Beyond Teleconsultation: Telesurgery Is Already on the Agenda

From Telepresence to Telesurgery
Many people are familiar with QQ video chat, which allows users to engage in lively conversations with friends from all over without leaving home. However, current video chat technologies still struggle to replicate the sensation of face-to-face, close-range interaction. Is there, then, a technology that can deliver a truly immersive experience—blurring the line between reality and virtuality—and enable communication and interaction within the other person’s environment?
In the distant United States, a 7-year-old boy named Devon appears no different from his peers. However, due to severe allergies, he must remain at home and cannot attend school like other children. Nevertheless, Devon enjoys the school experience just as much as those who can attend in person. Currently, Devon can log in to a platform at his school calledVGoa robot that allows him to communicate with classmates and teachers. The VGo robot stands 1.5 meters tall with a slender build; its “face” is a screen, its single “eye” is a camera, and its “feet” are two wheels. It can move forward at the normal walking speed of an adult, capturing surrounding visuals and transmitting them to Devon, who sits in front of a computer. Devon is utilizing a new technology known as telepresence.
So-calledTelepresence, in simple terms, it is a virtual presence that enables individuals to be present remotely in real time at a given location, known as telepresence. In this context, presence equates to “being there,” meaning you can perceive the on-site environment in real time from outside the physical location and effectively perform certain operations.
This idea can be traced back at least to the early 1980s. At that time, Marvin Minsky, one of the pioneers of robotics, coined the term “TelepresenceThe term “telepresence.” He used this word to describe a comprehensive suite of technologies that make an individual feel as if they are present in a location other than their actual physical whereabouts. Although these technologies did not fully materialize as Minsky had envisioned at the time, they have since undergone rapid development in the post-Internet era.
Later, with theTelepresenceandRemote Sensing TechnologyWith such advancements, telepresence systems have begun to enable users to move and manipulate objects. Hospitals were the first to adopt telepresence technology, primarily for remote consultations and telesurgery, with the latter being the focus of this article.
Tele-surgery is also a part of telemedicine, referring to doctors using telemedical technologies to perform surgeries on remote patients in real time from a different location, includingRemote Surgical Consultation, Surgical Observation, Surgical Guidance, SurgeryIn short, surgeons perform operations based on live video feeds transmitted from the remote site; their movements are converted into digital data and sent to the patient’s location to control local medical instruments. While this may seem far-fetched at first glance, it becomes easier to understand when one considers that many modern surgical procedures are already performed using instruments manipulated under endoscopic guidance. Essentially, it merely extends the “length” of the endoscope and instruments. Of course, such procedures demand highly sophisticated technology, integrating computer science, satellite communications, remote sensing and telemetry, holography, electronics, and other advanced technologies. In Allen’s view, this represents the future of virtual reality and internet communications in remote medical treatment.
In fact,Remote SurgeryThis is not actually a new concept. The idea of telemedicine was proposed as early as the 1970s, and the concept of telesurgery emerged in the 1980s. In the 1970s, technical experts at the National Aeronautics and Space Administration (NASA) began exploring the feasibility of using robots to perform remote surgeries on astronauts. Since then, NASA has collaborated with the military to steadily advance robotic projects capable of practically executing telesurgery. Later, with the development of telepresence technology,Mehran AnvariTo further clarify how remote robotic surgery is performed, it embarked on its first robot-assisted telesurgery, primarily aimed at helping a warrior stationed at the Aquarius underwater habitat suture a wound. However, slow communication networks, limited bandwidth, and outdated telepresence technology hindered the further advancement of telesurgery.
"Lindberg Procedure"
Now, if you are in the United States and require a prostatectomy, the procedure can be performed via remote surgery, where a surgeon uses a robotic manipulator to carry out the operation. Currently, 90% of such procedures can be completed in this manner, with scalpels effectively being used across oceans. However, in the early 20th century, this was a rather novel technology. At this point, it is necessary to introduce an individual known as the "Father of Surgical Robotics," Wang Youlun.
On February 8, 2011, the U.S. National Academy of Engineering announced the list of 68 new members and 9 foreign associates.Wang Youlunlisted among them, and he is the surgical robot “AESOP" and "ZEUS” inventor.
In the early 1980s, Academician Wang fromUniversity of California, Santa Barbara(UCSB) He completed both his undergraduate and graduate studies in Computer Engineering. At that time, he was struggling to decide on a research direction for his doctoral studies. His father, Wang Youlun’s father, was teaching at the University of California, Berkeley. Recalling this period, he mentioned that he had asked his father, in a very traditional Chinese manner, which specialized field he should focus on. After a long pause, his father uttered four words:Engineering TechnologyThe rationale is that engineering technology can integrate engineering with knowledge, leveraging science to serve humanity. Furthermore, he has been fascinated by robots since childhood, viewing them as the direction of future development and a means for computers to interact with the physical world. Therefore, it was only natural for him to pursue a Ph.D. in Computer Engineering with a focus on robotics.
Subsequently, he began to study the robotics market of the 1980s and 1990s. With funding from NASA, and through discussions and learning with Academician Wang and his physician friends, he gained an understanding ofLaparoscopic Minimally Invasive Surgery。
In the early 1990s, this industry was still in its takeoff phase. In minimally invasive surgery, physicians perform treatments inside patients’ bodies using devices such as endoscopes, allowing pathological structures to be visualized on television monitors. This technology has significantly improved the success rate of surgical procedures. Minimally invasive surgery became a central focus of computer-assisted motion research. He began researching AESOP (Automated Endoscopic System for Optimal Positioning) in 1989, and the system was successfully developed and put into clinical use in 1997.
Equipped with a laparoscope, the AESOP system later evolved into the “Zeus” surgical robot, a complete robotic system for surgical instrumentation. Subsequently, it was used to perform the world’s first telesurgery. On September 7, 2001, a professor of general surgery in Strasbourg, FranceJacques Mariscoxwith a renowned surgeon in New York, USADr. MichelleThrough collaborative efforts between the two regions, while simultaneouslyEuropean Institute for Remote Surgery Research(EITS) also provided assistance, and together they completed this world-renowned “Lindberg Surgery"-Cholecystectomy, at that time France provided special cables to reduce latency and optimize connectivity, while the US side also"computer motionThe provided surgical robot was developed through joint collaboration by both parties.
One of the bottlenecks in surgical procedures has always beenShortage of well-trained surgeonsSince the success of the “Lindbergh Operation,” it indeed sparked a significant surge in the surgical community at that time. Canadian surgeon Mehran Anvari performed more than 20 remote surgeries on patients in other locations using surgical robots, including procedures for hernias and abdominal conditions. Anvari kept his robotic system in Canada, while he remotely operated from the console at St. Joseph’s Healthcare Hamilton in Hamilton, Canada. With his hands on the control panel, he directed the robot’s use of various surgical instruments. The robot’s camera served as his eyes, enabling him to communicate with the on-site staff and issue new instructions as needed.
Telemedicine surgery, as a convergence of engineering and medical sciences, provides an excellent platform and offers hope to many patients living in remote and relatively isolated areas.
So, how exactly is remote surgery in telemedicine achieved?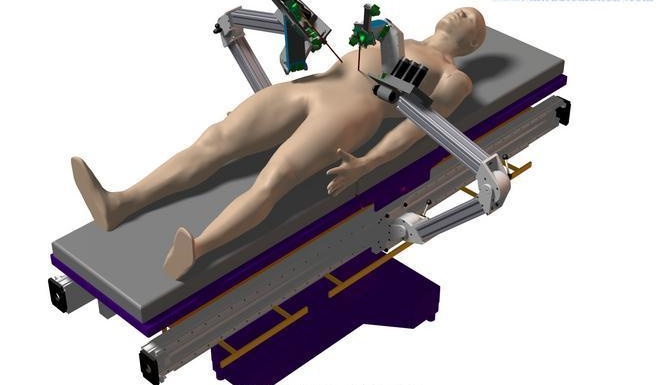
As previously mentioned, remote surgery based on the Medical Internet of Things (MIoT) is the product of integrating computer technology, communication technology, and multimedia technology with medical technology. ItInfrastructureRelatively high requirements, mainly including the following parts:
Communication Network: High-speed broadband networks provide the information transmission channel for remote surgery, transmitting on-site audio, video, and monitoring device signals via the network to the computer equipment of surgeons at a remote location, enabling them to understand the actual conditions of the surgical site. It is recommended to use a network connection withDDN, point-to-point connections can minimize line attenuation to the greatest extent. In addition, full-duplex communication should be adopted for calls between each terminal and the site, and it is preferable to use dual lines for image transmission to ensure that image transmission quality is not compromised.
Panoramic Camera: Equipped with zoom and autofocus functions; surgical equipment systems with camera support shall be compatible with image transmission systems.
Surgical Information System: Patient information can be stored digitally, intraoperative imaging data can be broadcast in real time, and retrieved on demand. On-site computers require high-speed CPUs and must be equipped with medical-grade video image acquisition cards, preferably imported ones, as domestic products currently do not meet the required standards. Terminal configurations at various locations must also be robust, particularly featuring high-performance graphics cards with large video memory.
Intelligent Mechanical Systems: The successful completion of remote surgery also requires a system precisely controlled by the central siteIntelligent mechanical systems, including robots, joysticks, or precision robotic arms. This mechanical device can fully and realistically replicate the surgical procedures performed by physicians at the central site within a virtual reality environment, in the operating room at the remote site, ensuring that the actions are accurately applied to the exact same anatomical locations on the patient’s body as in the virtual reality environment.
“Once a series of preparations are complete, should we proceed with remote surgery? Of course, it’s not that simple!”
Prior to surgery, remote consultations and surgical planning are also required. Physicians at the remote center and the distant site conduct detailed analysis and research on patient data via the Medical Internet of Things (MIoT) to formulate a detailedSurgical Plan, apply virtual reality technology for surgical planning and rehearsal to prepare potential alternatives to the primary surgical plan.
Finally, after the surgical rehearsal and alternative solutions have been fully prepared, we are ready to officially commence the remote surgery. It is quite an exciting moment. The operating surgeon is stationed at the central site, remotely controlling a robotic system located at a distant remote site to perform the procedure. The remote surgery is conducted simultaneously in a virtual operating room at the central site and the actual operating room at the remote site. The surgical subject in the former is a virtual patient reconstructed from the patient’s data. By applying virtual reality technology and precision sensing technology, the remote patient’sSpatial Perspective Image, the patient's status, posture information, and critical physiological data are transmitted to the control center and accurately displayed within a virtual image environment for the operator (surgeon).
Of course, with the development of virtual reality, surgeons now wear stylish VR headsets and use customized interfaces to perform virtual surgical procedures on virtual patient anatomy.
At this point, barring any unforeseen complications, Allen’s self-conceived remote surgery should have been successfully completed. Since we already possess the technology to perform remote surgeries, why has it not yet been widely adopted for civilian use? Below, we will examine the major obstacles hindering the implementation of remote surgery.
Remote Haptic Feedback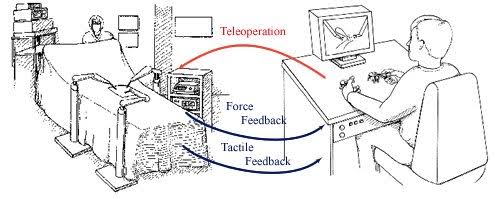
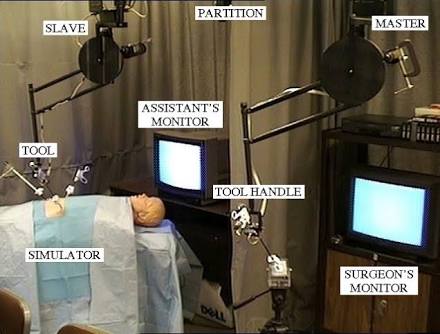
In conventional teleoperation systems, the primary concern is maintaining system stability. However, when dealing with soft tissues, the fidelity of force feedback between the robot and the environment becomes particularly critical. During surgery, geographical separation causes surgeons to lose haptic perception and operational experience, which are essential prerequisites for surgical success. Teleoperation systems are designed to restore these lost capabilities. Direct force feedback from the slave manipulator to the master controller can enhance operational dexterity. Unlike typical teleoperation systems, remote surgery demands exceptionally high levels of dexterity and fidelity. This is because surgeons rely heavily on their kinesthetic sense to perform high-precision maneuvers and detect subsurface tissue structures.
High-Speed Communication
The advantages of remote surgery are obvious, but as with any tool that relies on telecommunications technology, it also carries security risks. Communication between surgeons and robotic systems typically occurs over public networks; therefore, poor network conditions in the local area can compromise this communication.
For video gamers, latency is a common occurrence; when they move their controllers, their in-game avatars always lag by about one second. While such latency is acceptable in gaming, in real-life surgery, this brief one-second delay could very well cost a patient their life.
Take, for example, a physician manipulating vascular structures based on images displayed on a screen. If they are not accustomed to the associated time latency, they may believe they have moved to the correct distance; however, in reality, their movements may be too rapid, potentially leading to accidental puncture of arteries or organs.
"If you are a surgeon and experience a delay during an operation, to what extent can you tolerate the situation before the procedure fails and the delay renders the intervention unsafe?"
Hospitals have previously conducted remote surgery simulation tests, revealing that experienced surgeons can operate safely within a latency range of 200 milliseconds and can adapt to latencies between 200 and 500 milliseconds. If the latency exceeds 500 milliseconds, there are too many uncertainties. Therefore, on the other hand, the success of the surgery is also closely related to the surgeon.
Medical Robot Hacking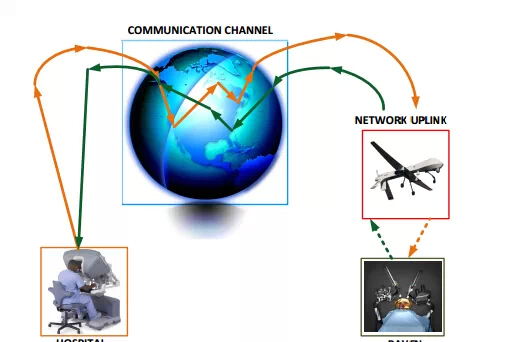
The robot itself is based onLinuxControl software on such open-source systems. It can be accessed via standard communication protocols (such asInteroperable Telesurgery Protocol) Connect to the remote control panel.
This connection is based on the public internet, making it potentially accessible to anyone. Furthermore, as the robot is designed for extreme environments, the quality of the network connection may be poor and may even rely on wireless connectivity.
This creates a risk. Due to the uncontrollable nature of network connections, malicious intruders can easily block, interfere with, or even hijack the network connection between surgical robots and surgical procedures.
Researchers at the University of Washington in Seattle have simulated how a malicious intruder could interfere with the behavior of surgical robots. They used the Raven II, which features dual robotic arms, and operated it through a state-of-the-art console that supports video transmission and haptic feedback. The team attempted three types of attacks: deleting, delaying, and scrambling the operator’s commands; altering the intent of control signals; and taking full control of the robot. All these attacks were successfully executed with ease.
The researchers also pointed out that the video images captured by the robot are publicly accessible, allowing anyone to view the footage in real time.
Encrypting the communication between robots and consoles could prevent many types of attacks. However, as we all know, even the most sophisticated security systems can sometimes be exploited by hackers who find vulnerabilities. As for what level of safety in remote surgery is acceptable, this clearly requires difficult choices to be made by doctors, policymakers, and the public. To avoid surgical procedures turning into a real-life version of Saw, all parties must immediately prioritize this issue.
Authorization and Liability
Licensing and liability remain among the primary obstacles to remote surgery. Taking the United States as an example, since medical licenses are issued by individual states, can a surgeon in Florida perform remote surgery on a patient in Texas? The internet has achieved interconnectivity across states, but does this mean that physicians must obtain medical licenses from all 50 states?Business LicenseCan surgery be performed?
Medical Disputes
Remote surgery may also give rise to medical disputes. If remote surgery accelerates a new wave in the healthcare industry, it will immediately trigger a series of new issues. For instance, where should these services be provided? Who should oversee them? If errors occur during certain steps of the medical procedure, or if an unqualified physician performs remote surgery, which court should conduct the investigation, and which hospital should bear liability? Indeed, no country has enacted specific regulations governing remote surgery, and most legal enforcement systems are unprepared to address medical procedures performed by physicians across national borders.
Employment
Beyond certain technical challenges, the large-scale adoption of remote surgery in real-world settings could significantly impact employment. Imagine a public hospital that extensively employs robotic systems for remote surgeries: it would cease hiring many skilled surgeons and instead raise the selection criteria for surgical staff. Consequently, less competent surgeons who previously secured positions through various channels would face the risk of unemployment.
The aforementioned situation has already occurred inIndustrial SectorIt has happened; however, due to the higher barriers to entry in medicine compared with ordinary industrial manufacturing, there remains a certain buffer period. Nevertheless, from both technological and economic perspectives, these developments are inevitable.
Matt Beane, a researcher in remote technology at the Massachusetts Institute of Technology (MIT) in the United States, pointed out that one remote worker can oversee 10 stores and 30 robots. As early as June 2011, Terry Gou, CEO of Foxconn Technology Group, announced plans to deploy one million robots. It is reported that a particular production line at Foxconn previously employed 20–30 workers; however, after introducing robots, the workforce on that line was immediately reduced to five. These remaining employees are only required to press buttons and operate the machines.
Cost
As previously analyzed in our introduction to the da Vinci surgical robot, the latest generation of the da Vinci system is priced at approximately25 millionapproximately. In addition to the cost of the main unit, this figure includes taxes, training fees, and clinical technical support fees. When costs are amortized per procedure, robotic surgery is approximately RMB 30,000 more expensive than traditional surgery. Furthermore, the costs associated with surgeries performed using the da Vinci Surgical System are currently not covered by national health insurance schemes in various countries, which imposes certain limitations on the application of remote surgery. Previously reported cases, such as a remote cataract surgery costing £30, were primarily made possible through self-funding by charitable organizations. For the general public, health insurance coverage remains a more critical concern.
How Far Away Is Remote Surgery?
In September this year, a hospital in Florida successfully conducted an online test to verify the feasibility of remote robotic surgery.
It is reported that during the test, the operating surgeon was located at a distance from the hospital.Over 1,200 miles, utilizing networked remote-controlled surgical robots to perform operations on simulated patients (not real patients, but virtual patient simulators). Subsequently, the hospital in Florida plans to extend the distance further, enabling physicians located as far away as Denver, California, or even Rome to remotely operate surgical robots for procedures.
Through these tests, they determined that remote surgery is feasible within the United States. Nationwide network latency has been significantly reduced and is no longer a limiting factor for remote robotic surgery. Furthermore, during this test, the hospital in Florida used the da Vinci Surgical System, which is currently the most common robotic surgical equipment worldwide.
Based on past experience, a prerequisite for a technology to deliver practical applications to society is that the military has fully developed it, adopted it for its own use, and demonstrated its value in military environments. Although remote surgery may not yet have entered the civilian market on a large scale, its future applications are highly anticipated. It can connect doctors in urban areas with patients in remote regions. If we imagine a more science-fiction scenario, you could even provide surgical services to astronauts in space.
Given China's large population and the highly uneven distribution of economic development and medical resources, forRemote SurgeryThe demand is becoming even more urgent. It is believed that with the implementation of the 13th Five-Year Plan and the development of the Medical Internet of Things, more people will benefit from the convenience brought by telemedicine.