JAK Inhibitors Enter the Eve of Commercial Breakthrough Following Removal of Black Box Warnings

CSPC
Innovative Drug Research and Development, Manufacturer

Zelgen
Innovative Drug Research and Development, Manufacturer

Highlightll Pharma
Innovative Drug Developer

Hengrui Pharma
Innovative and High-Quality Pharmaceutical Developer

Dizal
Innovative Biopharmaceutical R&D Developer

BeOne
Developer of Molecular Targeted and Immune Anti-Tumor Drugs

InnoCare
Innovative Drug Developer
Hot therapeutic areas have always been fiercely contested by multinational corporations (MNCs). In addition to the highly popular oncology sector, the autoimmune disease field is also a sought-after target.
According to data from The Lancet and the Chinese Journal of Dermatology, approximately 7.6%–9.4% of the global population suffered from various types of autoimmune diseases between 2019 and 2020. The American Autoimmune Related Diseases Association (AARDA) estimates that the number of autoimmune disease patients in the United States is as high as 50 million. As autoimmune diseases are currently difficult to cure completely and require long-term medication, the market for autoimmune disease drugs is substantial.
According to Frost & Sullivan’s estimates, the global market size for autoimmune disease drugs was projected to reach $132.3 billion in 2022, with the biologics segment accounting for $96.4 billion, or 72.9% of the total. Among the top 100 best-selling drugs in 2022, 18 were indicated for autoimmune diseases, representing approximately 18% of total sales.
As the patent for the previous generation’s “blockbuster drug” Humira expires, the arms race for next-generation autoimmune therapies is in full swing. Following continuous updates and iterations, JAK—a hot target in the autoimmune field—is ushering in a new chapter. Meanwhile, numerous domestic pharmaceutical companies are beginning to explore autoimmune drugs beyond their traditional focus on oncology.
The Multi-Indication Path of JAK Inhibitors Is Advancing in Multiple Directions
Due to the comorbidity among autoimmune diseases, patients with one autoimmune disorder are more susceptible to developing other types of autoimmune conditions. Given that immune-related pathways often interact with each other, a single drug can cover multiple indications. Consequently, both marketed and investigational autoimmune drugs are expanding toward multi-indication applications, with even type 1 diabetes becoming a target for JAK inhibitors.
In patients with type 1 diabetes, an irreversible decline in pancreatic β-cell function occurs. Although most patients are already at the clinical stage of type 1 diabetes at initial diagnosis and begin insulin replacement therapy, preserving residual β-cell function is associated with reduced glycemic variability and a lower risk of long-term complications, holding significant positive clinical implications.
In December 2023, a study published in The New England Journal of Medicine (NEJM) demonstrated that 48 weeks of daily treatment with the JAK inhibitor baricitinib preserved β-cell function in patients with newly diagnosed type 1 diabetes, suggesting that baricitinib represents a promising new potential therapeutic option for this condition.
This study was conducted by Professor Thomas Kay’s team at the St Vincent’s Institute of Medical Research in Australia. It was a multicenter, randomized, double-blind, placebo-controlled Phase 2b clinical trial involving 91 participants aged 10 to 30 years who had been newly diagnosed with type 1 diabetes and retained clinical C-peptide secretion. Participants were randomly assigned in a 2:1 ratio to receive either baricitinib (4 mg orally, once daily) or placebo.
The primary endpoint of the study was the mean C-peptide level under the concentration–time curve during a 2-hour mixed-meal tolerance test at Week 48: a higher mean C-peptide level indicates protection of β-cells from ongoing immune-mediated destruction, preservation of β-cell function, and stabilization of the pathological state.
The results showed that after 48 weeks of intervention, the median mean level of mixed-meal-stimulated C-peptide in the baricitinib group was 0.65 nmol/(L·min) (interquartile range, 0.31–0.82), which was significantly higher than that in the placebo group [0.43 nmol/(L·min) (interquartile range, 0.13–0.63)]; the adjusted mean between-group difference (ln[AUC+1]) was 0.13 (95% CI, 0.06–0.20; P=0.001).
Secondary endpoints included changes in HbA1c from baseline and daily insulin dosage. The results showed that after 48 weeks, the mean daily insulin doses in the baricitinib and placebo groups were 0.41 U/(kg·d) and 0.52 U/(kg·d), respectively. HbA1c levels were similar between the two groups. The mean coefficients of variation assessed by continuous glucose monitoring were 29.6% and 33.8%, respectively, with the baricitinib group showing a lower value than the placebo group. In terms of safety, no serious adverse events occurred in either group.
Although previous animal studies have shown that JAK inhibitors can induce diabetes reversal in non-obese diabetic mice, achieving diabetes reversal or clinical remission as an ideal endpoint remains highly challenging. As noted in the NEJM, patients with Stage 3 type 1 diabetes already have irreversible damage to β-cell mass at the time of diagnosis; therefore, discontinuation of insulin therapy is not a realistic goal.
The significance of this study lies in the fact that, for patients with type 1 diabetes diagnosed at an early stage 2 or partial stage 3, this therapy can effectively reduce the need for exogenous insulin in subsequent treatment. Furthermore, JAK inhibitors are poised to become the first oral tablet medication approved for improving outcomes in type 1 diabetes.
As research deepens, the applications of JAK inhibitors have expanded beyond autoimmune diseases to include certain oncology indications. However, to capture a broader market share, JAK inhibitors must still address their inherent “limitations.”
JAK inhibitors must first address safety concerns to expand their market.
JAKs constitute an important family of non-receptor tyrosine kinases, serving as key kinases and central nodes in intracellular signaling pathways. This family comprises four isoforms: JAK1, JAK2, JAK3, and TYK2. Each isoform performs multiple functions, and inhibition of JAKs can achieve therapeutic effects for related diseases.
First-generation JAK inhibitors were launched overseas in 2011. Due to their broad binding profile across JAK family targets, first-generation JAK inhibitors can bind to multiple targets within the JAK family and simultaneously inhibit multiple signaling pathways. While effectively treating diseases, they also interfere with normal physiological pathways, leading to significant toxic side effects. For instance, inappropriate inhibition of JAK2 can result in thrombocytopenia and anemia.
Therefore, the FDA has issued a boxed warning for first-generation JAK inhibitors, covering risks of cardiovascular events, malignancies, thrombosis, infections, and death. Furthermore, considering that subsequent JAK inhibitor products carry similar potential safety risks, the FDA has also issued boxed warnings for all subsequently approved JAK inhibitors.
Despite carrying black box warnings, major pharmaceutical companies consider JAK inhibitors to be effective therapeutic options for many dermatological conditions, such as atopic dermatitis, psoriasis, alopecia areata, and vitiligo. This has spurred the development of second-generation JAK inhibitors. In August 2019, next-generation JAK drugs from BMS and AbbVie were approved simultaneously.
AbbVie conducted a head-to-head trial comparing its next-generation JAK inhibitor, upadacitinib, with dupilumab (Dupixent), the mainstream treatment for atopic dermatitis, and published the results in JAMA Dermatology. The findings showed that patients treated with upadacitinib experienced relief from pruritus within one week and achieved effective clearance of skin lesions after two weeks. A higher proportion of patients with atopic dermatitis attained significant levels of skin lesion clearance after 16 weeks of upadacitinib treatment. The proportion of patients achieving at least a 75% improvement in Eczema Area and Severity Index (EASI-75) was 10 percentage points higher among those treated with upadacitinib than among those treated with Dupixent.
In terms of safety, no serious adverse cardiac events or venous thromboembolic events occurred in either group. During the 16-week treatment period, the most common adverse reaction in the upadacitinib group was acne, while the most common adverse reaction in the dupilumab group was conjunctivitis.
Although second-generation inhibitors exhibit higher selectivity than first-generation agents, providing more selective inhibition of specific JAK family subtypes and significantly reducing risks related to cardiovascular events and infections, the FDA has still issued a boxed warning.
If superior efficacy under comparable safety risks is the answer sheet delivered by the new generation of JAK inhibitors, then the FDA approval of BMS’s oral TYK2 inhibitor, Sotyktu, in September 2022 marked a milestone breakthrough for JAK inhibitors—no black box warning.
Sotyktu has been approved for the treatment of moderate-to-severe plaque psoriasis in adults. Its distinguishing feature lies in its mechanism as an allosteric inhibitor that binds with high selectivity to the regulatory domain of TYK2, thereby specifically inhibiting TYK2 activity and blocking cytokine signaling pathways and immune responses associated with the pathogenesis of psoriasis. Unlike broad-spectrum JAK kinase inhibitors, it does not interact with other JAK kinases, thus avoiding adverse effects on normal physiological functions such as granulopoiesis, hematopoiesis, and lipid metabolism. With a lower risk of off-target toxicity, it fundamentally mitigates the safety concerns associated with pan-JAK inhibition.
Highly selective allosteric TYK2 inhibitors mechanistically circumvent the safety constraints associated with previous JAK inhibitors. Meanwhile, the application of deuterium technology enhances metabolic stability and reduces the formation of toxic metabolites, further ensuring drug safety. Consequently, TYK2 has attracted significant interest and strategic investment from numerous pharmaceutical companies.
Of course, not all pharmaceutical companies are solely focused on TYK2; Pfizer, for instance, has chosen to develop dual-target inhibitors to enhance therapeutic efficacy.
Pfizer’s brepocitinib is a dual JAK1/TYK2 inhibitor that binds to the active sites within the catalytic domains of TYK2 and JAK1. Currently, brepocitinib is being investigated for more than ten indications, with dermatomyositis being the most advanced, currently in Phase 3 clinical trials. Although drugs in this class are unlikely to escape the risk of a black box warning due to their JAK1 inhibition, these dual-target inhibitors still hold broad prospects if their efficacy can surpass that of previous JAK inhibitors.
The absence of a black box warning, or superior efficacy under comparable safety risks, signifies a substantial reduction in barriers to commercialization. Consequently, many multinational corporations (MNCs) have begun to comprehensively strategize their market entry, while numerous domestic pharmaceutical companies are also following suit.
With Sotyktu’s rapid market uptake in 2023, generating over $100 million in sales in the first three quarters alone, TYK2 has emerged as a hot target due to its lack of a black box warning.
According to incomplete statistics, there are currently more than 20 TYK2 inhibitors under development worldwide. For instance, in late 2022, Takeda acquired Nimbus’s TYK2 inhibitor, TAK-279, for $6 billion, with an upfront payment of $4 billion. Currently, TAK-279 has advanced to Phase III clinical trials for psoriatic arthritis.
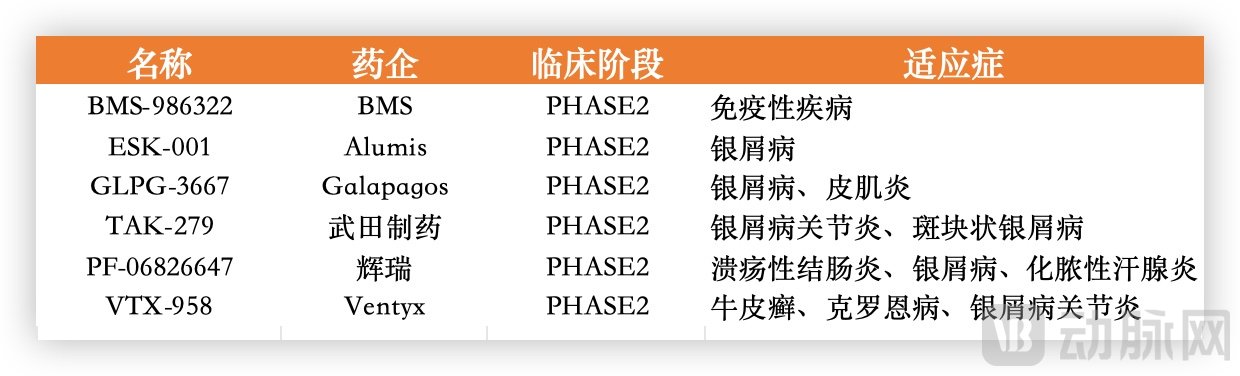
Selected TYK2 Inhibitor Programs in Development by Multinational Pharmaceutical Companies, Compiled from Public Sources
Notably, the first JAK inhibitor was approved overseas in 2011, but it took six years before it received approval for launch in China in 2017. Since then, the time gap between overseas and domestic approvals for related drugs from Pfizer, Eli Lilly, and AbbVie has been steadily narrowing. By 2023, the interval between the U.S. and Chinese approvals of Pfizer’s Litfulo was only four months.
On one hand, multinational pharmaceutical companies are aggressively expanding into the domestic autoimmune disease market; on the other hand, this trend imposes higher demands on domestic pharmaceutical firms. Whether pursuing differentiation, first-in-class (FIC), or best-in-class (BIC) strategies, it is essential to identify unmet needs within the R&D portfolios of numerous multinational corporations (MNCs) to achieve genuine innovation.
Although autoimmune disease drugs have not garnered as much attention as oncology drugs, many domestic pharmaceutical companies have still embarked on the path of exploration.
On December 17, 2023, InnoCare disclosed positive results from the Phase 2 clinical trial of its autoimmune drug candidate ICP-332 (TYK2 inhibitor) in adult patients with moderate-to-severe atopic dermatitis.
In this randomized, double-blind, placebo-controlled trial, ICP-332 demonstrated superior efficacy and safety in patients after 4 weeks of treatment, achieving multiple efficacy endpoints in the ICP-332 80 mg and/or 120 mg groups, including EASI 50, EASI 75, and EASI 90 (≥50%, 75%, and 90% improvement from baseline in Eczema Area and Severity Index score, respectively) as well as an Investigator’s Global Assessment (IGA) score of 0/1 (indicating complete or almost complete clearance of skin lesions).
ICP-332 is currently one of the most advanced TYK2 inhibitors worldwide in development for atopic dermatitis. If its safety profile can be further confirmed in subsequent clinical trials, it holds promising prospects and represents a significant milestone in China’s autoimmune drug R&D. In addition, InnoCare has another TYK2 allosteric inhibitor candidate, ICP-488, indicated for psoriasis, which is currently in Phase I clinical trials.
Highlightll Pharma’s JAK1/TYK2 inhibitor, TLL-018, reported interim analysis results from a Phase II head-to-head trial versus tofacitinib in patients with active rheumatoid arthritis at the 2023 EULAR Congress. The ACR50 response rates for the three TLL-018 dose groups were 48.0%, 65.4%, and 72.0%, respectively, exceeding the 41.7% observed with tofacitinib. In patients who had an inadequate response to tofacitinib, the medium dose of TLL-018 still demonstrated robust efficacy. TLL-018 holds promise in addressing the unmet clinical needs of this patient population.
SYHX1901, a small-molecule kinase inhibitor developed by CSPC, exhibits inhibitory activity against JAK1–3 and TYK2 kinases to varying degrees. In vitro and in vivo experimental results demonstrate potent inhibitory activity against TYK2, indicating its potential for treating various autoimmune diseases, including but not limited to psoriasis, rheumatoid arthritis, atopic dermatitis, and systemic lupus erythematosus. It is currently in Phase II clinical trials.
Furthermore, Enitiatebio’s JAK1/TYK2 inhibitor QY201 is undergoing a Phase II clinical trial for moderate-to-severe atopic dermatitis, which is being fully carried out across multiple centers in China. In July 2023, Enitiatebio received FDA approval for the Investigational New Drug (IND) application for QY201, marking its entry into the global market. Additionally, BGB-23339, a highly selective and potent allosteric TYK2 inhibitor developed by BeOne Medicines, has demonstrated highly promising activity in preclinical studies and is currently in Phase I clinical trials.
Hengrui Pharma, a leading domestic pharmaceutical company, announced on December 3, 2023, that it had received the “Notice of Acceptance” issued by the National Medical Products Administration. The company’s marketing authorization application for SHR0302 tablets, a JAK1 inhibitor, has been accepted for the treatment of adult patients with moderately to severely active rheumatoid arthritis.
Zelgen’s ruxolitinib analog, Jaktinib, has also submitted a marketing application to the NMPA, with a pipeline covering multiple indications—including intermediate- to high-risk myelofibrosis, moderate-to-severe atopic dermatitis, moderate-to-severe plaque psoriasis, ankylosing spondylitis, and severe alopecia areata—all of which are in late-stage clinical development.
Golidocitinib, developed by Dizal, has pursued a differentiated strategy by focusing on the field of hematologic malignancies. The company previously submitted a marketing application for the treatment of refractory or relapsed peripheral T-cell lymphoma (PTCL). At the 65th American Society of Hematology (ASH) Annual Meeting in 2023, Dizal announced the results of the global registration clinical trial of golidocitinib: in patients with relapsed/refractory PTCL, the median duration of response (DoR) reached 20.7 months, demonstrating durable clinical benefits compared with existing therapies. These findings were also published in the prestigious international journal The Lancet Oncology.
With increasing participation from domestic pharmaceutical companies, the Chinese market may witness a commercialization boom for new autoimmune drugs in the coming years.
As domestic pharmaceutical companies accelerate their pace in the autoimmune disease sector, multinational pharmaceutical giants such as Pfizer, AbbVie, and BMS have already begun to cultivate JAK inhibitors into blockbuster drugs with annual sales exceeding $10 billion.
Taking Pfizer’s Litfulo, which was newly approved for market launch both domestically and internationally in 2023, as an example, this innovative drug developed by Pfizer is the world’s first dual-channel inhibitor of the JAK3/TEC kinase family, indicated for the treatment of severe alopecia areata in patients aged 12 years and older. In 2018, Litfulo entered Phase III clinical trials, and alopecia areata received Breakthrough Therapy Designation from the U.S. FDA; in 2020, it also received Breakthrough Therapy Designation from China’s NMPA. Thanks to this foundation, Litfulo was approved in the United States and Japan in June 2023, and in the European Union and China in October 2023, becoming the second JAK inhibitor globally approved for the treatment of alopecia areata.
Alopecia areata is the second most common hair loss disorder, after androgenetic alopecia. Previously, treatment options for alopecia areata were limited and largely consisted of off-label use. In 2022, the FDA approved Eli Lilly’s JAK1/2 inhibitor Olumiant for adult patients with severe alopecia areata. Litfulo is currently the only medication approved for adolescents aged 12 to 18 years with alopecia areata, filling an unmet market need.
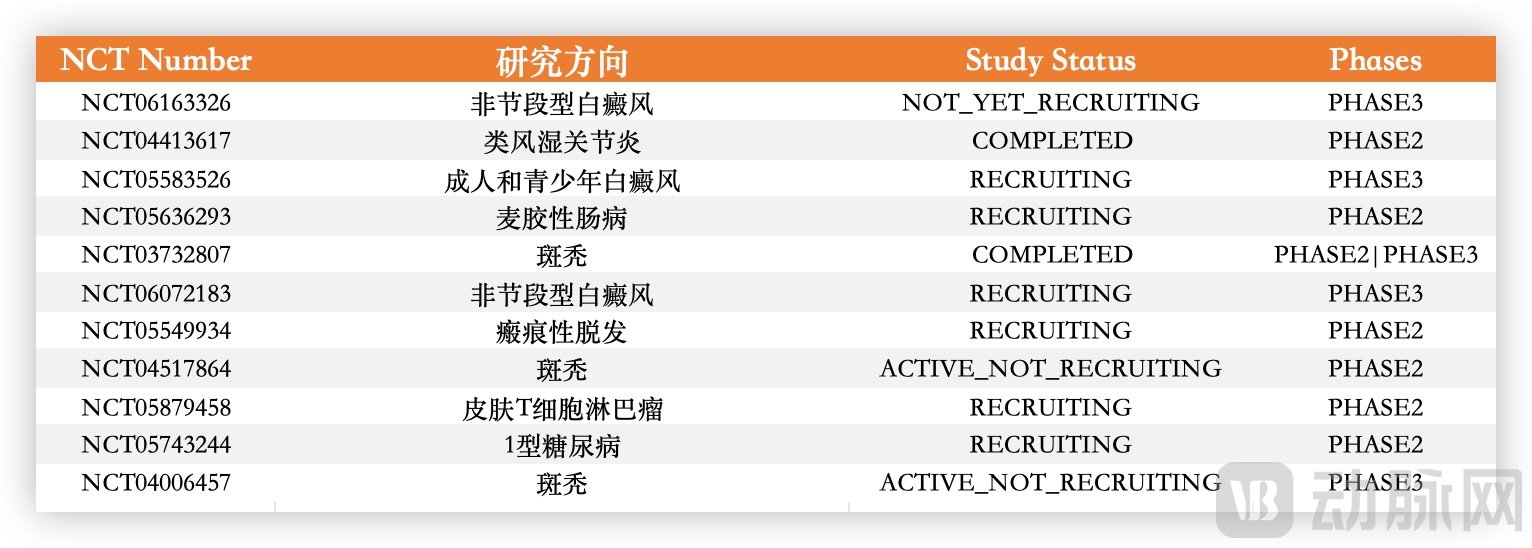
Selected Litfulo Clinical Trials, Data Sourced from ClinicalTrials.gov
Moreover, Pfizer is advancing various clinical trials for Litfulo. According to data from ClinicalTrials.gov, ongoing Phase 2 and Phase 3 studies include those for non-segmental vitiligo, rheumatoid arthritis, celiac disease, scarring alopecia, cutaneous T-cell lymphoma, and type 1 diabetes.
Given that this pertains to only one drug, Litfulo, while Pfizer’s JAK inhibitor portfolio also includes tofacitinib, abrocitinib (a JAK1 inhibitor), and the investigational brepocitinib, Pfizer should have high expectations for the future commercial prospects of its JAK inhibitors.
Not only Pfizer, but also AbbVie, the owner of the previous generation’s “blockbuster drug” Humira, places significant emphasis on autoimmune disease medications.
Against the backdrop of Humira’s patent expiration, AbbVie has proactively positioned its JAK inhibitor upadacitinib and IL-23 inhibitor Skyrizi, aiming to fully cover all former indications of Humira and achieve combined sales exceeding $15 billion within the next two years.
Since its market launch in 2019, upadacitinib has generated nearly $3 billion in revenue. This rapid revenue growth is attributable not only to AbbVie’s strong commercialization capabilities but also to the continuous expansion of upadacitinib’s indications. Starting with rheumatoid arthritis, upadacitinib has now received FDA approval for seven indications, including psoriatic arthritis in adults, moderate-to-severe atopic dermatitis, moderate-to-severe ulcerative colitis in adults, moderate-to-severe Crohn’s disease in adults, ankylosing spondylitis in adults, and non-radiographic axial spondyloarthritis.

Some Upadacitinib Clinical Trials, Data Sourced from ClinicalTrials.gov
To achieve its revenue targets, AbbVie has launched multiple clinical trials centered on upadacitinib. Data from ClinicalTrials.gov reveals strategic coverage across various conditions, including rheumatoid arthritis, vitiligo, lupus erythematosus, Crohn’s disease, hidradenitis suppurativa, and psoriasis. Notably, Phase III trials include population expansions for previously approved indications, such as extending the use of upadacitinib to younger patients with atopic dermatitis and vitiligo.
As the first TYK2 allosteric inhibitor approved for marketing globally, BMS has high expectations for Sotyktu. Multiple clinical trials registered on ClinicalTrials.gov have evaluated its efficacy in a range of conditions, including psoriasis, systemic lupus erythematosus, plaque psoriasis, psoriatic arthritis, inflammatory epigenital dermatoses, Crohn’s disease, ulcerative colitis, dermatitis, granulomatous enteritis, lupus nephritis, and lichen planus.
Based on global top-selling drugs, autoimmune therapies represent the second-largest therapeutic segment after oncology; indeed, their sales figures were nearly comparable in the 2022 Top 10 Global Drug Sales rankings. This indicates that the autoimmune market holds significant promise. Notably, among domestic pharmaceutical companies’ license-out deals in 2023, those with the highest upfront payments were almost exclusively for oncology drugs, with no autoimmune therapies featured.
According to Frost & Sullivan, the market size of autoimmune drugs in China is expected to reach approximately $23 billion by 2030, creating a significant gap between substantial market demand and insufficient R&D efforts. The explosive growth of China’s autoimmune disease market requires not only the support of multinational corporations (MNCs) but also greater participation from domestic players.
References:
DOI:10.1056/NEJMoa2306691
DOI:10.1001/jamadermatol.2023.4090
DOI:10.1016/j.autrev.2019.102390