Japan's Controlled Drug Pricing: Strained医保 Payments and Constrained Innovative Drug Pricing
Drug pricing mechanisms are closely intertwined with medical insurance cost containment and healthcare reform. In recent years, China has explored a transition from administrative to market-oriented approaches, gradually shifting regulatory control from the “visible hand” of government intervention to the “invisible hand” of market forces. This shift has, to some extent, guided the market-based pricing of pharmaceuticals. However, challenges remain, including difficult negotiations over medical insurance reimbursement prices and insufficient incentives for original brand-name drugs. As our close neighbor across the sea, Japan exercises stricter control over the pricing of new and original brand-name drugs, potentially offering a different interpretation of the balance between administrative regulation and market mechanisms. This article is part of Huachuang Securities’ series on observations of Japan’s biopharmaceutical sector, republished with permission by VCBeat.
Unlike the free-market pricing model in the United States, drug prices in Japan have long been under government control. This approach has enabled the government to leverage drug pricing as a tool to steer industry policies and exert a degree of regulatory control over the growth of pharmaceutical expenditures and total healthcare costs. However, it has also overlooked the inherent market mechanisms of the pharmaceutical sector. With the continuous emergence of high-cost drugs and mounting financial pressure on the national health insurance system, Japan’s pricing framework is now facing significant pressure for reform. As China prepares to implement its new National Reimbursement Drug List (NRDL) along with a supporting mechanism for setting insurance payment standards, this issue of “Japan Pharmaceutical and Biotech Industry Watch” focuses on the valuable lessons and insights that can be drawn from Japan’s experience as a pioneer in this field.
Highlights of This Issue
1. The current drug pricing mechanism, primarily based on relative pricing, has reached a bottleneck.
Japan’s universal, inclusive healthcare system is built upon a government-led national health insurance scheme. To ensure the proper functioning of this insurance system for a population of 127 million, the Japanese government has implemented strict controls on the growth of pharmaceutical expenditures by leveraging the drug pricing mechanism as a key intervention point, thereby curbing the rise in total health expenditure. In practice, the current drug pricing mechanism, which primarily adopts relative pricing, has largely achieved its stated objectives of controlling the growth of both drug costs and total health expenditure. However, this regulatory approach, akin to a planned economy, overlooks the market-oriented nature of pharmaceutical products and has significantly hindered the further development of Japan’s pharmaceutical industry. The dilemma of “expecting the horse to run fast while feeding it little” highlights the critical challenge facing the Japanese government and the current drug pricing mechanism: how to stimulate the market dynamics of pharmaceuticals while continuing to safeguard their public welfare attributes.
2. How Japan, with Its Inflated Drug Prices, Will Undertake Reform.
Japan’s current new drug pricing mechanism has inflated the launch prices of new medications. Even with biennial price adjustments intended as a corrective measure, this system has contributed to the persistently high overall pharmaceutical expenditures. In horizontal comparisons among developed countries, Japan’s drug prices remain far from affordable; given that Japan does not adopt a free-market pricing mechanism akin to that of the United States, describing these prices as artificially inflated is not an exaggeration. With shifts in disease patterns and demographic structures, the continuous emergence of high-cost therapeutic agents and the prolongation of treatment durations are expected clinical trends. It is evident that Japan’s current new drug pricing mechanism, which primarily relies on relative pricing, has reached a bottleneck and will inevitably need to transition toward a reform based on absolute cost calculation.
Main Text
I. The Current Drug Pricing Mechanism, Dominated by Relative Pricing, Has Reached a Bottleneck
As comprehensively elaborated in the first report of our series, Japan’s universal healthcare service system is built upon a national health insurance scheme predominantly led by the government. To ensure the proper functioning of this insurance system covering a population of 127 million, the Japanese government has implemented strict controls on the growth of pharmaceutical expenditures by leveraging the drug pricing mechanism as a key entry point, thereby curbing the rise in total healthcare spending. In terms of outcomes, the current drug pricing mechanism, which primarily adopts relative pricing methods, has indeed effectively achieved its established goals of controlling the growth of both drug costs and total healthcare expenditures. However, on the other hand, this regulatory approach, akin to a planned economy, overlooks the market-oriented attributes of pharmaceutical products and has significantly hindered the further development of Japan’s pharmaceutical industry. The dilemma of “expecting the horse to run fast while feeding it little” highlights the critical challenge facing the Japanese government and the current drug pricing mechanism: how to stimulate the market dynamics of pharmaceuticals while continuing to safeguard their public welfare nature.
(I) Universal Health Insurance System and Drug Price Formation Mechanism
The emergence and evolution of Japan’s drug pricing mechanism are inextricably linked to the establishment and operation of its universal health insurance system. In the early stages of the health insurance system, which was established in 1927, drug prices were determined entirely by market supply and demand, and the insurance system implemented a uniform fixed-amount reimbursement for all oral medications. It was not until after World War II, with the lifting of “postwar price controls” on pharmaceuticals and many consumer goods, and the gradual maturation of the universal health insurance system, that the drug pricing mechanism—which determines total pharmaceutical expenditure and constituted the largest portion of insurance payments at the time—was naturally incorporated into the policy framework of the health insurance system. The codified embodiment of this mechanism is the Drug Price Standard, which has been in use since the 1950s and remains in effect today.
Chart 1 Overview of Japan’s Health Insurance System

Source: Huachuang Securities
Building on the initial drug price survey, the first edition of the Drug Price Standard was officially promulgated and implemented by the then Ministry of Health and Welfare on September 1, 1950, marking the prototype of the current Drug Price Standard. However, it differed slightly from the current drug pricing mechanism. At that time, the Drug Price Standard served more as a reference catalog; it listed market prices for drugs to provide guidance for insurance organizations in setting reimbursement rates, rather than directly listing reimbursement prices as it does today. Meanwhile, drugs not included in the catalog could still be reimbursed on an actual-expense basis through health insurance.
With the further improvement of the national health insurance system, more standardized requirements have been put forward for the varieties and prices of drugs eligible for reimbursement. This is the primary reason for the introduction of the current *Drug Price Standards* in 1957, which incorporate both drug variety and pricing attributes. On one hand, the drugs listed in the *Drug Price Standards* constitute the complete list of medicines eligible for health insurance reimbursement; drugs not included in the list, as well as medical treatments outside the approved indications of the listed drugs, are not covered by health insurance payments. On the other hand, the drug prices stipulated in the *Drug Price Standards* serve as the unified national reimbursement prices, thereby formally establishing a price ceiling for pharmaceuticals. The formal implementation of the current *Drug Price Standards* marks an important first step in Japan’s health insurance system toward emphasizing the public welfare nature of pharmaceuticals, setting the tone for subsequent drug policy developments.
Subsequently, the Japanese government implemented a series of adjustments to the detailed implementation rules of the “Drug Price Standards.” These measures included shifting the scope of drug price surveys from retail endpoints, such as hospitals and pharmacies, to wholesale endpoints, such as pharmaceutical manufacturers and wholesalers, and changing the classification of listed drugs from generic names to brand names. Notably, the new drug pricing method established in 1982, which was primarily based on relative pricing, formally laid the foundation for the current drug price formation mechanism and exerted a profound influence on the subsequent development of the pharmaceutical industry.
Chart 2 History of the Current Drug Pricing Mechanism
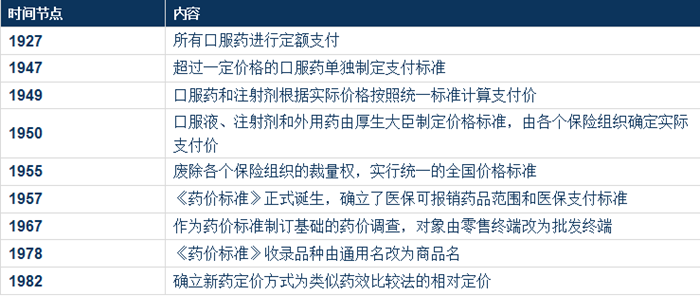
Source: Huachuang Securities
(II) Overview of the Current Drug Price Formation Mechanism
The “Drug Price Standards” cover only prescription drugs whose intended use is not for prevention or life-saving purposes, excluding in vitro diagnostic reagents, vaccines (with certain exceptions such as hepatitis B vaccine), low-dose contraceptives, and medications for erectile dysfunction. Compounded medications prepared by pharmacies are also excluded. Unlike in China, all over-the-counter drugs are entirely excluded.
Figure 3 Scope of Drugs Covered in the "Drug Price Standards"

Source: Huachuang Securities
Drug listing methods are also categorized into two types: listing by brand name and listing by generic name. As mentioned in the previous section, after 1978, the vast majority of drugs were listed in the National Health Insurance (NHI) Drug Price Standard under their brand names, while drugs listed by generic name were limited to those included in the Japanese Pharmacopoeia, vaccines, and traditional Chinese medicine decoction pieces. The primary reason for shifting from generic-name listing to brand-name listing in the NHI Drug Price Standard was that, with the rise of generic drugs in the late 1970s, significant price disparities emerged among drugs with the same active ingredient produced by different pharmaceutical companies. Only by refining the listing from generic names to specific brand names could the true market prices of these products be adequately reflected, thereby narrowing the gap between the NHI reimbursement price and the actual market price for individual products. At the same time, brand-name listing objectively shifted the core competitiveness of pharmaceuticals from price back to quality. However, it must also be noted that brand-name listing principally benefits originator pharmaceutical companies and does not help narrow the price gap between originator drugs and generics. This laid the groundwork for a series of drug pricing reform policies introduced in Japan over the past decade to increase the market share of generic drugs. Currently, if calculated entirely by brand name, the latest 2016 edition of the NHI Drug Price Standard includes a total of 18,948 types of drugs; if calculated partially by generic name, the number of listed products decreases to 15,925.
Figure 4 2016Comparison of the Number of Drugs Included in the Latest Edition of the "Drug Price Standards"
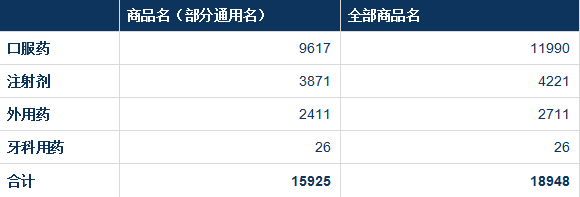
Source: Huachuang Securities
The inclusion process for the National Health Insurance (NHI) Drug Price Standard consists of three major stages: market approval, drug price determination, and formal inclusion, with drug price determination being the most critical step. In principle, all drugs approved for marketing in Japan, except those excluded from the NHI Drug Price Standard, are automatically eligible for inclusion within 60 days (no later than 90 days) after receiving market approval. During this 60-day period, the drug pricing body under the Central Social Insurance Medical Council (hereinafter referred to as “Chuikyo”), established by the Ministry of Health, Labour and Welfare, must complete the determination of the NHI reimbursement price for the drug and submit it to Chuikyo for record-keeping. Subsequently, originator drugs are formally included in the NHI Drug Price Standard through four annual inclusion windows (March, June, September, and December), while generic drugs are included through two annual windows (June and December). Furthermore, pharmaceutical companies must complete the market launch and sales of the drug within three months of its formal inclusion in the NHI Drug Price Standard. This requirement aims to prevent extreme scenarios where certain generic drug manufacturers cease production and sales based on market prices after their products have qualified for NHI reimbursement.
Chart 5 Procedure for Including Newly Approved Marketed Varieties in the "Drug Price Standards"

Source: Huachuang Securities
As mentioned in the first installment of our series on Japan’s health insurance system, Japan adjusts the National Health Insurance (NHI) reimbursement prices downward every two years, based on drug price surveys conducted in the preceding year, to curb the growth of pharmaceutical expenditures and total healthcare spending. These adjustments apply to all drugs listed in the NHI Drug Price Standard. As a critical tool for narrowing the gap between the NHI reimbursement prices and actual market prices for drugs included in the NHI Drug Price Standard, drug price surveys hold significant importance. These surveys are conducted through two approaches—passive and active surveys—with no difference in the surveyed entities, which primarily consist of distributors, healthcare institutions, and pharmacies. In passive surveys, surveyed entities report the actual market prices of drugs to the Ministry of Health, Labour and Welfare (MHLW) in the autumn of the year preceding an even-year price adjustment, covering a broader scope. In contrast, active surveys involve the MHLW proactively querying surveyed entities about prices on an irregular basis, offering greater flexibility in timing and methodology. Currently, results from passive surveys serve as the primary basis for downward adjustments to NHI reimbursement prices. Historical data from large-scale passive surveys indicate that since 2000, the price gap between NHI reimbursement prices and actual market prices has remained relatively stable, fluctuating around 8–9%.
Chart 6 1993-2013Drug Cost Share and Price Differentials in Japan by Year

Source: Huachuang Securities
As shown in Chart 6, the total pharmaceutical expenditure exhibits a pattern of “higher in odd-numbered years and lower in even-numbered years,” corresponding to the overall reduction in National Health Insurance (NHI) reimbursement prices for drugs during even-numbered years. The growth momentum of the drug cost ratio has also been curbed to some extent, remaining stable at approximately 22% over the past two decades. However, the total pharmaceutical expenditure has not declined; instead, it has shown an upward trend. This phenomenon is partly attributable to the intensifying “super-aged” demographic structure in Japan, and partly closely related to the current drug pricing mechanism in Japan, which adopts a relative pricing approach for most new drugs.
Chart 7 2000-2016The Impact of Annual Drug Price Reductions on Drug Expenditures and Total Health Expenditures

Source: Huachuang Securities
(3) The Increasingly Expensive Pricing Mechanism for New Drugs
Newly launched drugs included in the National Drug Price Standard have their medical insurance reimbursement prices determined through different pricing methods, depending on the availability of reference drugs and the degree of innovation. However, in general, Japan’s drug pricing mechanism has largely relied for over three decades on a relative pricing approach. In particular, for the pricing of originator drugs, this method involves referencing similar products with equivalent efficacy, thereby providing a certain level of price protection for originator drugs. As a result, although originator drugs under patent protection account for only 18.0% by volume in the current National Drug Price Standard, they represent as much as 55.9% of sales revenue. When including originator drugs that have passed their patent protection period, all originator drugs collectively account for 44.1% by volume and 80.8% by sales revenue.
Chart 8 Market Share of Products Listed in the Latest Edition of the "Drug Price Standards" (Inner Ring: Quantity, Outer Ring: Value)

Source: Huachuang Securities
Newly launched drugs follow different pricing procedures depending on whether reference products with similar efficacy exist. Even when relative pricing based on reference drugs is applied, the markup varies according to the degree of innovation. For new drugs without reference products, absolute cost-based pricing is adopted.
Chart 9 Flowchart of the Pricing Mechanism for New Drugs

It is relatively straightforward to distinguish whether newly launched drugs adopt relative or absolute pricing methods; one simply needs to examine whether there are already marketed products with similar therapeutic efficacy available on the market. The more complex aspect lies in drugs priced using the relative pricing method, where the degree of innovation is assessed separately against seven interrelated yet relatively independent criteria. The determination of these seven criteria is directly linked to the outcomes of seven drug price markups, which constitute the “supplementary markup” applied to certain varieties with a higher degree of innovation under the relative pricing framework.
Chart 10 Seven Items“Specific Details of the ‘Supplementary Markup’”
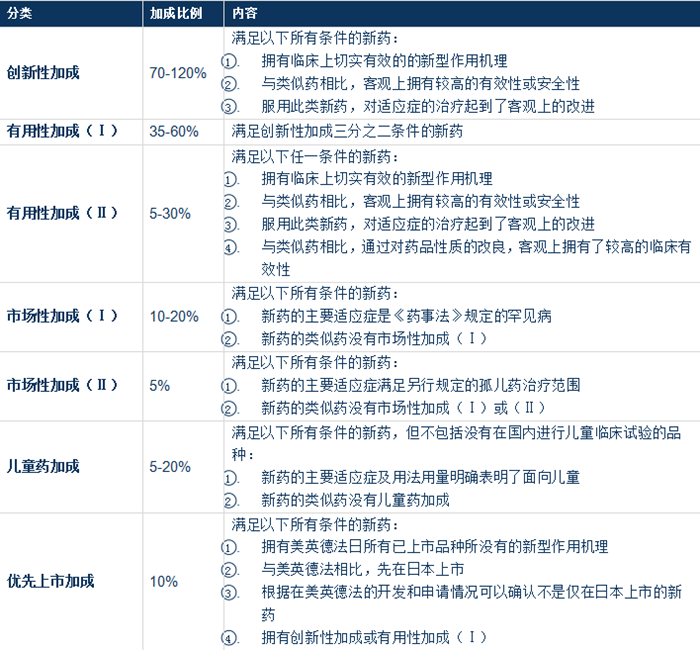
Source: Huachuang Securities
As can be seen from the detailed description of “supplementary add-ons” in the table above, if drugs are classified into originator and non-originator categories, most originator drugs are ultimately priced using the higher-innovation tier within the relative pricing method, while a small minority adopt the absolute pricing method based on cost calculation. In contrast, new non-originator drugs basically derive their final National Health Insurance (NHI) reimbursement price from the lower-innovation tier within the relative pricing method. Importantly, since drug pricing for new medicines in Japan predominantly employs a relative pricing method based on the average daily cost of reference drugs, coupled with various “supplementary add-ons,” the prices of new drugs invariably remain higher than those of reference drugs. This is an objective factor contributing to the persistently high drug prices in Japan.
In addition to the “supplementary markup,” new drug prices undergo two rounds of adjustments before being finalized: international average price adjustment and dosage-form adjustment. As the name suggests, international average price adjustment involves comparing the price of a new drug with the average market price of the same product already launched in four countries—the United States, the United Kingdom, Germany, and France. Adjustments are mandatory if the price exceeds 125% or falls below 75% of this benchmark. Dosage-form adjustment refers to first determining the price for the commonly used dosage strength, which then serves as the basis for setting prices for less common dosage strengths.
Following the aforementioned add-ons and adjustments, the final drug prices, together with the brand names of new drugs, are formally incorporated into the *Drug Price Standard*, which is revised periodically on an annual basis. However, as previously noted, price adjustments do not end there, nor can pharmaceutical companies rest easy. The biennial collective reduction of national health insurance reimbursement prices for drugs, conducted in even-numbered years, acts like a tight constraint, dampening the enthusiasm of pharmaceutical companies for research and development innovation. To maintain Japan’s status as a leading nation in original research and development (R&D) drugs, safeguard the innovative drive of originator pharmaceutical companies, and reduce off-label use, Japan introduced an innovation add-on mechanism for originator drugs during each price adjustment starting in 2012. Under this mechanism, the current drug price for originator drugs remains unchanged during the period before generic versions enter the market; a one-time price reduction is applied only after the generic drugs are officially launched.
(4) A Non-Discriminatory Pricing Mechanism for Generic Drugs
Unlike new drugs, the pricing mechanism for generic drugs can be described in four Chinese characters as “simple and crude.” Approved generic drugs have two opportunities each year, in June and December, to be included in the Drug Price Standard. In principle, their prices are uniformly set at 60% of the current price of the originator drug. However, for generic drugs with the same active ingredient where more than 10 varieties are already listed in the Drug Price Standard, the inclusion price is further reduced to 50%. Of course, before the final drug prices are established, there is also a specification adjustment mechanism similar to that for new drugs, but overall, it has little impact on drug prices.
Furthermore, unlike generic chemical drugs, biosimilars cannot skip the clinical trial phase prior to market approval. Consequently, a pricing mechanism of 70%/60% has been adopted for biosimilars: if there are fewer than 10 biosimilar products, the price is set at 70% of the current price of the originator drug; if there are more than 10 biosimilar products, the price is set at 60% of the current price of the originator drug.
Chart 11 Schematic Diagram of Generic Drug Pricing Mechanism

Source: Huachuang Securities
(5) Limitations of the Current New Drug Pricing Mechanism
Relative pricing based on the average daily cost of reference drugs with similar efficacy, while safeguarding the profit margins of originator drugs to some extent, has inadvertently inflated the launch prices of new drugs. Once blockbuster products such as monoclonal antibodies and molecular targeted therapies enter the market, the risk of a sharp increase in the financial burden on medical insurance is evident. Furthermore, including improved drugs within the scope of new drugs has, to some degree, contributed to artificially high launch prices. Sumitomo Dainippon Pharma once marketed zonisamide tablets, an antiepileptic drug, with a national health insurance reimbursement price of 38.5 yen per 100 mg tablet (in 2009). The company subsequently launched a product with the same active ingredient as a new drug indicated for Parkinson’s disease. Because the reference drug was an anti-Parkinson agent and a 5% utility add-on (Category II) was applied, the reimbursement price surged to 1,084.9 yen per 25 mg tablet—112.7 times higher than its price when indicated for epilepsy.
Similarly, the launch of a new drug with the same active ingredient but administered via a different route often leads to artificially inflated prices, a phenomenon that underscores the limitations inherent in the current comparative pricing mechanism for new drugs.
II. How Will Japan, with Its Inflated Drug Prices, Undertake Reform?
As previously articulated, Japan’s current drug pricing mechanism for new medicines has elevated their launch prices. Even with biennial price adjustments serving as a corrective measure, this system has contributed to the persistently high overall pharmaceutical expenditure. In horizontal comparisons among developed countries, Japanese drug prices remain far from inexpensive; particularly given that Japan does not adopt a free-market pricing mechanism akin to that of the United States, it is not an exaggeration to describe these prices as artificially inflated. With shifts in disease patterns and demographic structures, the continuous emergence of high-cost therapeutics and the prolongation of treatment durations are anticipated clinical trends. It is evident that Japan’s current new drug pricing mechanism, which relies primarily on relative pricing, has reached a bottleneck. Consequently, future reforms will inevitably need to shift toward an absolute cost-based calculation approach.
(I) Japan’s Not-So-Cheap Drug Prices
The Japan Federation of National Health Insurance Associations conducted two cross-country comparisons of drug prices between Japan and four other countries—the United States, the United Kingdom, Germany, and France—in 1995 and 2010. The results showed that in 1995, Japan’s drug prices ranked highest among major developed countries. Although they declined slightly by 2010, Japanese drug prices remained second only to those in the United States and were substantially higher than those in Germany, France, and the United Kingdom. As a country with regulated drug pricing, such price levels can only be described as artificially inflated.
Chart 12 Comparison of Drug Prices Between Japan and Major Developed Countries

Source: Huachuang Securities
From the perspective of specific disease areas, chronic conditions where Japanese pharmaceutical companies hold certain technological advantages in original drug development are the most severely affected by inflated drug prices. Antidepressants (SSRIs), antihypertensives (ARBs), and hyperlipidemia treatments rank as the top three, with prices ranging from 1.66 to 2.02 times the average prices in the other four countries.
Figure 13 Comparison of Drug Prices in Japan and the Average of Major Developed Countries by Therapeutic Area

Source: Huachuang Securities
(II) Where Is Reform Headed?
In summary, Japan’s current drug pricing mechanism, which adopts a relative pricing approach for new drugs, places excessive emphasis on relative fairness among prescription drugs for the same indication while neglecting the inherent cost structure of the medications. This has resulted in the current chaos of artificially inflated drug prices and has failed to assist the Japanese government in further controlling the overall growth of pharmaceutical and healthcare expenditures. It is evident that the existing drug pricing mechanism has reached a critical juncture where reform is imperative, with the pricing methodology for new drugs being the primary target. Significant transformations are underway across all aspects, from the definition of new drugs and their automatic inclusion in the reimbursement list to their pricing methods. Among these changes, absolute pricing based primarily on cost calculations—although it accounted for only 22% of new drugs included in the Drug Price Standard over the past five years—is expected to become the mainstream approach in the future. This shift represents a major transformation for the pharmaceutical industry ecosystem, suggesting that Japanese pharmaceutical companies will face increasingly challenging operating conditions.
Editor’s Note: This article marks the final installment of Huachuang Securities’ series on Japan’s pharmaceutical and biotechnology industry. We will continue to deliver high-quality research reports in the future. You are welcome to follow VCBeat (www.vcbeat.top) and its WeChat account (vcbeat).
Series Report Directory
Issue 1: Decoding Japan’s Universal Health Insurance System: A Sweet Burden Under the Pressure of an Aging Population
Part II: The Current State of Japan’s Pharmaceutical Distribution Industry: Bearing the Burden Under the Shadow of Cost Containment
Phase III: Traditional Chinese Medicine in Japan: Annual Output Value of Only 10 Billion, with Only One Listed Company
Episode 4: Japanese Drug Prices Under Government Control: Strained Health Insurance Reimbursements and Constrained New Drug R&D Pricing