Surgical Robots Reshaping Traditional Healthcare: A 30-Year Evolution and Product Overview
The Navy General Hospital pioneered stereotactic brain surgery in China, with the specific procedures consistentlyYesPerformed manually by physicians. According to neurosurgeons at the hospital’s Neurosurgery Center, the rationale for deploying robots to replace manual procedures is based on four considerations: first, robotic positioning offers greater precision and reduces human error; second, robots can perform hazardous tasks on behalf of medical staff, such as injecting radioactive isotopes; third, robotic systems enable shorter positioning times, higher accuracy, and minimal trauma; and fourth, robots allow for preoperative simulation of surgical maneuvers and selection of the optimal surgical approach.
The outcomes of robot-assisted surgery were also highly favorable. The pediatric patient experienced a recurrence of craniopharyngioma three years after undergoing craniotomy under general anesthesia, with the tumor measuring 3×3×2.5 cm. This subsequent surgical procedure lasted only 45 minutes. Upon leaving the operating room, the patient’s headache and symptoms of elevated intracranial pressure were immediately relieved, and vision returned to normal. The patient was able to consume milk two hours postoperatively without any complications.
Traditional surgical procedures involve physicians using medical instruments to excise and suture pathological lesions in patients. These operations entail local manipulation of the human body with tools such as scalpels, scissors, and needles to remove diseased tissue, repair injuries, transplant organs, and improve function and morphology. In some surgeries, patients endure significant suffering, such as incisions extending over ten centimeters in length and complete transection of muscles. Large incisions imply severe trauma, substantial blood loss, and a heightened risk of infection. The primary objectives behind the development of surgical robots are to alleviate patient suffering, enhance surgical precision, and reduce procedural risks.

Timeline of the Emergence of Historically Significant Surgical Robots

Surgical robots were developed much earlier abroad, with the first application of a surgical robot dating back to 1985. Physicians at Los Angeles Hospital in the United States performed a robot-assisted stereotactic neurosurgical brain biopsy using the Puma 560. In fact, the Puma 560 was not a dedicated surgical robot; it was an articulated industrial robotic arm. This marked the first use of robotic technology in medical surgery, representing a groundbreaking milestone. However, due to safety concerns, the manufacturer of the robot initially prohibited its use in surgical procedures.

Medical robots specifically designed for surgical procedures emerged in the early 1990s, with ROBODOC being a representative example. In 1986, IBM’s Thomas J. Watson Research Center in the United States collaborated with the University of California to develop this technology. Integrated Surgical Systems was established in 1992 and launched ROBODOC, the first surgical robot approved by the U.S. Food and Drug Administration (FDA). This robot is capable of performing total hip replacement, hip revision and reconstruction, and knee replacement surgeries. During hip replacement procedures, it achieves a femoral preparation accuracy of 96%, compared to only 75% for manual techniques performed by surgeons.

The surgical robots that truly embarked on the path to commercialization were the AESOP series developed by the U.S. company Computer Motion—a voice-controlled “camera-holding” robotic arm operated by surgeons to prevent image instability caused by the physiological fatigue of human camera holders.
In the early 1980s, Youlun Wang, hailed as the father of surgical robots, completed his undergraduate and graduate studies in Computer Engineering at the University of California, Santa Barbara (UCSB). At that time, he was contemplating the direction of his doctoral research. Having been fascinated by robotics since childhood, Wang viewed robots as the future trajectory of development and a means for computers to interact with the physical world. Consequently, he decided to pursue a Ph.D. in Computer Engineering (with a focus on Robotics) at UCSB.
Subsequently, he began to study the robotics market of the 1980s and 1990s. Fortunate to receive funding from NASA, he started leveraging these resources to examine robotic demands across various industries. Through conversations with physicians, Wang Youlun gained insights into laparoscopic minimally invasive surgery. In the early 1990s, this field was still in its nascent stage of rapid growth. In minimally invasive procedures, surgeons perform treatments inside patients’ bodies using devices such as endoscopes, allowing pathological structures to be visualized on television monitors. This technology significantly improved the success rate of surgical operations. Minimally invasive surgery became the core focus of Computer Motion.Wang Youlun began researching “AESOP” (Automated Endoscopic System for Optimal Positioning) in 1989 and successfully developed it in 1997.
This robot can mimic the functions of the human arm and enable voice-controlled settings, eliminating the need for assistants to manually control the endoscope. It provides more precise and consistent camera movements than manual control, offering surgeons a direct and stable field of view. In 1997, AESOP performed its first laparoscopic surgery in Brussels, Belgium. AESOP became the first FDA-approved robotic system for debridement procedures. By 2014, surgeons using AESOP had performed over 75,000 minimally invasive surgeries worldwide.

By 1998, AESOP was equipped with laparoscopic capabilities and gradually evolved into the ZEUS system. Capable of remote operation, it constituted a complete robotic surgical instrument system. The ZEUS system comprises a Surgeon-side component and a Patient-side component. The Surgeon-side system consists of a pair of master controllers and monitors, allowing the surgeon to operate the master handles while seated and view the patient’s internal anatomy captured by the endoscope on the console displays.
The patient-side unit consists of two robotic arms for positioning and one robotic arm for controlling the endoscope’s position. The surgeon can operate the laparoscopic arm via voice commands while simultaneously manipulating the other two robotic arms to perform the surgery. The Zeus system demonstrated its minimally invasive advantages in a fallopian tube reconstruction procedure, requiring only a few small incisions, each about the diameter of a chopstick, on the patient’s abdomen for the insertion of the endoscope and robotic arms.

On September 7, 2001, renowned surgeon Jacques Marescaux, based in New York, and Dr. Michel, a distinguished surgeon also in New York, collaborated remotely to perform a cholecystectomy on a 68-year-old female patient in Strasbourg, France, using the Zeus system. The entire procedure lasted only 48 minutes; the patient resumed fluid drainage within 48 hours postoperatively, with no complications. Professor Marescaux regarded this milestone as the third revolution in surgical history, following minimally invasive techniques and computer-assisted applications, successfully introducing the concept of “global sharing of surgical technology,” enabling surgeons to participate in operations anywhere in the world, regardless of their physical location.
This groundbreaking procedure was dubbed the “Lindbergh Operation.” Although the surgery was successfully completed, latency in image transmission and surgical manipulation posed significant challenges, making remote surgery difficult to achieve. However, with increasing internet speeds, latency in modern telesurgery will undoubtedly be improved.

The da Vinci Surgical System is currently the most successful and widely used surgical robot worldwide. Developed by Intuitive Surgical in 1999, it has since released four generations of products. Representing the highest level of contemporary surgical robotics, the system primarily consists of three components: the surgeon’s console, the 3D vision system, and the patient-side cart equipped with robotic arms, an endoscopic camera arm, and surgical instruments. During surgery, the operating surgeon does not have direct physical contact with the patient; instead, they control the procedure through a 3D visual system and motion-scaling technology, enabling the robotic arms and surgical instruments to precisely replicate the surgeon’s technical movements and operative maneuvers.
Apart from Zeus, other surgical robots that were nearly on par with it technologically at the time were also well utilized. AESOP once achieved the remarkable feat of assisting in tens of thousands of surgeries annually, and ROBODOC was adopted in multiple countries and regions across North America, Europe, Asia, and Oceania. In 2000, the da Vinci Surgical System officially received FDA clearance, becoming the first endoscopic surgical robot to be FDA-cleared. Although AESOP and Zeus entered the market earlier, their failure to secure FDA approval hindered their market penetration. Following a patent dispute in 2003, Computer Motion, the company behind Zeus, merged with Intuitive Surgical, the developer of da Vinci. As a result, da Vinci became the only FDA-cleared surgical robot on the market, effectively monopolizing the global surgical robotics market—a situation that has persisted to this day.
The more advanced da Vinci system not only requires minimal incisions but also transmits high-definition 3D video via its endoscope, creating an immersive sense of presence for the lead surgeon as if they were inside the patient’s abdomen. Its digital zoom function enables magnification of the surgical field by more than 10 times without further advancing the instrument into the patient’s body. Anatomical structures and tissue layers are rendered with exceptional clarity, thereby enhancing precision during surgery.
Don’t conventional endoscopic procedures also allow surgeons to feel “immersed” in the surgical field? In fact, they are quite different. First, endoscopy deprives surgeons of the intuitive, direct manipulation of instruments while failing to provide true 3D stereoscopic vision. Second, laparoscopic techniques are far more challenging than anticipated, with a steep learning curve. The da Vinci Surgical System expands surgeons’ visual fields and, through its 3D imaging, compensates for the lack of depth perception inherent in 2D flat images. Moreover, although the da Vinci system stands nearly two meters tall, it offers exquisite precision capable of handling an embroidery needle. A viral online video once showcased its remarkable dexterity by demonstrating the suturing of a grape’s skin inside a glass bottle, astonishing viewers worldwide.
Like the human arm, the da Vinci robotic arm features three joints: the shoulder, elbow, and wrist. However, the range of motion in the human shoulder, elbow, and wrist is quite limited; once these limits are reached, movements must be readjusted. In contrast, the three joints of the da Vinci system can move freely in all directions—up, down, left, and right. Most remarkably, the da Vinci system boasts a 7-degree-of-freedom “EndoWrist.” Although only 0.5–0.8 cm in diameter, it is significantly more dexterous than the human hand.
The human hand can flip up and down by a maximum of 180 degrees, whereas the da Vinci surgical system’s wrist can rotate freely through 540 degrees, enabling it to bend and rotate with ease within the narrow confines of the human thoracic and pelvic cavities to perform actions such as grasping, cutting, suturing, and knot-tying.
Moreover, the da Vinci system’s instruments are not limited to a single design. To meet the diverse demands of surgical procedures, the da Vinci “hands” come in a wide variety of types. Ultrasonic scalpels, electrocautery knives, scissors, forceps, hooks, and more are employed for thoracotomy, suturing, hemostasis, and other tasks, while traditional surgical instruments take a back seat as secondary options.
Although surgeons possess exceptional technical skills, they are human and cannot overcome the physiological tremor of their arms. The da Vinci system filters out these unnecessary tremors, leveraging the stability of machinery to maintain a safer and more precise state throughout the surgical procedure. With the assistance of the da Vinci system, the highest goals of surgery are being progressively achieved: smaller incisions, reduced trauma, less bleeding, and diminished vascular injury. Taking the prostate as an example, which is located deep within the body at the junction of the urethral orifice and the bladder, traditional open surgery requires large incisions. In contrast, the da Vinci system only requires several small ports approximately 1 cm in size, resulting in significantly less blood loss. This greatly reduces patient blood loss and postoperative pain, markedly shortens hospital stays, and facilitates postoperative recovery. In fact, in the United States, over 90% of radical prostatectomies for prostate cancer are performed with robotic assistance.
More importantly, robotic assistance has made surgeries for patients with infectious diseases easier and safer. For instance, patients with HIV/AIDS often suffer from compromised systemic immune function, making them poorly tolerant of major open surgeries; the da Vinci Surgical System effectively overcomes this limitation. Furthermore, during traditional surgical procedures, physicians must adhere to extensive protective measures, which can impair both visibility and tactile feedback, and may fail to prevent infection in certain emergency situations. In contrast, robotic surgery is conducted entirely within the patient’s abdominal cavity, substantially minimizing the risk of viral transmission through blood and bodily fluids, thereby ensuring physician safety.
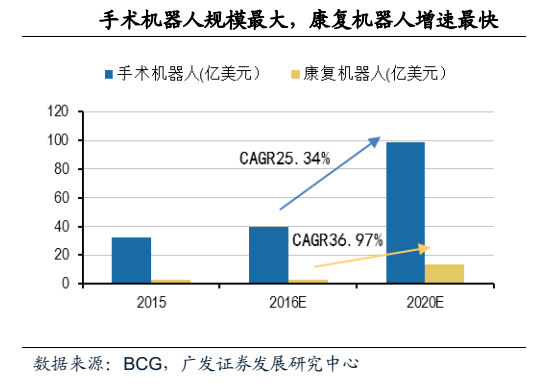
Among the four categories of medical robots—rehabilitation robots, surgical robots, bionic prosthetics, and behavioral assistance robots—surgical robots boast the broadest development prospects. Since their emergence in the 1980s, with accelerated growth beginning in 2000, surgical robots have captured the largest share of the medical robot market, accounting for approximately 60%. The global market sales value for surgical robots was estimated at $4 billion in 2016 and is projected to reach approximately $10 billion by 2020.
While the da Vinci surgical system offers numerous benefits, its high usage costs and procedural prices constitute its most significant drawbacks. Due to its monopolistic position, the initial batch of da Vinci systems sold in China commanded a staggering price of RMB 25 million per unit, with the second batch priced at RMB 18 million; procurement costs after 2015 may be slightly lower. In contrast, the selling price in the United States is only RMB 10 million per unit, and even in South Korea and Japan, the prices are lower than those in China.
In addition to the high purchase price of the machine itself, consumables and maintenance costs are also extremely expensive. Da Vinci surgical forceps cost RMB 40,000–50,000 per unit; three units are typically used per surgery, and they must be replaced after ten uses. When insurance, maintenance, and other costs (RMB 1.5 million per year) are factored in, the cost of Da Vinci surgeries allocated to patients becomes prohibitively high. Currently, patients in China incur an additional out-of-pocket expense of approximately RMB 30,000–40,000 for Da Vinci procedures, which are not covered by medical insurance. In contrast, the cost of such surgeries in the United States is approximately USD 100,000 per procedure. Although consumable prices there are only one-third of those in China, the majority of the cost comprises professional service fees for physicians and nurses.
In the United States, the da Vinci Surgical System has become widely adopted. With over 2,200 units installed across more than 5,000 hospitals nationwide—including community hospitals—any hospital of considerable scale is virtually certain to be equipped with a da Vinci system.
In addition to the U.S. domestic market, another major market is Europe, which was also the first market pioneered by the da Vinci surgical system. Before obtaining FDA clearance, the da Vinci robot had already secured CE marking from the European Union, thereby gaining access to the European market. Compared with the U.S. market, the European market still holds significant potential for growth.
In China, however, the situation is entirely different, no matter how remarkable the da Vinci system may be.
Since the introduction of the first da Vinci surgical robot by the PLA General Hospital (301 Hospital) in 2006, the da Vinci system has been present in China for a decade. However, as the da Vinci surgical robot is classified as a Class III medical device, its adoption by any hospital in China requires direct approval from the National Health and Family Planning Commission (NHFPC), resulting in a consistently slow rate of introduction. To date, the total installed base in mainland China remains under 60 units, making it a scarce resource.
As of June last year, there were a total of 3,398 da Vinci surgical robots worldwide, with approximately 383 in Asia and around 2,295 in the United States. In China, the installed base reached 42 units by December of last year, up from only 17 units in 2013. According to the plan at that time, at least 36 new installations were to be completed over the following three years, meaning that the installed base in mainland China would reach at least 53 units by 2016. Da Vinci surgical robots distributed across China have performed 11,445 procedures, bringing the cumulative total number of surgeries performed to date to 22,917.

With a population of 1.3 billion and 7 billion medical consultations recorded over 14 years, China presents a significantly larger demand potential for medical robots compared to the United States. In the absence of insurance coverage, independent research and development (R&D) is undoubtedly the most direct means of reducing the cost of robotic surgery. To address the high purchase prices of equipment and the scarcity of procurement quotas, some institutions have embarked on the independent R&D of surgical robot systems. After several years of exploration and collaborative efforts, the goal of localizing surgical robots in China is drawing nearer. Currently, domestically produced surgical robot systems are at a critical stage of R&D and are expected to be launched within the next few years.
Verb Surgical:Verb Surgical was jointly founded by Verily, the life sciences division of Alphabet (Google’s parent company), and pharmaceutical giant Johnson & Johnson. The venture aims to build a platform that integrates robotics, advanced imaging, machine learning, big data, and cutting-edge instruments, enabling physicians to perform both open and minimally invasive procedures. In other words, their goal is to provide doctors with greater flexibility. Physicians can use Verb Surgical for specific steps of a surgical procedure or throughout the entire operation, as needed. Both Google and Johnson & Johnson place significant emphasis on big data. According to a financial analyst, recording and analyzing procedural data through big data technologies can truly enable the replication of robotic surgical procedures, thereby facilitating their broader adoption.
Medtronic:Medtronic, founded in 1949, is a Fortune Global 500 company. In 1957, Medtronic manufactured the first portable external cardiac pacemaker, and in 1960, it produced the first reliable implantable cardiac pacing system, thereby establishing its position as a global leader in pacing technology. Today, Medtronic has become a world-leading medical technology company, providing lifelong solutions for patients with various chronic diseases. Medtronic announced its aim to launch a surgical robot by mid-2018, with initial deployment in India.
TransEnterix:TransEnterix is a Canadian surgical robotics company. It originally planned to further develop the SurgiBot surgical robot based on its previous product, the “SPIDER” minimally invasive laparoscopic surgical system (SPIDER Surgical System), but this effort was rejected by the U.S. Food and Drug Administration (FDA). The company subsequently shifted its focus to the ALF-X surgical robot, acquired through its nearly $100 million acquisition of Italy’s SOFAR in 2015. Recently, TransEnterix sold its first unit to a hospital in Milan, Italy. Compared with the da Vinci Surgical System, TransEnterix’s device is more affordable and offers features not available in the da Vinci system, such as eye-tracking software and haptic feedback.
Titan Medical:Titan Medical, a Toronto-based company, is developing the Sport Surgical System, which integrates an operating table, a single-incision camera, and multi-articulated instruments, with a U.S. launch scheduled for 2017. The Titan robotic system aims to refine robotic surgery, enabling procedures on minute anatomical structures, including cholecystectomy.
Medrobotics:Medrobotics’ Flex Robotic System provides a robotically assisted visualization system for laryngeal surgery, enabling greater flexibility and ease of operation. The system allows the robotic platform to access anatomical regions that are difficult or impossible for surgeons to reach, thereby helping patients with laryngeal conditions alleviate their symptoms.
CRAS:The CRAS robotic system, jointly developed by the Navy General Hospital and Beihang University, is a pioneer among domestic surgical robotic systems and has completed the development and clinical application of its sixth generation. The system employs PUMA 260 and 262 robots as the executive mechanisms for assisted operations. The first-generation robot was first applied in clinical practice in May 1997. The second generation, successfully developed in 1999, achieved frameless stereotactic surgery. In addition to incorporating the features of the previous four generations, the fifth-generation robot features more advanced automatic positioning capabilities, including visual automatic positioning, which minimizes surgical errors and makes procedures faster and safer. The system enables remote surgical operations via the Internet. On December 12, 2005, two stereotactic surgeries were successfully performed remotely between Beijing and Yan’an using the Internet. Nevertheless, the CRAS surgical robot still faces many challenges that need to be addressed in terms of expanding its scope of application and practicality.
Minimally Invasive Laparoscopic Surgical Robot System:Developed by the Robotics Institute of Harbin Institute of Technology (HIT), the system has passed acceptance review by the expert panel of China’s National “863” Program. According to R&D personnel at HIT’s Robotics Institute, this domestically produced minimally invasive laparoscopic surgical robot system possesses independent intellectual property rights in China. Researchers have achieved significant breakthroughs in key technologies—including mechanical design, master-slave control algorithms, three-dimensional (3D) laparoscopy, and system integration—tailored to various minimally invasive surgical procedures, and have filed multiple national invention patents. This achievement is regarded as breaking the technological monopoly held by the imported da Vinci Surgical System, thereby accelerating the adoption of domestically developed robotic assistance in minimally invasive surgeries.
"Miaoshou S" Surgical Robot:The “Miaoshou S” robot, jointly developed by Tianjin University, Central South University, and other institutions with independent intellectual property rights, successfully completed three surgeries at the Third Xiangya Hospital of Central South University, marking the successful implementation of the first domestic robotic surgery in China. “Miaoshou S” is a minimally invasive surgical robot system with independent intellectual property rights developed by Tianjin University, featuring three technical advantages over similar foreign products. First, it employs a multi-degree-of-freedom wire transmission decoupling design for minimally invasive surgical instruments, resolving motion coupling issues while ensuring fixation, anti-slip, and anti-loosening properties, thereby better maintaining precision. Second, it achieves reconfigurable layout principles and implementation technologies for the master manipulator, making the robot’s “arms” lighter and more adaptable to surgical needs. Third, it utilizes heterogeneous isomorphic control model construction technology to ensure consistency among hand, eye, and instrument movements in a stereoscopic visual environment. It is reported that the “Miaoshou S” surgical robot system is expected to enter production within three years.
NSRS:The Hong Kong Polytechnic University has successfully developed the NSRS, the world’s first robotic system specifically designed for surgery with built-in motors. This research leveraged the surgical clinical expertise of the Li Ka Shing Faculty of Medicine at the University of Hong Kong and has been successfully applied in animal experiments. The technology is expected to enter clinical trials within two years, with a market launch as early as 2019. Featuring motor-driven robotic arms, the system can access the human body through a single incision or natural orifices to perform various abdominal or pelvic surgeries. With its precise operation and excellent force feedback, the system marks a new chapter in the field of minimally invasive surgery.
The “2016 World Medical Robot Conference,” hosted by the World Association of Medical Robotics, is scheduled to take place in Shenzhen, China, on October 29–30. This inaugural global summit integrates scientific research, clinical practice, and industry development in the field of medical robotics. The event will be attended by more than 20 academicians from various countries, along with dozens of presidents of renowned hospitals and clinical experts worldwide who will deliver reports and participate in discussions. Experts and scholars from prestigious domestic and international institutions—including the Swiss Academy of Technical Sciences (SAWT), the UK Royal Academy of Engineering, the Chinese Academy of Sciences, the Singapore Academy of Medical Sciences, and the ROBO Medical Robotics Institute—will share insights on global application trends and research directions in medical robotics. They will conduct thematic discussions centered on the conference theme: “Technological Innovation Transforming Healthcare, Health Leading the Future.”

Venue: Wuzhou Hotel, Shenzhen, China
No. 6001, Shennan Avenue, Futian District, Shenzhen
Conference Dates: October 29–30, 2016
{kind=link}
Click the link below or scan the QR code to register. For investment and sponsorship inquiries, please contact Peipei at VCBeat (WeChat ID: xiaopeiling185025).

Related Reading:
“2016 World Medical Robot Conference” – Get the Latest News First
Growth Rate Reaches 34.45%, Medical Robotics Industry Has a Promising Future