GU cancers.
In the ASTER trial, Anthos primarily compared abelacimab with apixaban regarding VTE recurrence and bleeding outcomes in patients with cancer-associated VTE who were recommended for DOAC therapy. Patients in the first group received a 150 mg intravenous injection of abelacimab on Day 1, followed by monthly subcutaneous injections for up to 6 months; patients in the second group received oral apixaban at a dose of 10 mg twice daily for the first 7 days, then once daily thereafter, for a duration of 6 months.
In September of the same year, the AZALEA-TIMI 71 clinical study by Anthos Therapeutics found that abelacimab targets the active domain of Factor XI, exhibiting dual inhibitory activity against both Factor XI and its activated form, Factor XIa, with high selectivity and high affinity. Consequently, the FDA granted Fast Track designation to abelacimab for research into the prevention of stroke and systemic embolism in patients with atrial fibrillation (AF).This marks the second Breakthrough Therapy designation granted to Anthos Therapeutics in less than two months.
As early as 2021, a Phase II clinical trial conducted by Anthos evaluated the efficacy and safety of three doses of abelacimab (30 mg, 75 mg, or 150 mg) versus enoxaparin in preventing thrombosis in patients following total knee arthroplasty.
This Phase II clinical trial enrolled a total of 412 patients undergoing total knee arthroplasty, who were allocated in a 1:1:1:1 ratio to different dose groups of abelacimab or the enoxaparin group. Participants were assigned to receive either a single intravenous injection of abelacimab (30 mg, 75 mg, or 150 mg) or daily subcutaneous injections of 40 mg enoxaparin postoperatively.
Trial results published in The New England Journal of Medicine demonstrated that abelacimab increased the activated partial thromboplastin time (aPTT), a key coagulation parameter reflecting the intrinsic coagulation pathway, whereas enoxaparin did not exhibit this effect. Meanwhile, factor XI activity and free factor XI levels were negatively correlated with plasma concentrations of abelacimab.
Regarding safety endpoints, abelacimab effectively reduced the incidence of postoperative venous thromboembolism. In the group receiving abelacimab 30 mg, 13% of patients (13 out of 102) experienced venous thromboembolism; the rates were 5% in the 75 mg group and 4% in the 150 mg group, compared with 22% in the enoxaparin group.
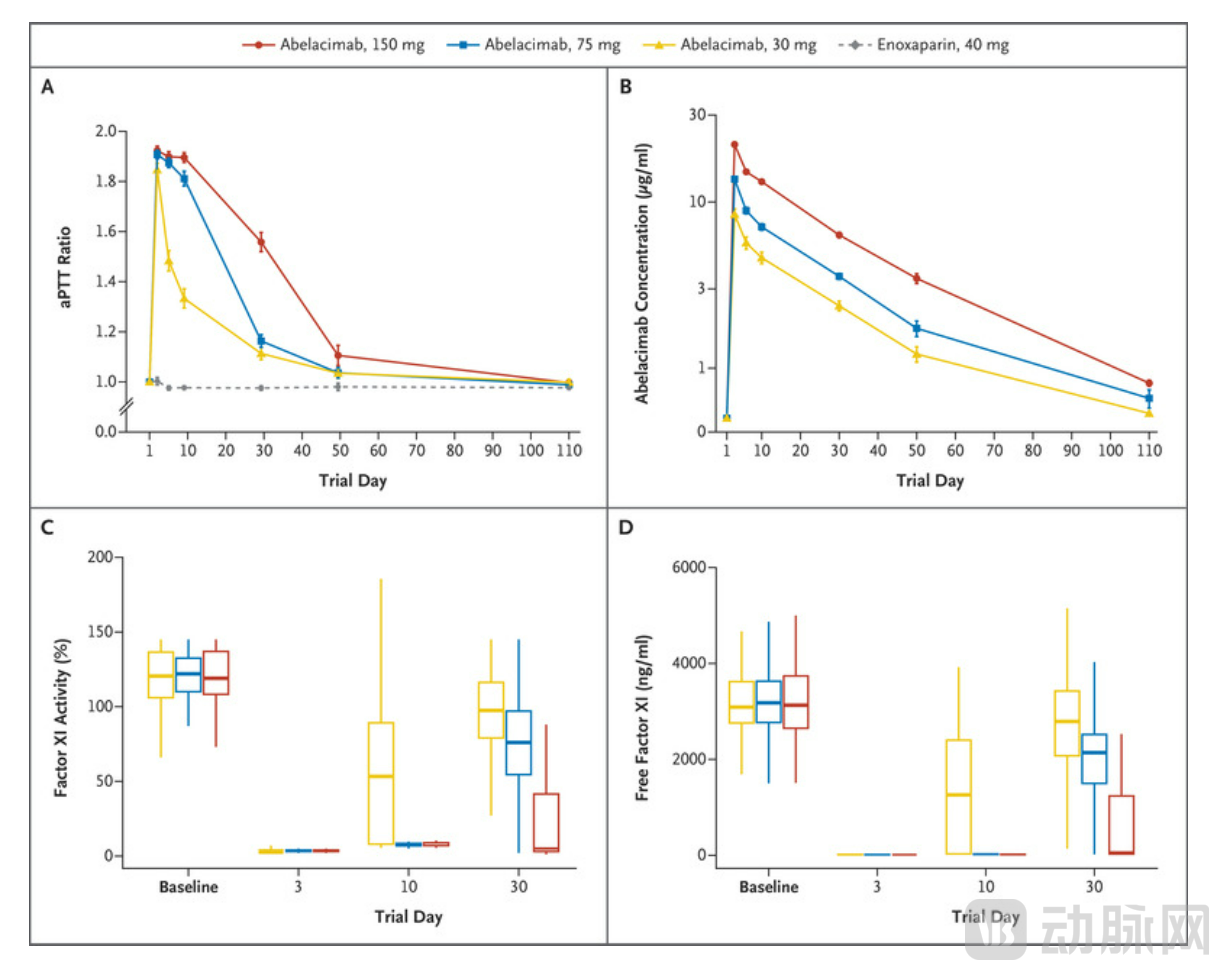
Results of the Comparative Trial of Abelacimab versus Enoxaparin (Image source: The New England Journal of Medicine)
If subsequent research data on abelacimab remain favorable, rivaroxaban and apixaban, two blockbuster drugs, will face formidable competition.