Hidden Pain Points in China's Healthcare Reform: When Will Pharmacists Gain Prescribing Authority?

Separation of prescribing from dispensing, reduction in the proportion of drug costs, tiered diagnosis and treatment, telemedicine, the two-invoice system, and adjustments to medical insurance payment—healthcare reform has introduced key terms across every segment, from pharmaceutical manufacturing and distribution to diagnosis and treatment. The lifting of restrictions on pharmacists’ prescribing authority, a mere ripple submerged in the tidal wave of healthcare reform, has rarely drawn attention.
Data on the 2016 National Licensed Pharmacist Qualification Examination, released by the Licensed Pharmacist Qualification Certification Center of the China Food and Drug Administration (CFDA), showed that the number of applicants and those who passed the exam in the previous year were 884,700 and 151,100, respectively, with a pass rate of 20.74%. The number of applicants for the licensed pharmacist examination has remained above 800,000 for three consecutive years, and the pass rate has also increased significantly.
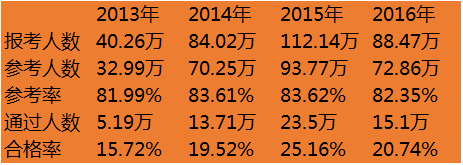
In fact, since 2013, there has been a significant upward trend in both the number of applicants for and the number of individuals passing the Licensed Pharmacist Qualification Examination, driven by a surge in demand for licensed pharmacists from pharmaceutical distribution and retail enterprises. The industry widely attributes this trend to the impetus provided by the Good Supply Practice (GSP) for Pharmaceutical Products. This regulation mandates that the legal representative or person in charge of a pharmaceutical operating enterprise must hold a licensed pharmacist qualification, and that enterprises must staff licensed pharmacists in accordance with national regulations to be responsible for prescription review and guidance on rational drug use. Specifically, pharmaceutical wholesale enterprises are required to employ at least two registered licensed pharmacists on staff, retail pharmacies must have at least one licensed pharmacist, and standalone pharmacies are required to have two licensed pharmacists covering both traditional Chinese medicine and Western medicine.
This policy rapidly created a shortage of licensed pharmacists. In response, pharmaceutical distribution and retail enterprises implemented incentive measures, such as “paid study leave for exam preparation,” “examination registration subsidies,” and “salary increases upon passing the exam,” which drove a sharp rise in the number of applicants for the licensed pharmacist examination. Meanwhile, it also spurred training institutions to capitalize on this market, leading to strong demand for training materials and preparatory courses for licensed Chinese and Western medicine practitioners.
In fact, such a shortage was inevitable. Currently, there are more than 440,000 retail pharmacies and over 10,000 pharmaceutical distribution enterprises in China, while the number of registered licensed pharmacists stands at only around 320,000, resulting in a shortfall of more than 100,000. Relevant authorities have taken note of this situation and allowed for a transition period, extending the deadline to 2020.
Currently, the average number of registered licensed pharmacists per 10,000 people in China is 2.2. The target set by the National Drug Safety Plan during the 13th Five-Year Plan period was 4, indicating a potential for twofold growth. However, when benchmarked against the international standard of 6.2 licensed pharmacists per 10,000 people, as reported by the International Pharmaceutical Federation (FIP) across 82 countries, the shortfall would be even more significant.
On one hand, there is a significant shortage of licensed pharmacists; on the other, there is a stark disparity in the treatment and compensation they receive across hospital systems versus pharmaceutical distribution and retail enterprises. Outpatient pharmacists have long been marginalized, as patients place insufficient emphasis on medication safety and contraindications. Consequently, medication consultation clinics established within hospitals remain underutilized, contributing to several medication safety incidents. Relevant surveys also indicate that patients tend to follow physicians’ recommendations exclusively. However, medications prescribed by different physicians often involve drug interactions and contraindications, necessitating unified oversight by pharmacists.
In this context, new perspectives have emerged regarding the prescription privileges of licensed pharmacists in hospital outpatient departments and retail pharmacies. With respect to the definition of prescription authority, the Measures for the Administration of Prescriptions stipulate that a prescription is a medical document issued by registered licensed physicians and assistant licensed physicians for patients during diagnosis and treatment activities, which is then reviewed, dispensed, and verified by pharmaceutical professionals who have obtained professional technical qualifications in pharmacy, and serves as proof of medication for patients. In other words, only physicians have the authority to prescribe medications in China; pharmacists do not currently hold prescription rights. Pharmacists possess the authority to verify prescriptions, but this responsibility is often reduced to a cursory review, leaving pharmacists with no choice but to “dispense medications strictly according to the prescription.”
With the goals of ensuring medication safety and promoting rational drug use, pharmacists should not be confined to the simplistic task of dispensing medications based solely on prescriptions. Instead, they should leverage their pharmaceutical expertise to provide professional insights and recommendations regarding therapeutic regimens. Furthermore, they should be empowered to participate in disease diagnosis, offer medication advice, and hold limited prescribing authority. It is important to note that pharmacists’ prescribing privileges must be restricted in terms of prescriber eligibility, prescription models, conditions, and content, with specific requirements set for professional tenure and academic titles. Specifically, pharmacists’ prescribing authority should focus on simple cases such as minor ailments, common diseases, chronic conditions, and follow-up visits. The establishment of a “micro-prescription” catalog, akin to the Over-the-Counter (OTC) drug list, should also be considered.
This approach does not disrupt the existing balance of division of labor between physicians and pharmacists; rather, it aims to better leverage medications to meet patients’ diagnostic, treatment, and rehabilitation needs, enhance medication safety and precision, and improve the accessibility of medications for minor and chronic conditions through retail and other channels. Precedents for this practice exist abroad.
One is the UK's "nurse prescribing rights" and "pharmacist prescribing rights"This exploration began in 1992, when the UK Parliament passed the Nurses’ Prescribing Regulations, granting prescribing authority for dressings, medical devices, and a limited range of prescription medications to registered nurse practitioners. Since then, the National Health Service (NHS) has continuously pursued reforms to expand prescribing rights. In 2006, training programs for pharmacists were launched; through relevant training and under physician supervision, pharmacists undergo a series of certification processes and ultimately obtain prescribing authority for most medications, excluding controlled drugs. Starting in 2008, the UK Department of Health explicitly proposed that pharmacists play a greater role within the healthcare system, including the management of minor conditions such as colds, simple gastrointestinal disorders, and skin diseases.
The second is the U.S. model of protocol-based prescribing, under collaborative practice agreements in the United States, pharmacists and physicians may negotiate to prescribe certain medications, and in some cases, clinical pharmacy specialists may even prescribe independently. In the U.S., prescribing pharmacists are certified by their respective healthcare institutions and authorized to provide medication therapy management services; however, this differs from the prescribing authority granted to pharmacists in the United Kingdom. In the UK, pharmacists who obtain qualification as supplementary prescribers are recognized across all secondary and primary care settings. Some U.S. pharmacists have long been prescribing for patients as part of their medication therapy management services, accumulating considerable experience in their relationships with physicians and in service development. The UK also drew heavily on U.S. experience when formulating laws governing pharmacist prescribing.
Third is Canada's limited prescription modelAs a close neighbor of the United States, Canada shares many similarities with the U.S. regarding pharmacists’ prescribing authority. Canadian health authorities stipulate that pharmacists may obtain prescribing privileges for certain chronic diseases upon approval by the health department. The conditions for prescribing include: the presence of a chronic disease, prior treatment by a physician, stable condition requiring only continuation of existing medication therapy, and the requirement that prescriptions be uploaded for physician review.
Conditions for pharmacists to obtain prescribing authority and the scope of their prescribing privileges vary across countries, primarily due to differences in national contexts. From a broader perspective, the United Kingdom, with its universal healthcare system, grants partial prescribing rights to nurses and pharmacists mainly for “cost containment within the healthcare system.” In contrast, the United States and Canada have adopted such measures primarily to improve accessibility to medications at the primary care level and to supplement medical resources to a certain extent.
Guided by the concept of “learning from others’ experiences,” some voices are calling for China to grant pharmacists prescription privileges, drawing on models such as collaborative practice agreements and limited prescribing authority. The rationale behind this proposal is that the current pharmaceutical distribution landscape has changed significantly compared to the past, particularly with the rise of internet healthcare and e-pharmacy, as well as growing public demand for proactive health management, which have placed higher requirements on pharmaceutical distribution and retail.
From a pharmacy business perspective, sales were previously dominated by over-the-counter (OTC) products, with prescription drugs accounting for less than 30% of the total. Against the backdrop of the broader separation of prescribing and dispensing, restrictions on the outflow of prescriptions have been lifted, inevitably leading to a substantial increase in prescription drug sales through retail channels. This trend necessitates enhanced prescription management capabilities at pharmacies. In addition to increasing the number of pharmacists and improving their professional competency, granting limited prescriptive authority would also afford greater autonomy in their workflow.
Another notable phenomenon is that some retail pharmacies are beginning to transform into multi-service providers, aiming for models such as “pharmacy + clinic,” “smart pharmacy,” and “health service points.” In particular, the pharmacy-clinic model enables simple initial and follow-up consultations within pharmacies by introducing remote consultation equipment and integrating with online hospitals. This approach not only drives incremental foot traffic to pharmacies but also generates growth in prescription volume. To effectively handle the increase in prescriptions, primarily electronic ones, pharmacies must have adequate capacity. If on-site pharmacists possess diagnostic capabilities and prescription authority, they can better coordinate with remote medical services, thereby facilitating more effective consultation and medication management.

Global Active Exploration of Pharmacist Prescribing Authority
Regarding “tiered diagnosis and treatment,” a centerpiece of healthcare reform, the coverage of pharmaceutical retail outlets is already very high, meeting the standard of one store per 3,000 people. In urban central areas, there are several pharmacies every two to three kilometers. Introducing primary care consultation services into these pharmacies could serve as a supplement to primary healthcare and effectively alleviate the patient burden on large hospitals.
Secondly, there is the pharmaceutical e-commerce sector, which has developed very rapidly in recent years. By the end of December, more than 800 enterprises held licenses for online drug trading, and the transaction volume of pharmaceutical B2C reached RMB 20 billion, with continued rapid growth expected. However, pharmaceutical e-commerce has not yet resolved the issue of prescriptions. Since B2C pharmaceutical e-commerce relies on physical pharmacies as its qualification basis, granting partial prescription rights to resident pharmacists would significantly boost the development of pharmaceutical e-commerce.
In summary, from the perspective of pharmacists’ functions, their essential role is to assist patients in selecting appropriate medications, compensate for physicians’ gaps in pharmaceutical knowledge and awareness of drug contraindications, manage adverse drug reactions, ensure medication safety, and develop rational medication plans for patients to achieve precision therapy and cost control. However, under the impetus of healthcare reforms—such as the separation of prescribing and dispensing, the outflow of prescriptions from hospitals, and tiered diagnosis and treatment systems—pharmacists must gradually adapt to new models in the pharmaceutical industry. Furthermore, with the development of internet-based healthcare, pharmacists with prescription privileges are needed to provide recommendations for the treatment of minor ailments and chronic diseases. Therefore, pharmacists should play a more significant role in the process of diagnosis and medication management, ensuring that their authority aligns with professional requirements.